
Abstract
Introduction:
Human hydatidosis, being caused by the larvae of Echinococcus granulosus, rarely presents as disseminated peritoneal disease which can be either primary or secondary. Iatrogenic secondary peritoneal echinococcosis is more common while primary form of infection is found occasionally. Radiological imaging including ultrasonography or computed tomography (CT) scan is considered the most essential diagnostic modality. The mainstay of treatment for localized hydatid cysts or infected cysts and multiple septations is the surgical management in the form of excision. Disseminated hydatid disease presents with varied manifestations involving multiple organs. However, primary peritoneal hydatidosis is being rare entity, accounting for only 2% of cases of abdominal hydatidosis. The dissemination to multiple organs usually occurs through either lymphatic or systemic circulation.
Case Report:
In this case report, we present an uncommon presentation of primary disseminated peritoneal hydatidosis. On further evaluation, the patient was diagnosed to have peritoneal hydatidosis with hepatic and lung hydatid cyst involvement on contrast-enhanced CT abdomen. The patient was managed conservatively with oral tablet albendazole 400 mg twice a day during his 1st admission and later presented again with acute abdomen, and then, radical surgery in the form of pericystectomy was carried out but patient developed large gastric perforation, for which again surgery was attempted, but patient succumbed to his illness. In this case, the rare presentation of primary disseminated peritoneal hydatidosis as acute abdomen was observed.
Conclusion:
Primary disseminated peritoneal hydatidosis as the presentation of acute pain abdomen is rare entity. This case emphasizes an atypical presentation of hydatidosis.
Introduction
Hydatid disease is a zoonotic infection, most commonly prevalent in Mediterranean countries, North and East Africa, Australia, and South America because of its relation to cattle grazing and poultry cultivation.[1] In India, the highest number of cases are reported in Tamil Nadu, Andhra Pradesh, Gujarat, South Maharashtra, and North Karnataka. Human hydatidosis is caused by the larval parasite of Echinococcus, and the Granulosus species predominantly, followed by the Multilocularis species. The involvement of the liver is the most common (75%), followed by the lungs (15%) and the spleen, kidney, brain, and bones are less frequently and secondarily involved.[2]
The definitive host in the Echinococcus granulosus life cycle includes the canids family, such as canines, foxes, and wolves, while the intermediate host belongs to the family of ungulates such as sheeps and dairy cattle. Humans are the accidental intermediate host [Figure 1].[3] After ingestion of food inoculated with eggs of the parasite or because of close contact with contaminated pets, the eggs reach the intestines and release oncospheres. Further, these oncospheres infiltrate the intestinal wall and enter the circulatory system through the portal circulation. They disseminate to different organs with most predominantly to the liver (75%), followed by the lungs (15%), where they transform into cysts. The scolices (the larval stage) appear in the inner germinal layer of the cysts and create an acellular laminated layer on the outside. This endocyst contains the hydatid fluid and acquires its nourishment through the pericyst. The germinal layer is required for the development of daughter cysts or the brood capsules which further produce protoscolices.
