
Abstract
Introduction
Globally, perinatal death presents a profound challenge for healthcare and healthcare professionals, requiring enormous clinical expertise and mental fortitude. The complexity involved in balancing professionalism, empathy, and the human face pose significant emotional challenges for nurses and midwives. Perinatal deaths in Ghana remain high and have adversely impacted the achievement of Sustainable Development Goal 3. Nurses and midwives play a central role in the Ghanaian healthcare system, and understanding their experiences in providing care to grieving mothers can provide valuable data for enhancing bereavement support as well as promoting quality improvement in clinical care.
Objective
To explore the experiences of nurses and midwives who support bereaved parents during perinatal deaths in Ghana.
Methodology
A descriptive-phenomenological approach was used to explore the lived experiences of the participants. Twelve participants were purposively recruited from the neonatal and intensive care unit of a District Hospital in northern Ghana. Interviews were conducted using a semi-structured interview guide. The data was analyzed iteratively using the thematic analysis approach.
Findings
Six themes emerged from the interviews with the study participants. The six themes were personal experience of perinatal death, emotional impact on the nurses and midwives, parental reactions and coping, blame and guilt, the impact on work, and long-lasting psychological impact. The themes reflect the emotional and practical experiences encountered by the nurses and midwives when supporting bereaved parents and the impact of such experiences on their well-being.
Conclusion
Perinatal bereavement support is a core responsibility of the nurses and midwives who work in maternal and neonatal units. Despite an improvement in perinatal death globally, the rates are still of great concern in Sub-Saharan Africa. Ironically, the experiences of nurses and midwives who support parents in times of perinatal death are lacking in Sub-Saharan Africa. This study sheds light on the experiences of nurses and midwives who support parents during perinatal death in a Ghanaian context, highlighting the importance of supporting these healthcare professionals.
Keywords
Introduction
Perinatal death refers to fetal death of at least 28 weeks of gestation and/or 1000 g in weight and newborn death of up to and including the first seven days after birth. 1 Thus, perinatal death includes miscarriage, stillbirth, and neonatal deaths. 2
Although the global rate of perinatal death is declining, the burden is still unacceptably high, with stillbirth occurring every 16 seconds, amounting to 5,400 each day and 2 million every year, which means approximately 1 in 72 babies are affected.3, 4 Over the past two decades, a staggering 48 million stillbirths have been documented globally. 3 More worrying is the fact that Sub-Saharan Africa alone accounts for 42% of global stillborn babies. 3 In 2021, the global estimate for neonatal mortality stood at 17.5 (16.5–19.5) per 1,000 live births, whereas in Sub-Saharan Africa, the estimate was higher at 27 (24.4–32.2). 5
Specifically, in Ghana, the stillbirth rate was reported as 21.7 (16.4–28.3) per 1,000 total births in 2019, while the neonatal mortality rate was 22.8 (16.9–30.8) per 1,000 live births in 2020.3, 5, 6 Locally, the Bongo District Hospital Annual Performance Review 7 reported a perinatal mortality rate of 29.2 (2020), 35.0 (2021), and 25.6 (2022) per 1,000 live births. Perinatal deaths are therefore not evenly distributed, not even in-country.
According to Verdon et al., 8 nurses and midwives who support parents during perinatal deaths experience distress and grief over the death. Previous studies have also reported a feeling of deep sadness, grief, guilt, and helplessness among nurses and midwives as they witness the profound sorrow of grieving parents.9, 10 Nurses and midwives who support parents during perinatal death often experience a wide range of emotions, which can affect their ability to provide compassionate care. However, compassionate support from healthcare professionals, particularly nurses and midwives, is crucial during perinatal grieving. Consequently, nurses and midwives may be at risk of compassion fatigue and burnout due to the emotional demands of this role.
