
Abstract
Aim:
The lack of knowledge among primary care physicians about autoimmune rheumatic diseases can contribute to referral delays by impeding early recognition, accurate diagnosis and timely referral to specialists. The present study is aimed at analysing the factors influencing the diagnostic and referral delay in patients with systemic lupus erythematosus (SLE) to the rheumatology speciality in India.
Results:
The study considered 786 out of 833 patients fulfilling the Systemic Lupus International Collaborating Clinics criteria. The median delay in referral to a specialist was 1 month, with an interquartile range of 11 months, but the delay ranged from 1 to 192 months. The major causes of referral delay were the management of SLE by other specialists instead of rheumatologists (93%) and a lack of awareness of speciality care (89%). Additionally, more than 25% of primary care practitioners were unaware of rheumatology as a speciality, and a similar percentage of patients received incorrect diagnoses from their general care physician. Early referral within 6 months was associated with a lower prevalence of systemic complications, including pulmonary, gastrointestinal, peripheral vascular, central nervous system and ophthalmic involvement. Significant predictors for early referral included joint pain (49.51% vs. 19.64%; P = .013; odds ratio [OR] = 0.655), hair loss (12.76% vs. 4.76%; P = .279; OR = 0.789) and weight loss (5.05% vs. 1.12%; P = .053; OR = 0.469). Conversely, symptoms such as lung involvement (0.56% vs. 0.98%; P = .042; OR = 3.938), Raynaud’s phenomenon (0.14% vs. 0.98%; P = .002; OR = 15.847) and thrombocytopenia (0.84% vs. 1.12%; P = .035; OR = 3.002) were more likely to lead to referrals to other specialities.
Conclusion:
The delay in patient referral to the rheumatology speciality is primarily attributed to referrals to other specialities and a lack of knowledge about rheumatology. Educating primary care physicians and facilitating direct referrals to specialists could significantly contribute to reducing these delays.
Introduction
Autoimmune rheumatic diseases (AIRDS) are a group of chronic and persisting heterogeneous diseases affecting 3%–5% of the population and constitute one of the major proportions of the non-communicable disease burden. 1 Diseases such as systemic lupus erythematosus (SLE) have demonstrated better treatment outcomes under the speciality care of trained rheumatologists and immunologists. Schlencker et al. 2 reported excessive diagnostic delay and the lack of coordinated care as the major challenges in the management of SLE. The availability of rheumatologists and the awareness and attitude of both patients as well as primary care physicians are the key factors influencing the early referral and utilisation of speciality care. 2 One of the major challenges in the primary care setting is the limited knowledge among physicians about the complexities of AIRDS, which may lead to misdiagnosis or underdiagnosis. Patients may undergo unnecessary tests or treatments, prolonging the time to accurate diagnosis and initiation of appropriate care.
The delay in referral and management of patients with AIRDS can cause significant mortality and morbidity, as the undiagnosed disease may lead to prolonged disease activity and associated sequelae. Bruce et al. 3 reported that the diagnostic delay in SLE may result in reduced quality of life, fatigue and increased mortality. It is often difficult to define a definite cut-off period for delay in diagnosis and referral. Certain studies have investigated delay from the point of first attributable symptom to diagnosis as the cut-off, while others have suggested the time required to reach the speciality. In certain cases, patients with timely diagnoses might not have obtained the appropriate speciality care. Even a delay of 24 hours could be disastrous for acute rapidly progressing disorders like SLE. Based on several factors, the present study arbitrarily considered 6 months as a delay in accessing speciality care. Studies have reported different time points regarding delay in referral and diagnosis ranging from weeks to months. The number of trained specialists in the field of rheumatology, required to cater to the population in India, has improved in recent years. However, they are still inadequate to provide optimal care. 4
In addition to the accessibility and availability of speciality care, several factors impact the number of patients seeking speciality care. These can be broadly categorised into (a) patient-related factors (beliefs, self-care, education, socioeconomic status, demographics, disease awareness and affordability), (b) primary care or referring physician-related factors (speciality knowledge and diagnostic capabilities) and (c) disease-related factors (clinical presentation). The present study is intended to evaluate the factors influencing the diagnostic and referral delay in patients with SLE in India. The study findings may help in stratifying the interventions to improve early diagnosis and access to speciality care.
