
Abstract
Background:
Bee sting is a common entity during the summer season and is rarely associated with devastating complications such as myocardial infarction, pulmonary edema, bleeding, and rhabdomyolysis, neurological complications can occur after multiple stings. However, single bee venom infestation resulting in such complications is rare.
Patient’s Concern:
Here, we are describing a young male, who presented to us with a seizure episode, soon after bitten by a bee sting around his lips. The patient did not have hypertension, diabetes, other risk factors for seizure, or any history of trauma but the patient’s computed tomography head showed cerebral hematoma.
Intervention:
The patient was managed immediately with an injection of antiepileptics with intravenous (IV) fluids, antihistaminics, and IV steroids. The patient had gross improvement in the sensorium and was seizure free for 48 h under observation. The patient was discharged on the 4th day of admission with 100% recovery.
Conclusion:
This case report emphasizes the potential for severe neurological complications following bee stings in the form of cerebral hematoma which is clinically important to recognize early and further research is required to better understand the mechanism and management strategies.
Introduction
Bee stings are common during summers, following which mild-to-severe allergic reactions can occur, including local pain, swelling, itching, and blistering. Severe systemic reactions, such as myocardial infarction, pulmonary edema, bleeding, and rhabdomyolysis, can occur when multiple stings occur. Massive envenomations, where a single sting releases high venom loads equivalent to >50 stings result in a toxic reaction.[1] These toxins can cause various neurological complications including seizures, ischemic, or hemorrhagic stroke through various mechanisms. Here, we present a case of a young male presenting with seizure and intracranial hemorrhage following 5–6 h of single bee sting at the upper lip.
Case Report
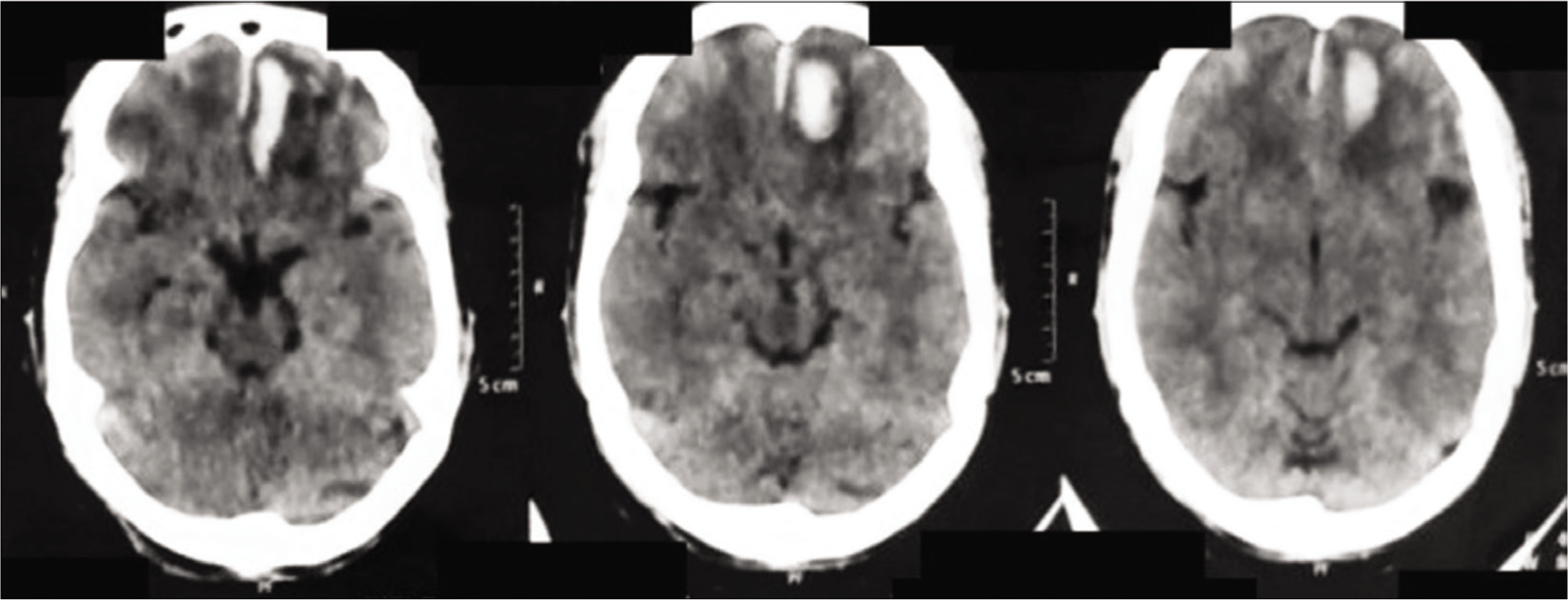