Life Cycle Echinococcus granulosus
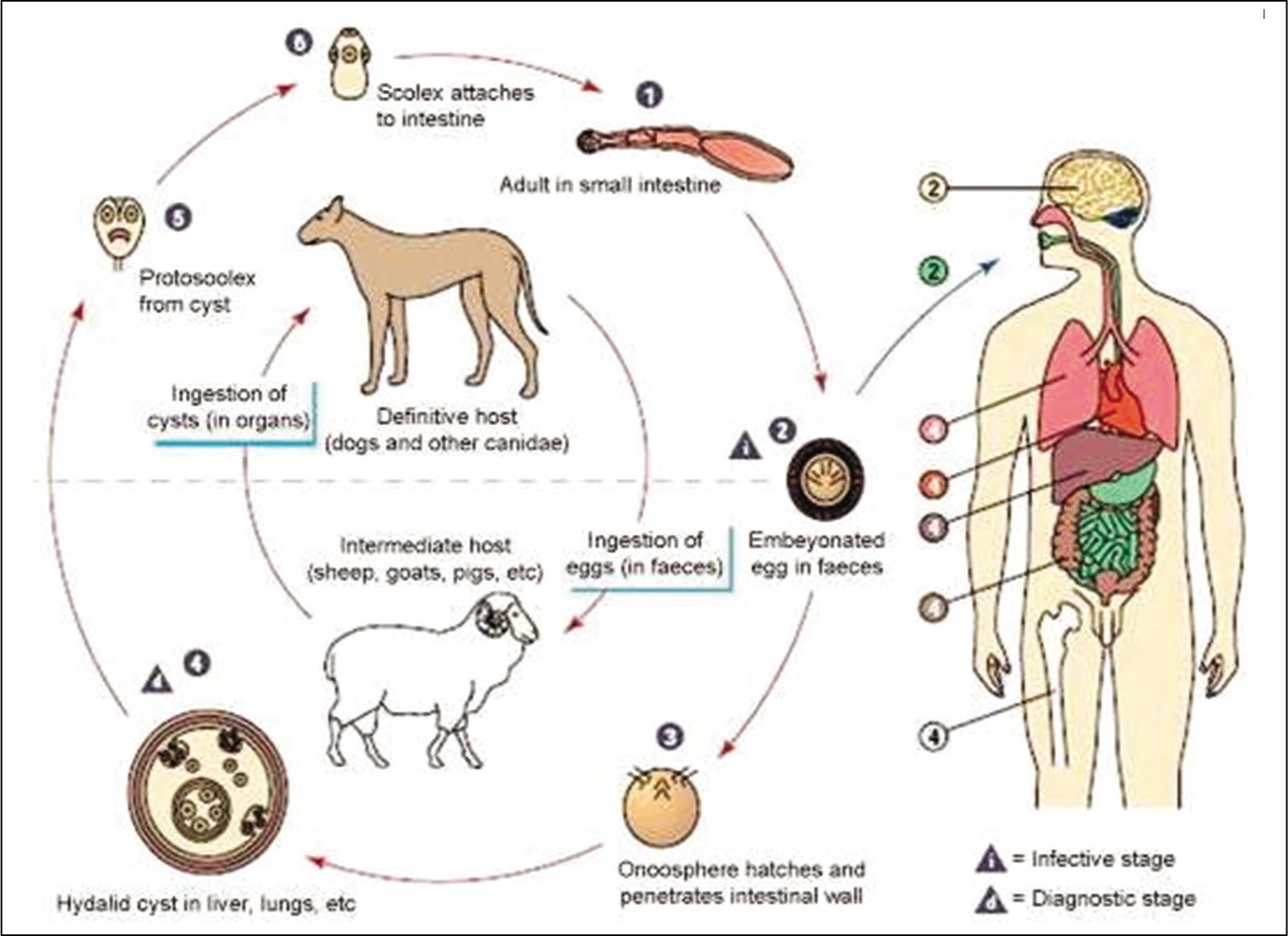
The daughter cysts are released into the bloodstream circulation, following rupture of the cysts, giving rise to the new foci.[4] Disseminated abdominal hydatidosis is uncommon with peritoneal implantation occurring as a result of traumatic or surgical rupture of the cyst (secondary type). Most of the studies have also reported that daughter or secondary cysts are causing peritoneal hydatidosis. However, primary peritoneal hydatidosis is rare and represents only 2% of instances of abdominal hydatidosis. Herewith, we reported an intriguing case of primary disseminated intra-abdominal hydatidosis.
