
Abstract
Background:
Sjögren’s disease (SS) is a chronic autoimmune disease with an estimated global prevalence of 6.9 per 100,000 person-years. However, population-based data from India are lacking. Information on reproductive health in Indian women with SS, particularly concerning marital status and pregnancy outcomes, is limited.
Objective:
To assess the impact of marital status on clinical and reproductive characteristics in women with SS and to compare pregnancy outcomes before and after disease onset among married women in India.
Methods:
This multicentre prospective observational study used data from the Indian Rheumatology Association (IRA) registry across seven centres. Female patients fulfilling the 2016 ACR/EULAR criteria for primary SS were included. Data on demographics, menstrual and reproductive history, and disease characteristics were collected using structured proformas. Reproductive health indicators were calculated using standard epidemiological methods.
Results:
Of 124 records, 115 female patients were included in the final analysis. The mean age at recruitment was 49.63 ± 10.31 years. The mean age at menarche was 13.74 ± 1.08 years, and 78.3% reported regular menstrual cycles. The mean age at disease onset was 41.34 ± 9.74 years, with a mean illness duration of 8.43 ± 5.4 years. Among married women (n = 112), there were 236 pre-disease pregnancies resulting in 212 live births, with a CFR of 1.89. Pregnancy wastage ratio was 80.51 per 1,000 pregnancies, and stillbirth and abortion rates were 4.71 per 1,000 live births and 76.27 per 1,000 pregnancies, respectively. Vaginal delivery was the most common mode. Due to the very small number of unmarried participants (n = 3) and those with pregnancy after disease onset (n = 1), comparative analysis was not performed.
Conclusion:
Reproductive events in women with SS predominantly occurred before disease onset. Marital status was associated with age at diagnosis but not with adverse reproductive outcomes.
Introduction
Sjögren’s disease (SS), a chronic autoimmune disorder characterised by lymphocytic infiltration of the exocrine glands, often affects women of childbearing age. A 2023 systematic review reported that the prevalence of primary SS is highest among females and the elderly. 1 A pooled meta-analysis estimated the global incidence of SS to be approximately 6.9 per 100,000 person-years. 2 Despite growing recognition, there are currently no robust, population-based prevalence studies from India on primary SS, and available data are largely limited to clinic-based cohorts, suggesting the condition may be underdiagnosed.
Pregnancy complications in female patients may include thromboembolic events, miscarriages, preeclampsia, intrauterine growth restriction, preterm delivery, and Caesarean delivery. 3 Studies have reported the transplacental passage of antibodies specific to SS, such as anti-Ro/SSA and anti-La/SSB antibodies. High titres of these antibodies can impair foetal cardiac development. One of the most recognised risks in neonates due to this transplacental passage is autoimmune congenital heart block (CHB). 4 Prenatal counselling is warranted in such patients to explain the associated risks and emphasise the importance of achieving disease control prior to conception. 5
There is a paucity of data from India on how marital status influences clinical presentation and reproductive outcomes in women with SS. Most existing studies are from Western populations and often do not explore the unique sociocultural and healthcare-related factors that may influence these outcomes in Indian women. The present study is intended to assess the impact of marital status on disease characteristics and reproductive outcomes in female patients with SS, and to compare pre- and post-disease pregnancy outcomes among married women diagnosed with SS in Indian settings.
Methodology
This independent, prospective, multicentre observational study considered data from patients with SS enrolled across seven centres in India through the Indian Rheumatology Association (IRA) database. Initiated in April 2020, the IRA database was established to systematically collect data on six autoimmune rheumatic diseases (AIRDs), namely rheumatoid arthritis, spondyloarthritis, psoriatic arthritis, systemic lupus erythematosus, systemic sclerosis, and SS. Participating centres were selected based on geographic representation and patient volume.
The study included both newly diagnosed and follow-up female patients with primary SS who met the 2016 classification criteria jointly established by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR). 6 Data were collected using two structured proformas. The first proforma captured demographic details, socioeconomic status, obstetric history, functional limitations, and general health-related parameters. The second focused specifically on disease-related information. Clinical research associates (CRAs) entered data based on patient responses obtained during site visits. To maintain consistency across centres, both principal investigators (PIs) and CRAs underwent online training conducted by the nodal centre. Any queries during data collection were addressed by the nodal centre’s PI.