Available literature indicates that the emotional impact on care providers can be so profound that they may struggle to find the right words for the fear of saying something inappropriate 11 when supporting the bereaved parents and their families. Additionally, nurses and midwives may find it challenging to balance the emotional needs of parents with the demands of medical procedures, 9 making the period of perinatal loss a critical moment for the healthcare worker and the bereaved parents. According to Papadatou, 12 healthcare providers invest a lot in the care and support of their patients and families. This investment becomes the source of their grief; therefore, healthcare professionals will experience their loss differently for every perinatal death. Papadatou 12 identified these losses and categorized them as loss of a close relationship with a particular patient with whom one has shared part of a significant journey, loss due to a professional’s identification with the pain of family members, loss of one’s unmet goals and expectations and one’s professional self-image and role, losses related to one’s personal system of beliefs and assumptions about life, past unresolved losses or anticipated future losses, and the death of self. 12 There is an abundance of literature mostly studied in the West and in the cultural context of the West,8, 10, 13–18 reporting on the emotional, physical, and psychological impact on nurses and midwives who support bereaved parents and families during perinatal death. The studies have also indicated that the emotional and psychological challenges that nurses and midwives who support bereaved parents go through during perinatal death greatly impact their productivity.8, 14 Ironically, these studies, which mostly informed our current understanding of the experiences of nurses and midwives who support bereaved parents, were mostly conducted in high-income countries, mostly in the West, where enormous progress has already been made in perinatal bereavement care.
A search of the literature reveals a scant amount of evidence that specifically studies the experiences of nurses and midwives who support bereaved parents during perinatal loss in Africa. A few of the studies investigated the experiences of health workers in general, including nurses, midwives, and doctors, in Kenya and Uganda. 19 Healthcare professionals in this study also reported sadness, frustration, guilt, and shame, a situation that is worsened by a lack of preparation and support from senior management. 19 In Ghana, while there have been a handful of reports of healthcare professionals’ experiences of perinatal death,20, 21 these were not studies that specifically targeted nurses and midwives who provide frontline perinatal bereavement support. Due to the differences in healthcare policies, cultural differences, health education and training, and the disproportionate burden of perinatal death between lower-middle income countries and high-income countries, the findings and for that matter interventions that are based on Western knowledge of the experiences of nurses and midwives during perinatal death may not be truly representative of lower-middle income countries.
This study aims to explore the experiences of nurses and midwives who support parents during perinatal death in Ghana. The findings from this study will enhance the development of support systems for healthcare workers who support families during bereavement.
Research Question
What are the experiences of nurses and midwives who support bereaved parents during perinatal deaths?
Methodology
Research Setting
The study was conducted in a district hospital in the Upper East Region of Ghana. The district has a total of 67 health facilities and health posts. However, the study site is the only facility with hospital status in the district, serving as the main referral center for the remaining 66 facilities. 7 Specifically, the participants were drawn from the newborn unit, which is made up of the maternity and neonatal units of the hospital. Both units have a combined staff strength of 59 nurses and midwives. The total bed capacity of both units is 56, consisting of 46 at the maternity unit and 10 at the neonatal unit. On average, the maternity unit delivers 1,185 babies yearly, of which approximately 24 will be stillborn. The neonatal intensive care unit (NICU) admissions and the number of neonatal mortalities from 2020 to 2022 are averaged at 448 and eleven (11) annually, respectively. 7
Research Design
This study employed a descriptive phenomenological approach to explore the lived experiences of nurses and midwives caring for parents during perinatal deaths. Phenomenology allows a detailed and in-depth exploration of individuals’ subjective experiences, capturing the meaning and essence of these experiences as they occur to the study participants. 22
Study Population
All registered nurses and midwives working at the newborn care unit of the District Hospital and who met the inclusion criteria were interviewed.
Inclusion and Exclusion Criteria
Inclusion Criteria
Being a registered nurse or midwife working at the Newborn Care Unit of the District Hospital, having experienced at least one perinatal death, and consenting to data collection were included in the study.