Case Report
Patient information
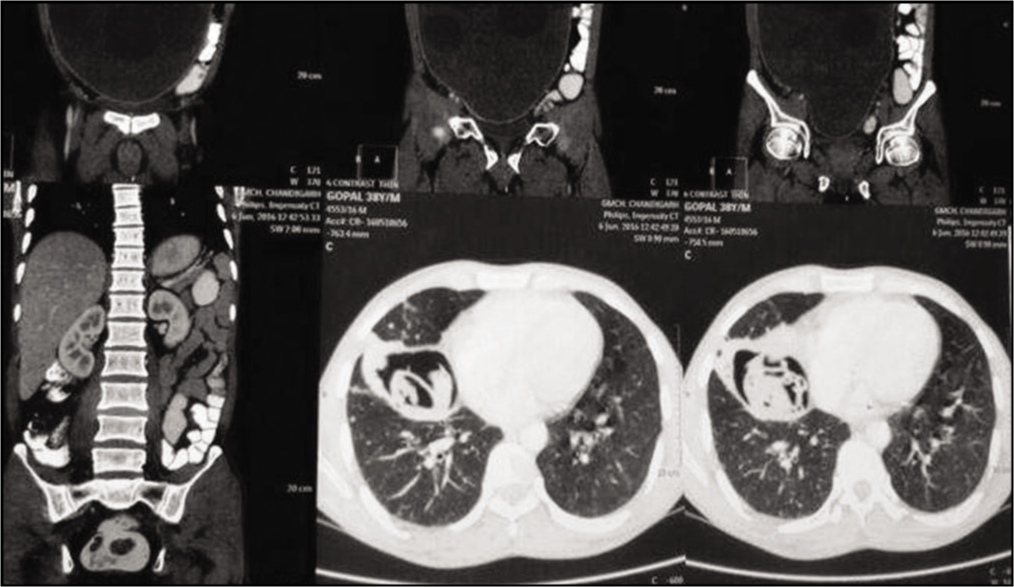
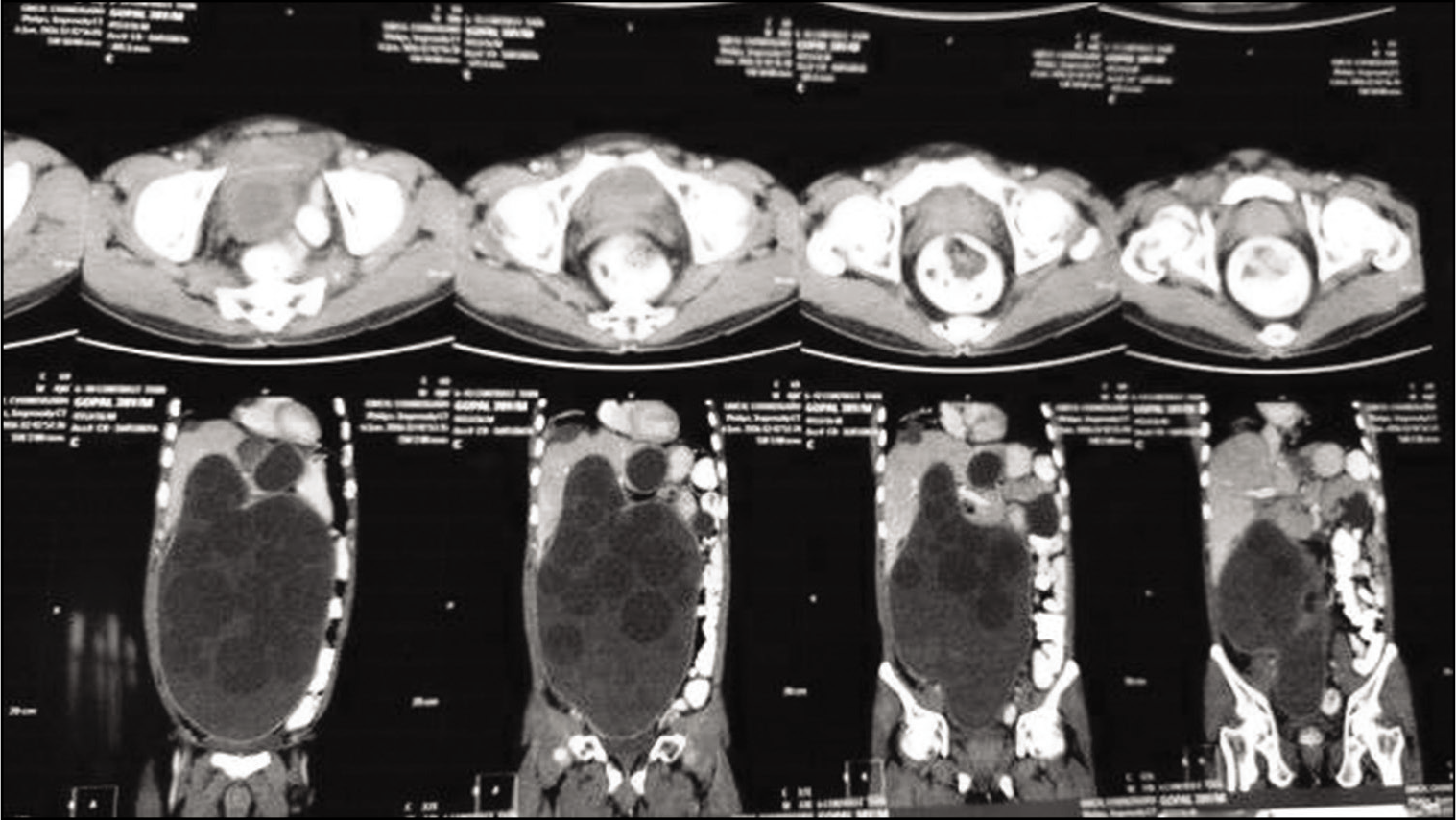
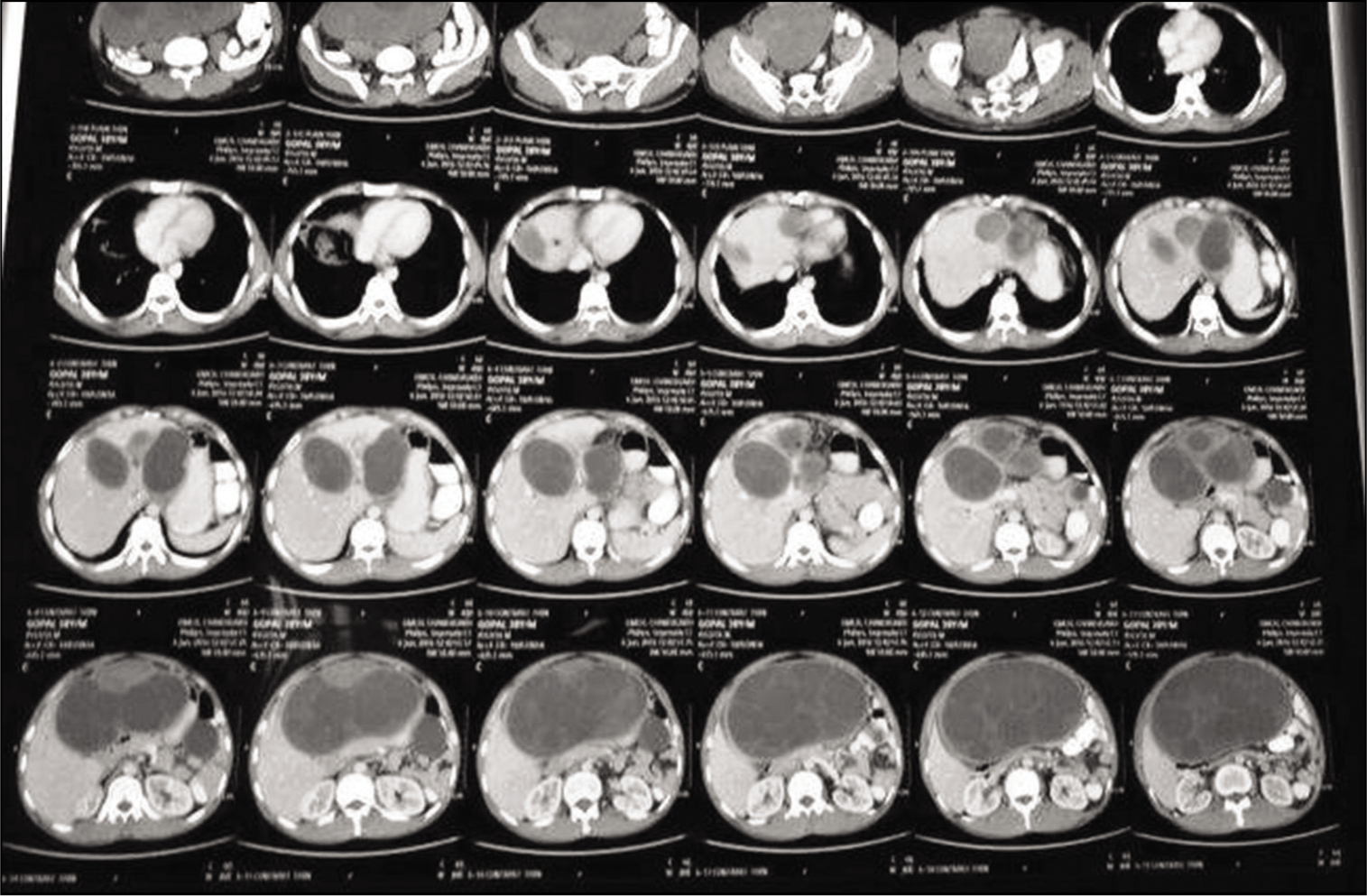
A 38-year-old male patient, a poultry farmer by profession, presented to the hospital with the chief complaints of pain in the abdomen, along with gradual abdominal distension for the past 1 month; fever for the past 20 days; nonprojectile vomiting containing food particles for 20 days; and shortness of breath with nonproductive cough for 7 days. No other cardiovascular, respiratory, gastrointestinal complaints were reported. On examination, the abdomen was distended, tense, and mildly tender. The umbilicus was slightly inverted. The laboratory investigations were as follows: hemoglobin –11.5 g/dl, total leukocyte count –12,000/μL with 10% eosinophils, and