
Abstract
The world has recently been hit by a pandemic caused by the novel Coronavirus infection. The infection is highly contagious and possesses a significant risk for health care workers caring for the infected patients. With more than 200 countries being affected and around 3,00,000 deaths across the globe, the essential supply of masks and personal protective equipment has been falling short of the ever increasing need. In such crisis there is a need for innovating and designing endogenous masks and equipment to avoid compromise in care of the effected patients and for safeguarding the health of health care workers.
Introduction
Recently, the world has been fighting the pandemic caused by the novel Coronavirus also known as COVID-19, which was first identified as the cause of a cluster of pneumonia cases in Wuhan city of China. It spread rapidly throughout the world. More than 6 million confirmed cases of COVID-19 have been reported across the world. 1 Person-to-person spread occurs mainly through respiratory droplets during coughing, sneezing, or talking. Spread of infection has also been reported through infected surface/fomites by gaining entry through eyes, nose, or mouth. Droplets can travel up to 6 feet. 2 The incubation period varies from 5 to 14 days.3-5 In the absence of specific and effective treatment, prevention seems the best option to keep away the COVID-19. Health care workers treating COVID-19 patients are at highest risk of infection. During the severe acute respiratory disease (SARS) pandemic in 2003, health care workers made up 21% (1706/8096) of the global cases. 6 According to a case series of 138 hospitalized patients from China, 29% (40/138) of the patients were health care workers that had been infected in hospitals. 7 The current recommendations to protect health care workers against COVID-19 are conflicting for nonaerosol-generating routine care of patients.8-11 For example, European Centre for Disease and Prevention (ECDC) and the US Centers for Disease Control and Prevention (CDC) recommend the N95 mask/respirator, while the Public Health Agency of Canada and the World Health Organization (WHO) recommend medical masks.10, 11 Because of huge burden of disease there has been a shortages of surgical masks, N95 masks, and personal protective equipment throughout the globe. 12 This is especially concerning for the medical staff engaged in managing the COVID-infected patients. 1
In view of increasing cases across the globe including India there is shortage of masks and personal protective equipment. Therefore, we aimed to make low cost indigenous masks of different types that could serve the purpose during management of nonaerosol-generating patient care activities.
Material and Methods
The different masks were developed with the help of common things available in most of the homes and neonatal intensive care units (NICUs).
Giri Aakash Respiratory Eye Infection Preventer: GAAREIP
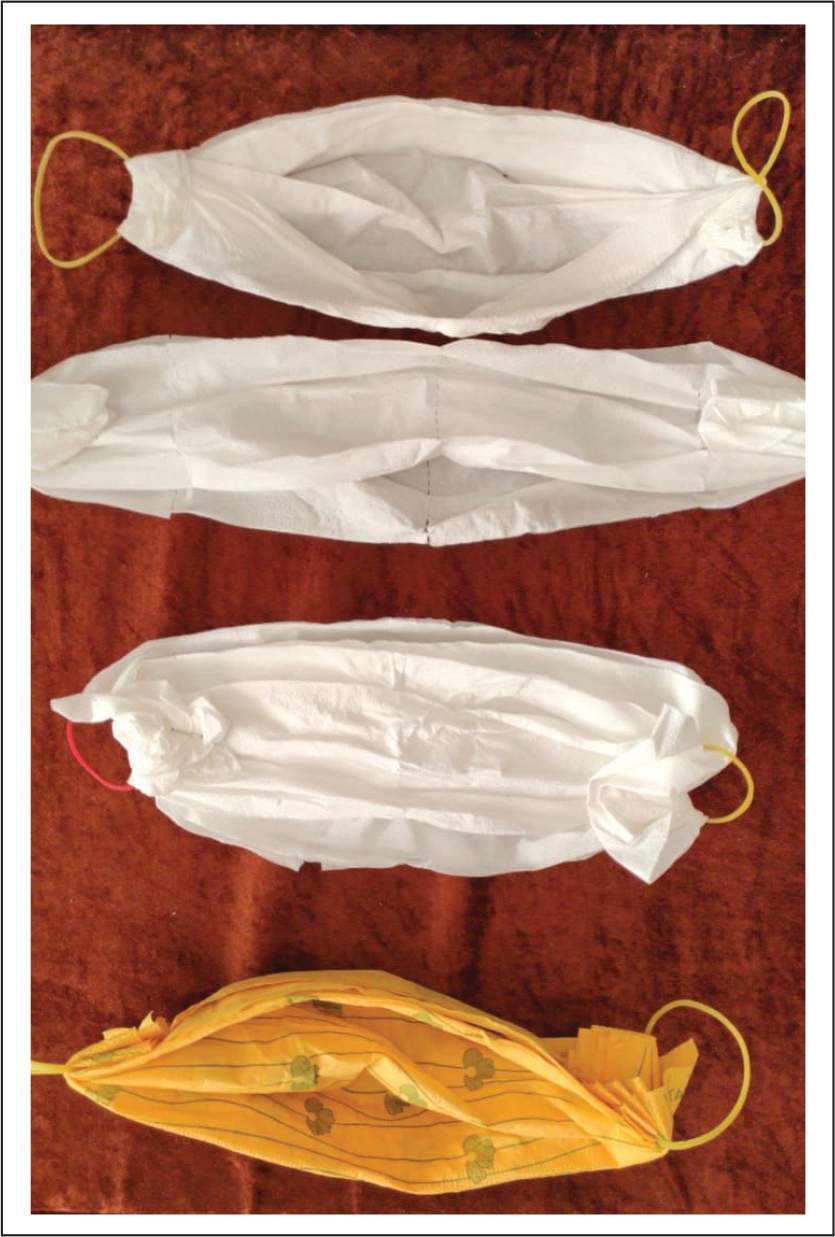
Five different masks were designed, type 1 to 5 (Figures 1 and 2).