Exclusion Criteria
Registered nurse or midwife not working at the newborn care unit, working in the unit but on any form of leave, not having experienced perinatal death, or not consenting to the data collection were excluded from the study.
Sample Size
A sample size of 20 was initially planned;23, 24 however, having applied the principle of data saturation, a total of 12 participants were interviewed. Six each of nurses and midwives participated. Data saturation refers to the point in data collection where new information or insights stop emerging and the researcher feels that they have achieved a comprehensive understanding of the phenomenon under study. 25 The final sample size was determined iteratively as data collection and analysis progressed. Sampling continued until a point of saturation was reached, where additional interviews did not provide substantially new or different information.
Sampling Method
The study employed a purposive sampling technique. This approach was necessary to recruit only nurses and midwives who had firsthand experience of supporting parents during perinatal deaths at the Bongo District Hospital and as such, had valuable insights and experiences relevant to the study objective. 26
Data Collection Procedure
A semi-structured interview was employed for data collection, and all interviews were conducted at the study site at the convenience of the study participants. All interviews were conducted by the first author.
A semi-structured interview was used due to its suitability to the study objectives and because little is known about the phenomenon under study; therefore, there were no predetermined questions to pose.27, 28 To ensure an in-depth and rich engagement with the participants, the researchers developed an interview guide comprising themes27, 29 that sought to elicit participants’ experiences of perinatal death. All interviews were audio recorded using a digital audio recorder and transcribed verbatim.
Data Analysis
The digital audio-recorded interviews were first transcribed verbatim using inbuilt transcription features of Microsoft 365. 30 The transcriptions were then analyzed using Braun & Clarke’s 31 six-step thematic data analysis of qualitative data. The first step was the familiarization of the data through repeated readings of transcripts. The second step involved the generation of initial codes. Third, themes were developed from the codes generated. The fourth step was a revision of the themes generated from step 3. In step five, the themes were defined. The final step was writing the emerging themes alongside outstanding participants’ quotes. Steps 1–4 were independently undertaken by the first and second authors. The codes from the independent analysis were then reconciled prior to step 5. The differences were resolved by the last author.
Methodological Rigor
To ensure the trustworthiness of this study, the researchers employed Lincoln and Guba’s Framework of Qualitative Criteria as elaborated by Polit and Beck, 32 for developing the trustworthiness of a qualitative inquiry: credibility, dependability, confirmability, and transferability.
Credibility
To achieve this, reflexivity was observed during data collection by being conscious of the first author’s own biases, experiences, interests, beliefs, and professional background to influence the responses of participants. Deep probing was employed, and participants were allowed to freely talk about their experiences until they had nothing more to say. Assuring participants of their confidentiality and the anonymity of their identities gave them the confidence to freely talk about their experiences without any reservations. All the participants met the inclusion criteria, and the exclusion criteria was strictly adhered to.
Dependability
The same interview guide was used for all the research participants. The guide was pretested among three trial participants in a different district of the same region to ensure that it was able to effectively elicit responses that could satisfy the study question. Although probing questions were rephrased during the interviews, their original meanings were maintained.
Confirmability
To ensure the confirmability of the study findings, audio transcription was completed verbatim using the inbuilt features of Microsoft Word, the themes were initially developed independently by the first and second authors, and where misunderstanding occurred and could not be resolved, the last author helped to resolve them. An audit trail of audiotaped data, transcripts, consent forms, and the semi-structured interview guide were kept for external or future scrutiny.
Transferability
In ensuring this, a detailed and complete description of the research setting and context has been made. Additionally, the study’s design, data collection tool and procedure, and number of participants were reported. The researchers also used a purposive sampling technique to select the participants who possessed the characteristics necessary to provide useful information for the study.