urea/creatinine –34/0.9. The liver function tests and serum electrolytes were within the normal range. Ultrasound of the abdomen revealed multiple peritoneal hydatid cysts with hepatomegaly –19 cm and two cystic lesions in the left lobe of liver. Furthermore, contrast-enhanced computed tomography (CECT) of abdomen confirmed peritoneal hydatidosis with hepatic and lung hydatid cysts [Figures 2-4]. The characteristic water-lily sign signified the presence of simple as well as complicated hydatid cysts.
CECT abdomen confirmed peritoneal hydatidosis with hepatic and lung hydatid cysts. CECT: Contrast-enhanced computed tomography
CECT coronal section - abdomen confirmed peritoneal hydatidosis with hepatic and lung hydatid cysts. CECT: Contrast-enhanced computed tomography
CECT axial section - abdomen confirmed peritoneal hydatidosis with multiple hepatic and lung hydatid cysts. CECT: Contrast-enhanced computed tomography
Therapeutic intervention
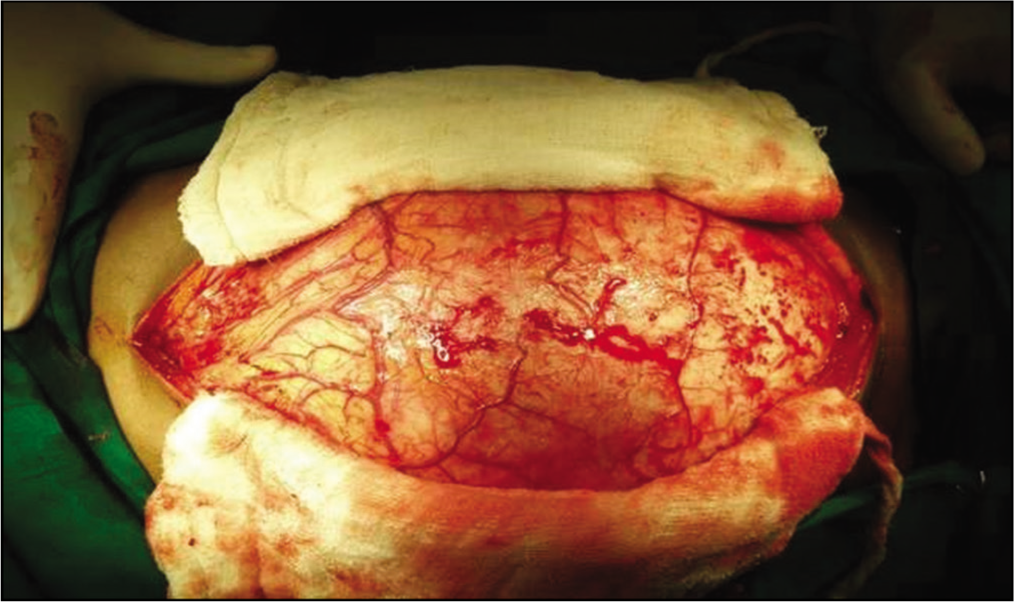
The patient was diagnosed with disseminated hydatid disease and managed conservatively with tablet albendazole 400 mg twice a day. He was advised surgery, following which, Pre-Anaesthesia Clearance (PAC) was done. However, the patient’s attendant denied surgery and took discharge on request. The patient presented, after a month, to the surgery emergency with acute abdomen, for which he underwent surgery. Following general anesthesia, a midline abdominal incision was given. A giant hydatid pericyst was found occupying the whole abdomen, making it difficult to enter the main peritoneal cavity [Figures 5 and 6].