The reproductive health data gathered were age at menarche, menstrual cycle characteristics, and menopausal status in older women. Detailed information related to pregnancy, such as number of pregnancies, number of live births, abortions, medical termination of pregnancy (MTPS), intrauterine deaths (IUDs), and mode of delivery, was recorded separately for the periods before and after the onset of SS. Marital status, including any history of divorce, was also documented. After data extraction, a rigorous cleaning process was carried out to remove records with missing reproductive health information, inconsistencies in pregnancy outcomes, or missing information on the duration of illness. Records with incomplete data across all fields were also excluded from the analysis.
Reproductive health indicators were assessed using established epidemiological formulas. These metrics included the pregnancy wastage ratio, stillbirth and abortion rates, and the cumulative fertility rate (CFR). The pregnancy wastage ratio refers to the number of stillbirths and abortions that occur per 1,000 total pregnancies. 7 Stillbirths per 1,000 live births indicate the number of stillbirths occurring for every 1,000 live births. Similarly, stillbirths per 1,000 pregnancies represent the rate of stillbirths among all pregnancies. The lifetime stillbirth rate per 1,000 women provides an estimate of the number of stillbirths experienced per 1,000 women.8,9 The abortions per 1,000 pregnancies metric indicates the number of abortions per 1,000 pregnancies. The lifetime abortion rate per 1,000 women reflects the number of abortions per 1,000 women in the population. 10 The CFR is defined as the total number of live births per woman. 11
Sample Size Calculation