A 35-year-old male presented to the emergency room in an altered sensorium following a seizure episode. The patient had a bee sting on the same morning while he was driving to work. He was stung on his upper lip following which he developed a localized swelling but he continued to work without taking any medications. Four hours later, he started feeling uneasy, dizzy, and sweaty and became unconscious. His colleagues took him to the local hospital where he developed two episodes of generalized tonic–clonic seizures, and got referred to our hospital. At the presentation, he was confused, incoherent, and recognized his relatives but disoriented to place with a Glasgow Coma Scale of 14/15. A swelling of the upper lip was noticeable. There was no headache, vomiting, trauma, fever, or history of atopy. His blood pressure was 110/70 mmHg, heart rate 88 beats/min, respiratory rate 14 breaths/min, and oxygen saturation 98% under room air. Pupils were normally reacting to light with the right plantar extensor and left flexor. Considering primary recurrent seizures, he was started on levetiracetam injection, weight-based loading dose given followed by 12 hourly maintenance dose. Furthermore, parenteral antihistaminics and dexamethasone 4 mg injection were administered at presentation to avoid bee sting-related anaphylactic complications. His electrolytes, hemogram, renal and liver function tests, and coagulation profile returned normal. Noncontrast computed tomography head was done suggesting intracranial hemorrhage in the left frontal lobe [Figure 1], with no other lesion and an intact bony frame.
Computed tomography head showing intraparenchymal bleed in the left frontal region
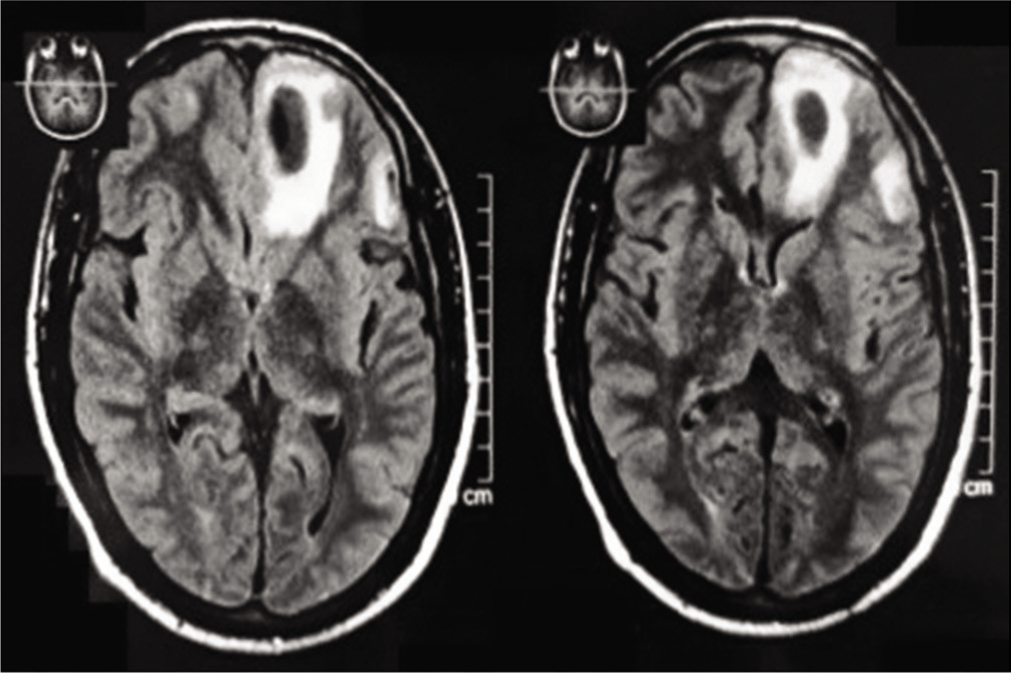
To confirm further the nature of the bleed, contrast-enhanced magnetic resonance (MR) imaging brain with MR angiography was done which revealed a well-defined round heterogeneously hyperintense lesion measuring 24 mm × 12.6 mm on T1 [Figure 2] and hypointense lesion on T2/fluid-attenuated inversion recovery with perilesional edema involving left basifrontal region. Similar small lesions seen in the left cerebellar parenchyma and inferior gyrus of the left frontal region suggest intracranial hematoma with vascular structure showing no aneurysmal changes. Neurosurgical opinion was obtained and any operative management was ruled out. He was managed conservatively and remained seizure free for 48 h under observation. On discharge, he was in a hemodynamically stable condition and planned to follow-up regularly.