Ethical Consideration
The ethical clearance for this study was obtained from the Institutional Review Board of the 37 Military Hospital, Ghana. A written permission was also granted by the Bongo District Hospital before the commencement of the study. Verbal and written informed consent were obtained from all prospective participants prior to conducting the interviews or engaging in study activities, ensuring their voluntary participation and understanding of the study’s purpose, procedures, potential risks, and benefits. The study posed no harm to any participants, and they were free to withdraw from the study at any time without facing any penalties. All audio recordings and transcribed data were stored on a separate storage drive, password-protected, and secured from unauthorized access. Only the investigators have access to the data.
Results
Demographic Characteristics and Work Experience of Participants
Twelve nurses and midwives working at the maternity and neonatal units of Bongo District Hospital participated in the interview. They were 10 females and 2 males between the ages of 28 and 48 years. Seven of the participants were Christians, and 5 were members of the Islamic faith. Participants had at least one year and at most 17 years of working experience with parents and neonates. The longest-serving participants reported a total of 100 perinatal death experiences during their respective 17 and 16 years of working with parents and neonates. The minimum experience of perinatal death was two during a participant’s one-year work experience with neonates. Table 1 illustrates the demographic characteristics and work experiences of the study participants. Six themes emerged from the experiences shared by the nurses and midwives: personal experience of perinatal death; emotional impact on the nurses and midwives; parental reactions; coping, blame, and guilt; the impact on work; and long-lasting psychological impact.
Demographic Characteristics and Work Experience of the Study Participants.
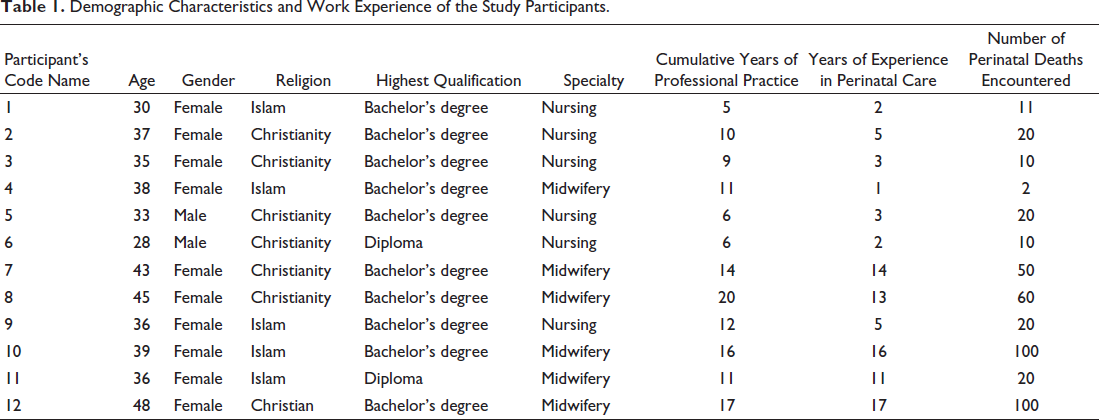
The themes reflect the emotional and practical experiences encountered by the nurses and midwives when supporting bereaved parents and the impact of such experiences on their well-being. An elaborate presentation of the themes has been given below with supporting participants’ quotes.
Balancing Personal Loss with Compassionate Care
The participants mentioned their personal experiences of losing a child or witnessing the perinatal deaths of a close relative or friend, which led them to empathizing with bereaved parents and using their own experiences to provide support and counseling. They recounted personal experiences of not receiving the support they needed when they had to face the death of a loved one. By reliving those experiences, they were able to support bereaved parents. Others felt being females helped them to understand the losses experienced by bereaved mothers.
I actually lost my first child about 10 years ago and so I have lived it and I always show bereaved mothers’ empathy. I have always used myself as an example to several bereaved parents and share some of the coping mechanisms I used in order to get over it. (Participant 10; midwife) I always feel very sad seeing my fellow women go through such pain. (Participant 2; nurse)
Emotional Impact on the Participants
Participants expressed feelings of sadness, guilt, demoralization, stress, and burden when dealing with perinatal deaths.
Very sad, you feel demoralized. Sometimes you even feel bad to the extent that you can’t even talk to the mother. (Participant 1; nurse)
They mentioned that the emotional toll can affect their mood, work output, and overall well-being.