For the comprehensive analysis of the six AIRDs, an estimated total sample size of 6,500 patients was determined, based on the reported prevalence of each condition. 12 The sample size for each disease was allocated proportionally according to its individual prevalence. In the case of SS, with an estimated prevalence of 10 per 100,000, the target sample size was approximately 96 participants. 13
Statistical Analysis
Stratified analyses were planned to compare reproductive outcomes before and after the onset of SS, focusing on parameters such as pregnancy wastage ratio, stillbirth and abortion rates, CFR, and pregnancy-related complications. However, a meaningful comparison was not feasible, as only one participant reported a pregnancy following disease onset. The influence of marital status on reproductive health indicators was also examined. Variables analysed included age at recruitment, age at menarche, menstrual regularity, age at marriage, duration of marriage, estimated illness duration, and age at disease onset. Statistical comparisons were made between married and unmarried individuals, as well as between pre- and post-disease onset data.
Descriptive statistics were employed, with categorical variables represented as percentages, and continuous variables summarised using mean ± SD. All tables were generated using Microsoft Excel (version 2409, build 16.0.18025.20030). Statistical analyses were conducted using SPSS version 29.0.2.0 and Python version 3.8.3.
Results
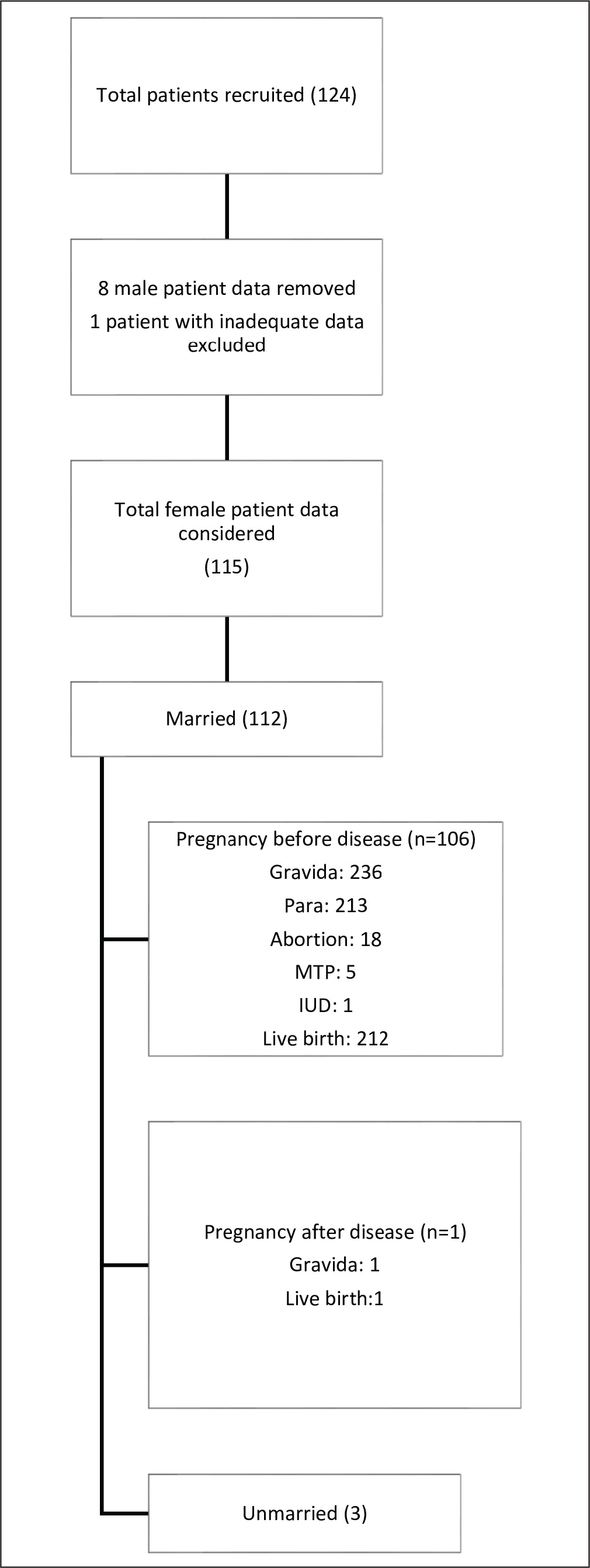
Out of a total of 124 records initially identified as SS patients, data of 8 male patients were excluded, resulting in 116 female patients. Subsequently, one record was excluded due to inadequate data. Thus, the final sample size included in the analysis was 115 female patients. The distribution of patients across cohorts is shown in Figure 1.
Distribution of Patient Population to Different Cohorts.