A giant hydatid pericyst was found occupying the whole abdomen, as the midline incision was given
The cyst fluid, membranes, and daughter cysts after incision of the large pericyst
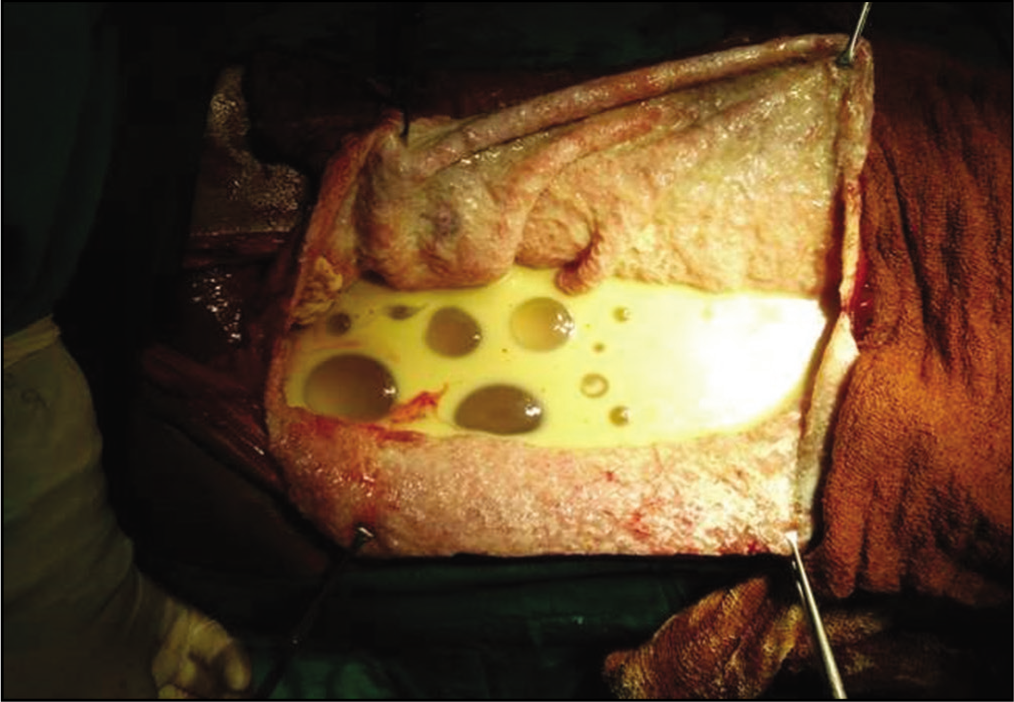
The pericyst was incised, after keeping 10% betadine sponges all around to avoid spillage. All cyst fluid, membranes, and daughter cysts were removed/sucked with suction. The intraoperative findings were as follows: the cyst was pushing the whole gut posteriorly; the cyst was arising from the right lobe of the liver and growing in an exophytic manner in the main peritoneal cavity; and there was another cyst in the left lobe of the liver. After which, the whole pericyst of the right lobe cyst was excised. The left lobe cyst was marsupialized. There were multiple biliary openings at the base of the cyst, arising from the right lobe. After lavage, two drains were put near the right and the left lobe of liver draining bile, following which the abdomen was closed in layers [Figure 7].