If a baby passes away, it is as if a part of you the nurse has been taken away and lose interest in the work. It affects some nurses so much that they will want to take some form of leave to get over it. (Participant 3; nurse) I become very sad and the whole day I can’t do anything. (Participant 8; midwife)
Some participants also shared instances of developing a connection or bond with the parents and babies, which made the loss more difficult to cope with.
Some of these perinatal deaths affect me seriously because I sometimes develop a form of connection or bond with parent and the baby. (Participant 12; midwife)
Adjusting to Parental Reactions and Coping
Participants observed that parents react differently to perinatal loss. Some parents cope well, possibly due to cultural beliefs or prior expectations, while others experience intense grief, crying, and wailing. Some participants stated that there were times they wished they were not left all alone to break bad news to parents due to the uncertainty with which the parents may react to the news. There is a fear that they can be hurt by parents who do not take their bad news well.
Some parents believe that you don’t buy clothes for a baby you have not delivered yet, even sometimes educated ones. Such parents do not grieve for long when baby dies. And to others, they have struggled for years in order to conceive and then lose a baby. So, the grieving process is different for each bereaved family. (Participant 4; midwife) I think breaking bad news should not be left on the nurses or midwives alone. Because sometimes we are afraid about the outcome after breaking the news. (Participant 9; nurse)
Impact on Work
Participants mentioned that perinatal deaths have always affected their work, reducing their ability to provide care for other babies and increasing their stress levels.
After losing one baby on the ward, the care you give to other babies reduce because you are down. And you feel the care you have given is not enough. You feel all your efforts prove futile. You don’t feel motivated to work so it really affects the shift. (Participant 1; nurse). I just pretend that we are fine for the sake of the other surviving ones. So, we are able to manage to pull ourselves together somehow in order to care for the surviving babies. Sometimes too, I go to sit down, say a prayer, and then I get up again just to attend to other cases. (Participant 9; nurse)
Long-lasting Psychological Impact
Participants recounted that perinatal bereavement had a long-lasting impact on healthcare providers, including psychological distress and worry about the well-being of the parents. Some participants still remember parents they have supported previously and have always wondered if they have been supported enough to move on.
Personally, I am affected psychologically. I think about them a lot and I worry and if I worry, my colleagues too worry because death doesn’t happen on one shift. (Participant 7; midwife) Oh psychologically, as I am speaking to you there is this client of mine. I always think about her whether she has moved on. (Participant 9; nurse) I really feel for them. I had a personal experience where the death of a baby I nursed overnight affected me so much that, I became depressed, dehydrated, and it took the support of my husband to be able to recover from that incident. (Participant 8; midwife)
Blame and Guilt
The nurses and midwives stated that they often experience guilt and blame, which extends its reach into professional relationships, thereby straining the bond between them and the families they support. The fear of being blamed for the loss of a baby was frequently mentioned as a factor that cast a shadow over the communication dynamics, making it difficult for them to effectively convey empathy and support to grieving parents. The intricate balance of professionalism and empathy becomes a delicate dance, with the weight of guilt and blame influencing the nature of these crucial interactions.