The mean age at recruitment for the overall cohort was 49.63 ± 10.31 years, ranging from 20 to 72 years, indicating that the majority were middle-aged women. The average age at menarche was 13.74 ± 1.08 years. Most participants (78.3%) reported regular menstrual cycles, while 13% had irregular cycles, and data were unavailable for 8.7%. The mean age at disease onset was 41.34 ± 9.74 years, with a range from 17 to 61.42 years. The probable duration of illness varied widely, with a mean of 101.3 months (approximately 8.4 years). The average age at marriage was 20.65 ± 3.19 years, ranging from 13 to 30 years.
Reproductive Outcomes of Married and Unmarried Cohorts
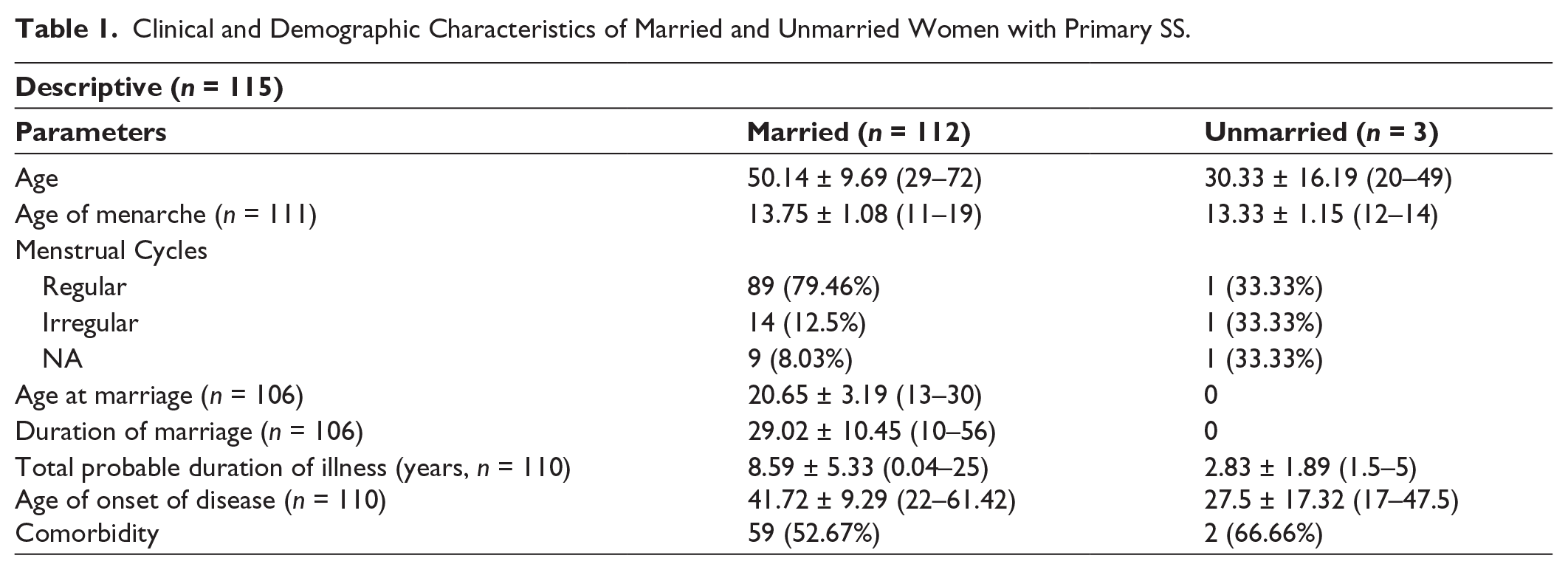
The descriptive analysis was conducted on 115 participants to assess clinical and demographic parameters among married (n = 112) and unmarried (n = 3) women. No comparison between the married and unmarried groups was performed due to the small sample size of the unmarried group. The mean age was 50.14 ± 9.69 years among married women and 30.33 ± 16.19 years among unmarried women. The mean age at menarche was similar across both groups, recorded as 13.75 ± 1.08 years in married women and 13.33 ± 1.15 years in unmarried women. Regular menstrual cycles were reported by 79.46% of married women and 33.33% of unmarried women. Data on age at marriage and duration of marriage were available only for the married group, with a mean age at marriage of 20.65 ± 3.19 years and a mean duration of marriage of 29.02 ± 10.45 years. The total probable duration of illness was 8.59 ± 5.33 years among married women and 2.83 ± 1.89 years among unmarried women. The mean age of disease onset was 41.72 ± 9.29 years in married women and 27.5 ± 17.32 years in unmarried women. Comorbidities were present in 52.67% of married women and 66.66% of unmarried women (Table 1).
Clinical and Demographic Characteristics of Married and Unmarried Women with Primary SS.
Reproductive Outcomes Before and After Disease Onset