Type 1 GAAREIP Covering Head, Eyes, Nose, and Mouth

GAAREIP 2-5: Different 1, 2, 3, 4 Layered Masks Using Cloth and Tissue Paper
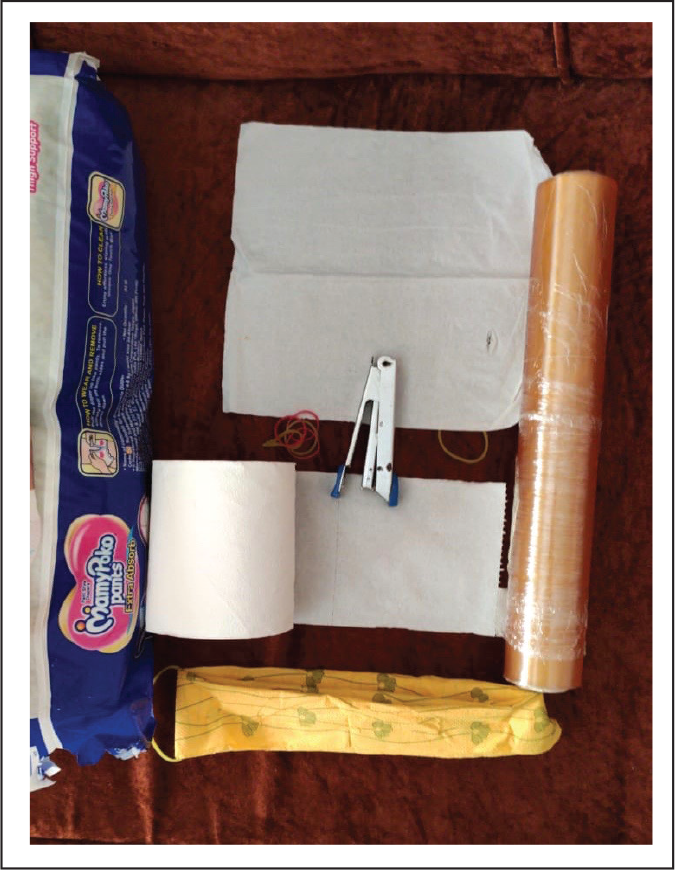
Type 1: Type 1 GAAREIPs were made with the help of a pant type diaper of varying sizes ranging from small to XXL as per the head size of individuals, which are commonly available in all NICUs, and cling wraps. A cling wrap is commonly used in neonatal care to protect neonates from hypothermia. The diaper is worn over head and the two openings are placed in front and back. The diaper covers whole of the head, face, nose, and mouth. The eyes are not covered by the diaper. The eyes are covered by a layer of cling wrap going around the head. The cling wrap is used to cover the top over the diaper. After each use the layer of cling wrap can be discarded and a new layer can be put across for reuse along with the same diaper (Figure 1). The cost for each use is approximately 5 INR. Most of the items used for type 1 category are commonly available and biodegradable (Figure 3). The model was tested in 5 adults for 4 to 5 hours to see for any difficulty in breathing and vision. All the 5 volunteers were blinded for this study and none of the 5 adults reported discomfort or any difficulty in vision with the model.
Types 2 to 5: GAAREIP Types 2 to 5 were made with the help of cotton cloth, soft tissue paper, and rubber bands. The cost was approximately 3 INR for each mask. The different masks were made by increasing layers ranging from 1 to 4 for types 2 to 5, respectively. Masks with more number of layers were likely to be safer and could be similarly used in increasing risk scenarios. Two rubber bands were stapled at the ends to help in fixing the mask. Each mask fits snugly covering the nose and mouth. The masks were tested on 5 healthy participants who were blinded to study and its outcomes, and they did not report any discomfort after 4 to 5 hours of use.
Discussion
We have tried to provide a solution to the shortage of personal protective equipment and masks by developing indigenous mask sand face-shield-cum-mask models. These are made from material that is easily available in most of the NICUs or at home. The cost of each unit is less than 5 INR and some can even be reused. Limited availability of masks and personal protective equipment has jeopardized medical care of patients and health of medical staff, in the present era of COVID-19 pandemic. According to the CDC, there is cancelation of nonurgent procedures or visits that would warrant the use of PPE, prioritization of the use of PPE for the high-risk situations, and cautious reuse of PPE.13-15 Furthermore, CDC has mentioned 3 methods for decontamination of N95 masks when supplies are critically low during a crisis These include the use of UV light, hydrogen peroxide vapor, and moist heat. There has hardly been any innovation because of lack of time and initiative,14-23 and if there has been any, it has not been published to the best of our knowledge.
Material Used in Making Different Masks
Limitations
Our model lacks clinical testing because of lack of time and ever-increasing numbers of infected patients.
Conclusion
Indigenously made, low-cost masks and personal protective equipment GAAREIP from type 1 to 5 are very practical and easy to make. They have full potential to adequately address the current and future preventive needs of health care professionals during COVID-19 and future such epidemics. Most importantly, this will induce confidence and positivity in health care workers and facilitate them to discharge their responsibilities effectively.
Footnotes
Acknowledgments
To our little stars, parents, faculty, residents, nursing staff, and other workers working in NICU. Special thanks to Dr Shivani Bajpai.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.