I normally feel guilty, more stressed and in some instances feel burdened to manage bereaved parents because, there is limited support in terms of resources, staffing, flexible scheduling as well as supportive environment. (Participant 12; midwife) Some too are always being aggressive, they (bereaved parents) blame us that we have killed the baby. You hear some of them on radio saying we have killed their (bereaved parents) baby because we are not able to exhaust and allow them to go through the grieving process well because they took anger home. (Participant 7; midwife)
Discussion
Perinatal bereavement support is a growing area in healthcare, with increasing recognition of the psychosocial impact of perinatal loss on caregivers.14, 21, 33 With nurses and midwives at the forefront of supporting bereaved parents, studies exploring the impact of perinatal loss on nurses and midwives who care for the bereaved parents are now gaining momentum in Western countries. 8
However, the same cannot be said of Sub-Saharan Africa, where the burden of perinatal death is the highest. 3 This is the first study in Ghana to report the experiences of nurses and midwives who support bereaved parents in a maternity and neonatal unit combined. The nurses and midwives in this study described their rich experiences with perinatal death and bereavement support. Our findings confirm reports8, 34 that nurses and midwives who support parents during perinatal loss experience feelings of sadness, guilt, demoralization, stress, and burden when dealing with perinatal deaths. The nature of the relationship between nurses and midwives and their service users, particularly mothers and expectant mothers, is one in which feelings turn to influence each other. 8 Nurses and midwives who work at the maternity unit and/or neonatal units are often driven by a deep commitment to deliver live babies to their parents. However, when faced with the tragic outcome of a newborn’s death, they may find themselves caught in the throes of guilt, haunted by the belief that they could have done more or taken a different course of action to avoid the loss. This internal struggle arises from a profound desire to fulfill their professional duty to protect and nurture life. As described by Papadatou, 12 participants in this study reported that they developed intense feelings of guilt when they observed parents’ grief and blamed themselves for inadequate effort in preventing the loss. The emotional impact is intense when they have developed some form of bonding with the parents and the newborn.
Our findings also confirm several studies, including those conducted in other parts of Africa, that nurses and midwives can become guilt ridden following perinatal death, with most questioning their competence and doubting their abilities to offer professional support to the bereaved parents8, 10, 13, 14, 16, 19, 34, 35.
Personal experience of the loss of a child, family member, friend, or grief experienced by people in the immediate circle of care givers replays itself in the time of perinatal death. 12 Our findings support Papadatou’s proposed model 12 in this regard and further confirm Jonas-Simpson et al.’s 14 findings that healthcare workers who support bereaved parents relived their past experiences of death and the loss of a loved one. Further, their past experiences also equipped them to better support bereaved parents. While Jonas-Simpson et al. 14 reported that the nurses used their past experiences of loss to better approach bereaved families, we also found that nurses who have healed from their loss used their experiences to teach parents how to cope with their loss.
Although we have not established from this study the role of unresolved losses or grieving by healthcare workers, it is important to be aware of this and support nurses and midwives who support bereaved parents. Another interesting finding from this study was that nurses and midwives’ experiences and how they cope with the loss are partly influenced by the grieving mechanisms of the bereaved families.
A similar finding was made by Rent et al. 21 in a study among healthcare workers in Ghana and Ethiopia, in which participants indicated that when bereaved parents grieve by blaming workers for their loss, coping becomes difficult. Fear becomes a prominent aspect of provider guilt as healthcare professionals express trepidation about being blamed by grieving parents for the loss of their baby. This fear intensifies the emotional burden already borne by the nurses and midwives, creating a cyclical dynamic where guilt and fear exacerbate each other. The emotional strain can hinder effective communication, making it challenging for healthcare professionals to navigate the delicate conversations with grieving parents. 11
These findings suggest the interdependence of healthcare professionals and bereaved parents for a healthy grieving process. We extrapolated from this study and that of Jonas-Simpson et al. 14 that compassionate bereavement support offered by nurses and midwives during perinatal loss can facilitate a better coping mechanism. The emotional burden on caregivers can be very intense, thereby warranting the removal of self from the clinical area. This was evident from the findings of this study, in which nurses and midwives struggled to manage their emotions without having to remove themselves from the presence of the bereaved parents. Others reported demotivation to continue working; consequently, they were compelled to seek a break to process their feelings.