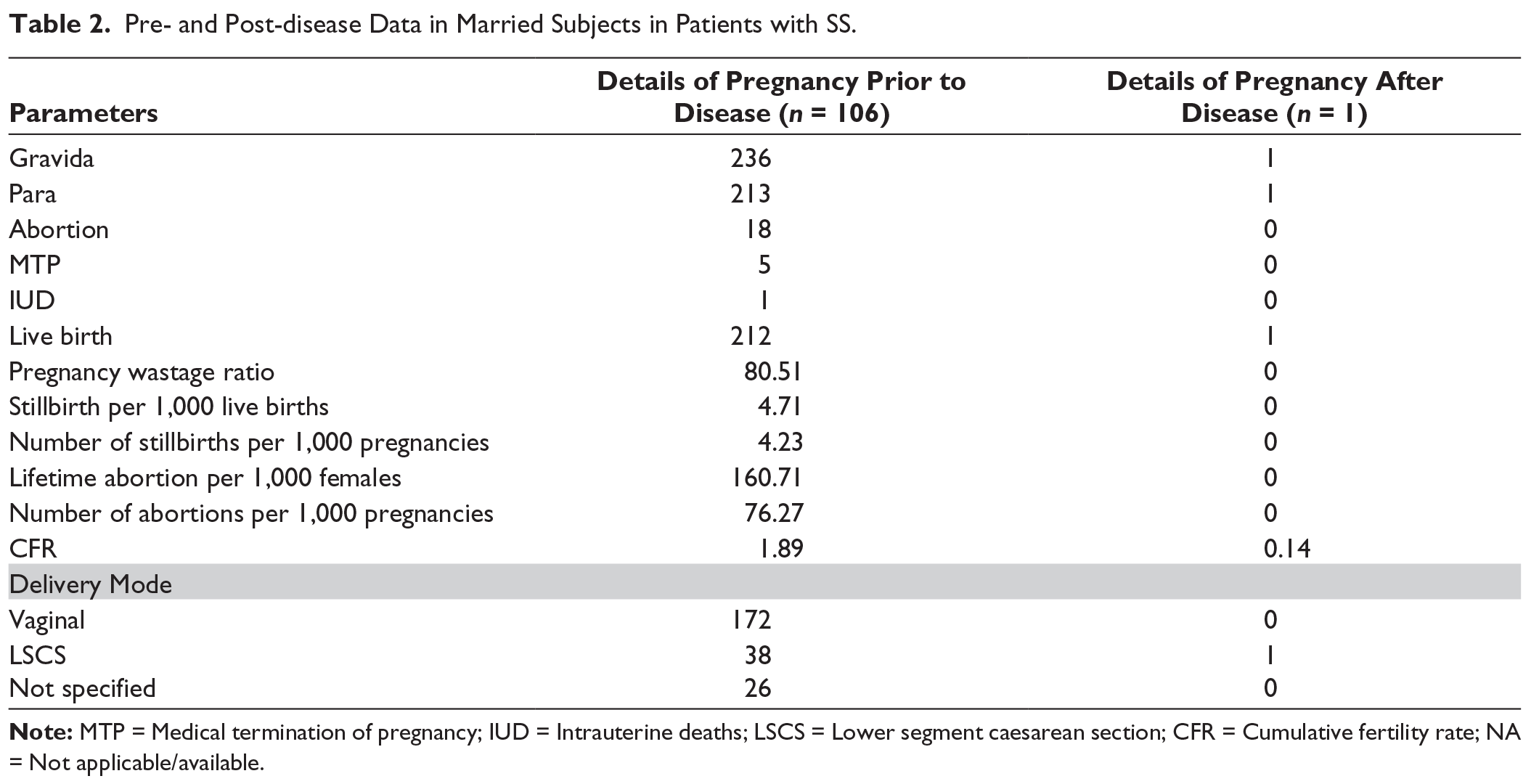
Details of pregnancies prior to disease (n = 106) and after disease (n = 1) were not compared, as only a single pregnancy occurred after disease onset. Before disease onset, data from 106 participants documented 236 pregnancies, resulting in 212 live births and a CFR of 1.89. Reported outcomes included 18 abortions, 5 MTPs, and one IUD (Table 2). The pregnancy wastage ratio was 80.51 per 1,000 pregnancies, with stillbirth and abortion rates of 4.71 per 1,000 live births and 76.27 per 1,000 pregnancies, respectively. Among pre-disease pregnancies, vaginal delivery was the most common mode (172 cases), followed by lower segment Caesarean section (LSCS, 38 cases), with 26 cases having unspecified delivery mode. The single post-disease pregnancy resulted in one live birth via LSCS, yielding a CFR of 0.14. No cases of pregnancy-induced hypertension (PIH), small-for-gestational-age (SGA) infants, preeclampsia, or CHB were reported in either group. Details of the calculation of reproductive health indicators are provided as supplementary data.
Pre- and Post-disease Data in Married Subjects in Patients with SS.
The pattern of autoantibody positivity in the cohort was dominated by antinuclear antibody (ANA) and anti-Sjögren’s-disease-related antigens (anti-SS-A, anti-SS-B, and anti-Ro-52). ANA positivity was observed in 60 cases. Anti-double-stranded DNA (anti-dsDNA) antibodies were detected in three patients. The most frequent extractable nuclear antigen (ENA) antibodies were anti-SS-A (36 patients), followed by anti-Ro-52 (22 patients) and anti-SS-B (20 patients). Low-level positivity was also seen for anti-RNP/Sm (3 patients), anti-Sm (2 patients), anti-Scl-70 (2 patients), anti-PM-Scl (2 patients), anti-Jo-1 (1 patient), anti-CENPB (1 patient), anti-PCNA (2 patients), and anti-ribosomal P protein (1 patient).