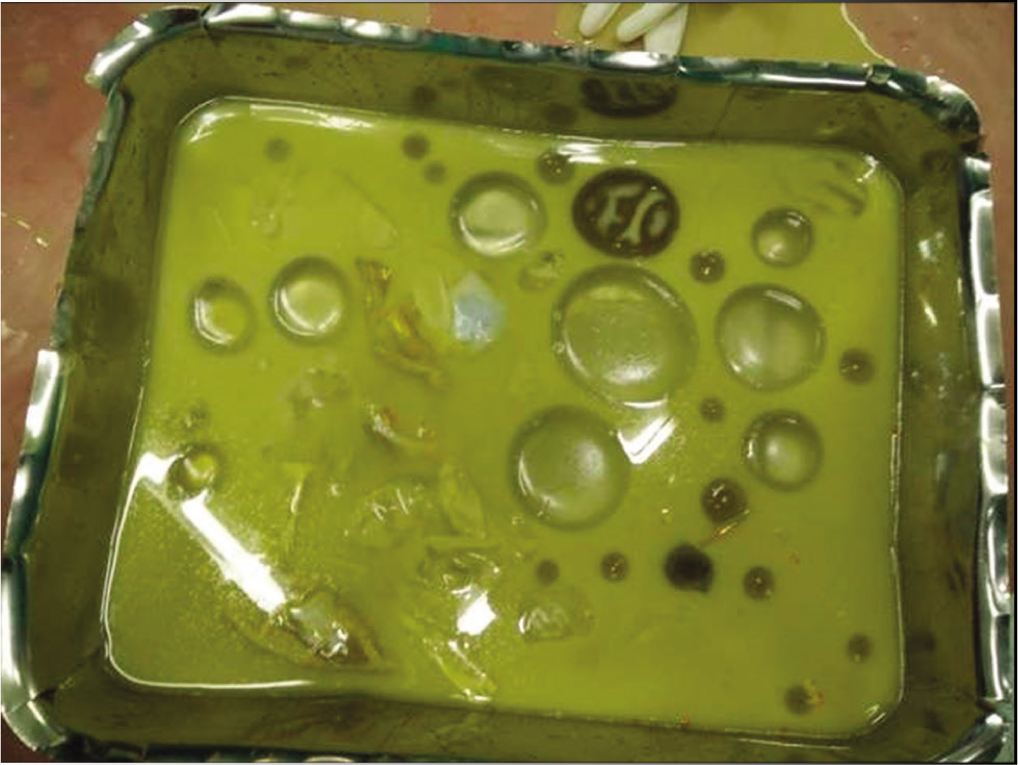
The picture shows the cyst fluid, membranes, and daughter cysts after drainage of fluid in operating tray
Follow-up and outcome
The patient was allowed nutrition perorally from the 4th postoperative day. The postoperative period was uneventful till the 14th day. The drain output noted was around 300 cc bile. The patient was put on oral albendazole. On the 18th postoperative day, the patient experienced one bout of massive hemoptysis, for which he was managed with cold saline gastric lavage, proton pump inhibitors, sucralfate, and whole blood. On the following day, a CECT abdomen was done which revealed a large perforation anteriorly in the antrum of the stomach. The patient was taken up for surgery again. Primary repair of the gastric perforation was done with gastrostomy and feeding jejunostomy, following which, the patient was shifted to the intensive care unit (ICU). In the ICU, the patient died of sepsis on the 6th postoperative day.