The participants described a feeling of loss and emptiness that could “not be described in words.” This collaborates with other studies that examined the experiences of nurses who support parents during perinatal bereavement.8, 14, 34 Nurses and midwives also suffer from perinatal death, and their grieving process can affect their professional relationship with the bereaved parents and, consequently, the quality of the support they provide them. 11
The emotional toll on the participants extends beyond the professional realm, infiltrating the mental and psychological health of the healthcare professionals. Feelings of sadness, anxiety, and even depression can become palpable as they grapple with the weight of the emotional toll of losing a newborn under their care. Instances have been expressed in this study in which a midwife experienced depressive episodes and dehydration, underscoring the severity of the impact on their mental well-being. A similar finding has been reported by Jonas-Simpson et al. 14 Despite the knowledge of the psychological impact of perinatal death on caregivers dating back to the 1990s, 36 the interventions that aim to address these are not proportionate to the effect. Experiencing perinatal death has a profound impact on nurses and midwives, necessitating the development of interventions and programs to support their coping mechanisms and well-being in the face of this challenging situation.
Conclusion
Perinatal bereavement support is an emerging field in healthcare that focuses on providing support to parents who have experienced the loss of a baby. Nurses and midwives are at the forefront when it comes to supporting bereaved parents. Although nurses and midwives who work at the maternity and neonatal units continue to face significant emotional and psychological challenges relating to perinatal death, their own experiences and the impact of perinatal death on their well-being are often overlooked. This study explored and reported the experiences of Ghanaian nurses and midwives caring for bereaved parents. It is important for policymakers and healthcare managers to be aware that the experiences of these nurses and midwives also influence how they support bereaved parents.
Strengths and Limitations
The main strength of this study is the use of a descriptive phenomenological approach that facilitated in-depth interviews, allowing the participants to share their rich experiences without interruption. The same researcher conducted all the interviews, thereby maintaining consistency across all participants. Also, all the participants had good experience working with parents and families in times of perinatal loss. Participants had experienced a minimum of two perinatal deaths occurring in the study setting, thereby providing us with rich and felt experiences of perinatal death.
Although this study resonates with similar studies from the literature, the generalization of the study could be problematic because of the cultural diversity of the administrative regions and districts of Ghana. Although the use of purposive sampling techniques provided valuable and rich experiences for participants, it is also possible that the participants only shared experiences that they wished to convey to the researcher to please them.
Implications for Practice
The findings of this study provide a clear picture of the experiences and impacts of perinatal death on nurses and midwives in resource-constrained maternal and neonatal units.
The emotional and psychological impact of perinatal loss on healthcare workers is enormous. Therefore, there is a need to establish structured support programs within maternal and neonatal units to support healthcare workers who care for parents and families during perinatal death. These programs should include access to counseling services, debriefing sessions, and peer support groups. The support systems should foster an environment where healthcare workers can share experiences, develop an awareness of the impact of perineal loss on themselves, and seek guidance when necessary to address the emotional toll of perinatal bereavement support.
Finally, this study provides a foundation for further research with a larger sample size to include nurses and midwives in various health facilities and regions to explore the broader and more representative experiences of the nurses and midwives in Ghana. Further study is also underway to understand the coping strategies of the nursing and midwifery staff in the facility.
Footnotes
Acknowledgments
We acknowledge Mr Edward Anyinasong, University Hospital, Dorset, for reviewing the manuscript.
Authors’ Contributions
L.M.: Conceptualization, investigation, methodology, project administration, resources, validation, formal analysis, writing—original draft, writing—review & editing.
G.D.: Methodology and project validation, data curation, writing—original draft, writing—review & editing.
S.K.A.: Conceptualization, methodology and project validation, project administration, data curation, formal analysis, writing—original draft, writing—review & editing, supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The ethical clearance for this study was obtained from the Institutional Review Board of the 37 Military Hospital, Ghana with reference number 37MH-1RB/MP/IPN/753/2023. A written permission was also granted by the Bongo District Hospital before the commencement of the study. Verbal and written informed consent were obtained from all prospective participants prior to conducting the interviews or engaging in study activities, ensuring their voluntary participation, and understanding of the study’s purpose, procedures, potential risks, and benefits. The study posed no harm to any participants, and they were free to withdraw from the study at any time without facing any penalties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.