Antiphospholipid antibody testing revealed borderline positivity for anticardiolipin immunoglobulin M (IgM) and immunoglobulin G (IgG) in two patients each, while β2-glycoprotein I antibodies and lupus anticoagulant were negative. Antineutrophil cytoplasmic antibodies (ANCA), including proteinase 3 (PR3) and myeloperoxidase (MPO), were negative in all patients. Thyroid-stimulating hormone (TSH) elevation in three patients indicated possible subclinical thyroid dysfunction in a minority. The presence of autoantibodies had no impact on reproductive outcomes.
Discussion
This study provides important insights into the reproductive and demographic profile of women with SS. The mean age at disease onset was approximately 41 years, and the majority of patients were middle-aged women. These findings are consistent with existing literature indicating that SS commonly emerges in early to mid-adulthood, particularly among women. A systematic review by Thurtle et al., which screened 3,510 records, reported that symptom onset typically occurs between the ages of 34 and 57 years, with diagnosis often taking place between 40 and 67 years. 1 Furthermore, SS is generally diagnosed in the fifth decade of life, with the mean age at diagnosis ranging from 51.6 ± 13.8 to 62 ± 13 years. However, initial symptoms often appear several years before formal diagnosis, highlighting the chronic and insidious nature of the disease. 14
The mean age at menarche in the current cohort was 13.74 ± 1.08 years, which is comparable to the age range reported for Indian women. For instance, data from the Indian Human Development Survey indicated a national mean age at menarche of 13.76 ± 1.2 years in 2005. 15 Similarly, a South India-based study by Omidvar et al. (2018) involving Indian adolescent females reported a mean age of 13.0 ± 1.1 years, with around 73% of participants experiencing regular menstrual cycles. 16 In line with these findings, most participants in the present study (78.3%) also reported regular menstrual cycles, suggesting preserved reproductive endocrinology prior to the onset of SS.
Almost all pregnancies in the current cohort occurred prior to the diagnosis of SS, with only one post-diagnosis pregnancy documented. This may be attributed to the mean age at disease onset (~41 years), by which time most women would have completed their reproductive years, particularly in the Indian context, where women tend to marry and conceive at an earlier age. Supporting these observations, a case-control study by Haga et al., involving 58 women with primary SS and 157 matched controls, reported that the majority of pregnancies occurred before SS diagnosis. The study found no significant differences in pregnancy outcomes prior to diagnosis, with only one case of CHB reported. 17 Similarly, a larger case-control study of 19 women with primary SS (54 pregnancies) and 216 matched controls observed that pregnancies occurring after SS diagnosis were associated with higher rates of spontaneous abortion (30% vs. 0.4%) and significantly lower birthweight percentiles, whereas outcomes of pregnancies prior to diagnosis were largely comparable to those of healthy controls. 18
Pre-disease pregnancies demonstrated generally favourable outcomes, with a high live birth rate (212 out of 236 pregnancies) and a low cumulative pregnancy wastage of 80.51 per 1,000 pregnancies. The CFR prior to the onset of SS was 1.89, which is slightly below the national average and may indicate mild pre-existing subfertility in this group. According to the 2025 estimates from the Indian Census and Family Welfare statistics, the general fertility rate in the Indian population is approximately 2.11 births per woman. 19 This suggests that the studied population experienced somewhat reduced reproductive outcomes even before being diagnosed with SS. Despite this, no major obstetric complications such as PIH, preeclampsia, SGA infants or CHB were reported either before or after disease onset, indicating relatively safe pregnancy outcomes. Vaginal delivery was the most common mode of childbirth (72.88%), while Caesarean sections accounted for approximately 16% of deliveries, consistent with national trends.
Compared to previous studies reporting adverse pregnancy outcomes in women with primary SS, the current study indicates minimal impact on reproductive outcomes when pregnancies occur prior to disease onset.20,21 Moreover, none of the pregnancies in this cohort reported CHB, underscoring this positive finding. A retrospective study conducted by Paladugu et al. in the Indian context reported 16 pregnancies in 10 women with primary SS, with high rates of complications including oligohydramnios (11.8%), intrauterine foetal demise (11.8%), first-trimester medical termination (23.5%), and a 50% incidence of CHB, attributed to the transplacental passage of maternal anti-SSA/SSB antibodies. 22 In contrast, the present cohort of 115 women with SS demonstrated a high pre-disease live birth rate (212 out of 236 pregnancies), low cumulative pregnancy wastage (80.51 per 1,000), and no cases of PIH, preeclampsia, SGA infants, or CHB. Only one pregnancy in this study occurred after SS onset. These contrasting findings highlight the critical role of disease timing in determining pregnancy outcomes, with conception prior to disease onset being associated with better maternal and foetal health.