T2 image of magnetic resonance imaging brain showing hypointense lesion surrounding perilesional edema in basifrontal region
Discussion
Neurological complications following bee stings are very rare and usually related to delayed immune response. Most patients only develop anaphylactic reactions but patients sensitive to immunoglobulin E (IgE) can develop severe complications. Mechanisms of occurrence of these complications are poorly understood in the literature. It has been found that typical antiepileptics including gamma-aminobutyric acid receptor blockers and calcium channel blockers are ineffective in controlling these seizures when mice are experimentally injected with a component of bee venom phospholipase A2.[2] These substances adhere to specific neuronal sites and result in seizures in mice.
Bee stings increase cytokines such as interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor, which trigger adverse reactions such as urticaria, angioedema, bronchospasm, myocardial depression, hypotension, and shock.[3] The venom of honeybees/wasps contains histamine, mast degranulating peptide, melittin, phospholipase A2, hyaluronidase, and acid phosphatase. Melittin is the most antigenic which results in IgE-mediated severe immune reaction. Melittin interferes with complement cleavage and bradykinin release, causing hemorrhage. Membrane-bound monomers of melittin, transient openings occur through which internal bleeding occurs.[4] Both mechanisms are directly or indirectly associated with coagulation, thrombolysis, hemolysis, and smooth muscle tone. Furthermore, bee venom contains apamin, phospholipase A2, mast cell degranulation peptide, hyaluronidase, histamine, dopamine, and hemolysin, which have toxic and hemolytic effects.[5] It is phospholipase A2, which, in conjunction with melittin, produces profuse hemolytic effects, resulting in hemorrhagic stroke.[6]
The clinical outcome following the stroke depends on the nature of the lesion, such as the location and size of the infarct/hemorrhage, hematoma expansion, edema formation, and intraventricular hemorrhage.[7] Our patient had a good outcome as the lesion was small and prompt early treatment was given. The mainstay of management in bee stings with neurological complications remains conservative including corticosteroids, antihistaminics, and antiepileptics. Specific evidence-based guidelines do not exist as most cases pertain to anecdotal reports.
On reviewing the medical literature, a similar case is reported in which a patient presented with nontraumatic cerebellar, subarachnoid, and parenchymal hemorrhage 2 days after being stung by 8–10 bees.[8] Another case was reported from Delhi with both ischemic and hemorrhagic stroke following 3–4 h of single bee stung.[9] However, our case exhibited unusual symptoms within 5–6 h of a single bee sting on the face. We emphasize the importance of being watchful for complications, especially when the bee sting is in the facial region.
Conclusion
This case report emphasizes the potential for severe neurological complications following bee stings. Health-care professionals need to be aware of these rare but serious reactions and consider them in the differential diagnosis when encountering patients with unexplained seizures or intracranial hemorrhage. Further research is needed to better understand the underlying mechanisms and to develop appropriate management strategies for such cases as the database is very limited.
Footnotes
Acknowledgements
I would like to thank the patient and his family for their support and cooperation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understands that his name and initials will not be published and due efforts will be made to conceal his identity, but anonymity cannot be guaranteed.
CRediT Author Statement
The authors Monica Gupta and Amandeep Kaur contributed to the study conception and design. Material preparation, data acquisition, literature search, data collection, and analysis were performed by all 4 authors. The first draft of the manuscript was written by Amandeep Kaur, Monica Gupta, and all authors commented on all versions of the manuscript. Monica Gupta and Ishreen Ahuja critically revised the work. All authors read and approved the final manuscript.
Data Availability
Data is available upon reasonable request from the corresponding author.
Use of Artificial Intelligence
Artificial intelligence was not used for this study.