Discussion
Peritoneal cavity is a rare location for the cysts to develop. Secondary peritoneal hydatidosis develops as a result of iatrogenic rupture of hepatic, mesenteric, or splenic cysts which is much more common than primary disease.[5] Spontaneous rupture of the cysts accounts for 12% of the cases worldwide. Primary hydatid disease is seen as a presentation in only 2% of the cases of intra-abdominal hydatidosis and occurs as a result of arterial spread of the hexacanth embryos to the peritoneal cavity or direct invasion through the bowel wall into the peritoneum.[6]
The disease shows a spectrum of clinical presentations which depends on the organs involved; size and site of the cysts in the affected organ; pressure effects due to the cysts. The cysts grow up to a definitive size before they produce symptoms, therefore, go unnoticed for initial few years. A mass may be palpable in the right hypochondrium with symptoms of right quadrant abdominal discomfort, nausea, and vomiting. The cyst may rupture, precipitating anaphylactic reaction.[7] Pulmonary cysts produce bronchial compression when >5 cm in diameter. Cyst rupture produces symptoms such as hemoptysis, chest pain, and cough. Suppuration and secondary infection are some of the other complications of pulmonary hydatidosis.[8] The peritoneal hydatid cysts are usually present with vague abdominal pain or allergic reaction in case of rupture.[9]
The serological tests employed in the diagnosis of hydatid disease are the Casoni (intradermal) test; immune hemagglutination test; and indirect fluorescent antibody test. ELISA is the most commonly used test to detect anti-Echinococcus immunoglobulin G antibodies.[10] Rupture of the cysts in the biliary tree can be detected by the presence of increased levels of cholestatic enzymes, hyperamylasemia, and eosinophilia. The final diagnosis rests on a combination of serological and radiological imaging. The radiological tools used for the diagnosis include plain radiography, ultrasound examination, CT scan, and magnetic resonance imaging. CT scan and ultrasonography are preferred in case of abdominal cysts. According to Gharbi’s classification criterion, the ultrasound appearances can be classified as follows: Type I – collection of pure fluid; Type II – collection of fluid with a split wall; Type III – collection of fluid with septa; Type IV – heterogeneous echo patterns; and Type V – reflecting thick walls.[11] The WHO classification is based on the cyst morphology as follows: CE1 – unilocular anechoic lesion with double-line sign; CE2 – multiseptated rosette-like honeycomb cyst; CE3A – cyst with detached membranes (water-lily sign); CE3B – cysts with daughter cysts in solid matrix; CE4 – cyst with heterogeneous hyperechoic/hypoechoic contents, no daughter cysts; and CE5 – solid plus calcified wall.[12]
The mainstay of therapy for disseminated peritoneal hydatid disease is medical; however, the gold-standard management for intraperitoneal rupture of hepatic cysts consists of emergency radical or conservative surgery. The conservative approach includes removal of the cysts along with their contents followed by peritoneal wash using a scolicidal agent, preferably hypertonic saline. Radical surgery includes pericystectomy which carries a higher risk for complications but lesser chances of relapse. Percutaneous aspiration–injection–reaspiration technique is employed in cases with contraindication to surgery or relapses following surgery and chemotherapy. The chemotherapeutic agents used are albendazole (10–15 mg/kg/d) or mebendazole (40–50 mg/kg/d) for a period of 3–6 months.[13]
Conclusion
Hydatid disease presenting as primary peritoneal dissemination is an extremely rare case scenario. A high index of suspicion is required to diagnose such cases. An interdepartmental collaboration is crucial in making a definitive diagnosis and then planning a holistic management scheme at the earliest. This case report describes the presentation and management along with complications and follow-up of a case of primary peritoneal hydatidosis with underlying hepatic cysts. Although, in our case, we attempted both medical and surgical management, still, if the patient did not left in the first admission and early surgical intervention would have been done, then the prognosis might have improved. Therefore, early diagnosis and timely adequate treatment improve the prognosis of disseminated peritoneal hydatid disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that he has obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Patient Consent
Written patient’s wife consent is present, duly signed by the patient. The authors obtained the consent after explaining that no identity will be revealed, and the case information, including pictures, will be used for education purposes only. She was also explained that journal publication will not contain any material or picture disclosing his identity. The patient gave positive consent for publication, and the authors certify that written patient’s wife consent is present, procured for publication.
Informed Consent
Proper written consent is present, which was obtained from the patient’s wife for the use of the data related to this case.
CRediT Author Statement
AG, DK: Case presentation, data collection, investigations, and writing of original draft
MG, AD: Literature review, writing of original draft including conclusion, references, and formatting.
Data Availability
Available in Medical Records Department of hospital.
Use of Artificial Intelligence
Not used during any part of the preparation of the article.