The present findings hold significant relevance given the limited Indian data on fertility outcomes in women with SS before and after disease onset. The study suggests that while active SS during pregnancy carries substantial risks, the impact is likely minimal when pregnancies occur prior to the clinical manifestation of the disease. This underscores the importance of individualised counselling, timely diagnosis, and comprehensive risk assessment in reproductive planning for women with autoimmune conditions.
The major strengths of the study include its prospective multicentre design, inclusion of both newly diagnosed and follow-up cases, and standardised data collection using structured proformas through the IRA database. The training of site personnel and centralised oversight enhanced data consistency and reliability. A notable methodological strength is the detailed stratification of reproductive events before and after disease onset, allowing for meaningful epidemiological comparisons. However, the study has several limitations. The small number of post-disease pregnancies (n = 1) severely limits comparative analysis and the generalizability of findings related to pregnancy outcomes after SS onset. Additionally, potential recall bias due to retrospective reporting of reproductive history, limited representation of unmarried participants, and lack of longitudinal follow-up data limit broader interpretation. Despite these limitations, the study lays an important foundation for future research on SS as well as autoimmune disease and reproductive health in Indian women.
Conclusion
Analysis of reproductive outcomes before and after disease onset highlights that the majority of pregnancies occurred prior to an SS diagnosis, with largely favourable outcomes. However, the near absence of post-disease pregnancies raises potential concerns regarding fertility or pregnancy planning following diagnosis. These findings underscore the importance of early reproductive health counselling for women diagnosed with SS and reinforce the need for prospective longitudinal studies to better understand fertility patterns, pregnancy outcomes, and associated risks in this population.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Dr Debhashish Dhanda and Dr Aman Sharma for their participation in the administrative role in the IRA database. The authors acknowledge the help of Research Assist (
Authors’ Contribution
Dr Chandrashekara S, Dr Padmanabha Shenoy, Dr Uma Kumar, Dr Sapan Pandya, Dr Alakendu Ghosh, Dr Apurva Khare, Dr Rajkiran Dudam, and Dr Rudra Prosad Goswami contributed equally to the conceptualisation, data collection, and development of the manuscript. Each author participated in the analysis and interpretation of the data and was actively involved in drafting the manuscript and revising it critically for important intellectual content. All authors have reviewed and approved the final version of the manuscript to be published. Additionally, all authors agree to be accountable for all aspects of the work, ensuring the accuracy and integrity of any part of the work is appropriately investigated and resolved. They collectively take full responsibility for the integrity and accuracy of the work.
Availability of Data and Materials
Data will be provided on request.
Declaration of Conflicting Interests
Padmanabha Shenoy and Rajkiran Dudam are Associate Editors in the journal. Sapan Pandya, Uma Kumar, Alakendu Ghosh and Arghya Chattopadhyaya are members of the National Editorial Board of the journal. None of them were involved in the decision making process related to this manuscript.
Ethical Approval
Ethical approval for the study was obtained from multiple institutional ethics committees prior to initiation. Approval was granted by the Ethics Committee of ChanRe Rheumatology and Immunology Center and Research (Protocol No. IEC-CRICR-132/101/2020; approved on 05 October 2020), Sree Sudheendra Medical Mission (approved on 12 September 2020), the All India Institute of Medical Sciences (Protocol No. IEC-59/03.07.2020. RP-462020; approved on 15 July 2020), the Ethics Committee of Care Institute of Medical Sciences (approved on 25 July 2024), the Institute of Postgraduate Medical Education and Research (Protocol No. IPGME&RC/ IEC/2020/478;
approved on 16 June 2020), the International Ethics Committee of LN Medical College and JK Hospital (Protocol No. LNMC&RC/Dean/2020/Ethics/146; approved on 07 August 2020), and the S2J Independent Ethics Committee (approved on 20 July 2021). Written informed consent was obtained from all participants in accordance with institutional guidelines.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Educational and research grants from Novartis India for developing a database for the Indian Rheumatology Association.
Informed consent
Written informed consent was obtained from all selected patients following institutional guidelines.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.