Material and Methods
Registry/Database Design and Study Population
The independent, multi-centre, database-based cross-sectional study gathered data from seven centres across India through the Indian Rheumatology Association (IRA) database. The centres were selected based on their geographic location, and data were collected from patients diagnosed with the following six autoimmune diseases: rheumatoid arthritis (RA), spondyloarthritis (SpA), psoriatic arthritis (PsA), SLE, scleroderma and progressive systemic sclerosis (SSc). This study focused on young and adult patients with SLE who met the Systemic Lupus International Collaborating Clinics (SLICC) criteria.5,6 The database, initiated in April 2020, included both newly diagnosed and follow-up patients. The following two structured proformas were used for data collection: the first captured demographic, socioeconomic, functional, obstetric and health-related details, while the second focused on disease-specific information. Questions for data collection were designed by experts who had trialled the database. Clinical research associates (CRAs) completed the proformas based on patient responses. To maintain consistency, both principal investigators (PIs) and CRAs received online training coordinated by the nodal centre, with any data-related queries directed to the PI at the nodal centre. Ethical clearance was obtained from the institutional committees of all participating centres (enclosed as a Supplementary File). Written informed consent was obtained from all the selected patients prior to the study, as per the respective institutional recommendation. Patients with inconsistent or incomplete data were not considered for the study.
Sample Size Calculation for Registry
The minimum required number of subjects with AIRDs for comparison was determined with the primary goal of assessing the clinical and laboratory profiles of six AIRDs based on the reported prevalence of each disease. The estimated total number of patients needed for the analysis was 6,500. 7 Given the cross-sectional study design and the selection of patients from those seeking rheumatology care, the prevalence of all AIRDs among individuals with musculoskeletal symptoms was approximated at 10%. 8 The calculated P value was set at .01, with a Z-score of 2.59 for a 99% confidence interval and an estimated precision (d) of 0.01. Using these parameters, the required sample size was calculated to be 6,037. To account for potential dropouts and missing data, a buffer was added, resulting in a final estimated sample size of 6,500. 9 The sample size for each disease was estimated based on the prevalence of each autoimmune disease, with a proportionate sample considered for each disease. For SLE, accounting for 0.6 per 1,000, the estimated number was approximately 600.
Data Collection and Definitions Specific to Delay
To explore the factors contributing to delayed access, the study assessed the time taken to reach tertiary care from the onset of the first symptom or sign attributable to SLE. A 6-month period was set as the threshold for defining referral delay or delayed access to tertiary care. In cases where patients had previously consulted a rheumatologist at a private clinic before arriving at a tertiary centre, their initial visit to the rheumatologist was considered when estimating the referral delay. The study focused on the patient’s first interaction with speciality care rather than the timing of the diagnostic conclusion, whether made prior to or within the rheumatology department.
Each patient was interviewed and evaluated by the research team to explore the factors contributing to delays in accessing care. The patient-related factors examined included their trust in modern medical care, lack of awareness about the rheumatology speciality, socioeconomic challenges (such as affordability and the distance to a speciality centre) and concerns about potential adverse effects of modern treatments. Referral factors, as reported by the patients, included the following: primary care providers either did not refer patients to a rheumatologist or were hesitant to do so; patients were accurately diagnosed but referred to other specialities like nephrology, dermatology or orthopaedics; primary care physicians were unaware of the rheumatology speciality; and patients were either unaware of their diagnosis or lacked proper documentation. In cases where the cause could not be determined despite considering all relevant factors, it was recorded as ‘not ascertainable’. Socioeconomic status was classified using the modified Kuppuswamy scale, which evaluates income, education and occupation. 10 The earliest symptoms and presentation significantly influence the referral process. Symptoms attributable to SLE were considered, along with clinical presentation and systemic involvement, for the analysis. The earliest symptom or sign documented and attributable to SLE, as per the criteria and clinical association determined by the PI, was considered. Symptoms such as joint pain and malar rashes, among others, were included in the analysis.
Statistical Analysis
Descriptive analysis was conducted using Microsoft Excel. The factors contributing to delays were compared using a t-test for continuous variables, while categorical variables were analysed with the chi-square test and Fisher’s exact test.11,12 Missing data, particularly those with no discernible causes, were excluded from the analysis, presuming them to be unrelated to the anticipated cause. Subjects were divided into patients referred to rheumatology speciality within 6 months and those referred >6 months for the comparison of systemic involvement and patients’ first clinical presentation. Logistic regression analysis was also performed to evaluate the likelihood of patients being referred to rheumatology speciality care based on various symptoms. The analyses were carried out using Statistical Package for the Social Sciences (SPSS, IBM, version 29.0.0).
Results
The study included 786 patients with SLE, with a mean age of 37.48 years and a gender distribution of 65 males and 721 females. The median duration of illness was 72 months, with an interquartile range (IQR) of 84 months. The duration varied widely, from as short as 1 month to as long as 480 months. The median delay in referral to a specialist was 1 month, with an IQR of 11 months, but the delay ranged from 1 to 192 months. Approximately 67% of patients accessed speciality care within 6 months, 20% between 6 and 24 months and 13% after 24 months. Management of SLE by other specialists instead of rheumatologists (93%) and lack of awareness of speciality care (89%) were the major reasons for the delay in diagnosis. In addition, >25% of primary care clinicians were unaware of the rheumatology speciality, and nearly 30% of the cases were misdiagnosed by the primary care physician (Table 1).
Demographic Distribution of SLE and Evaluation of the Causes of Diagnostic Delay.
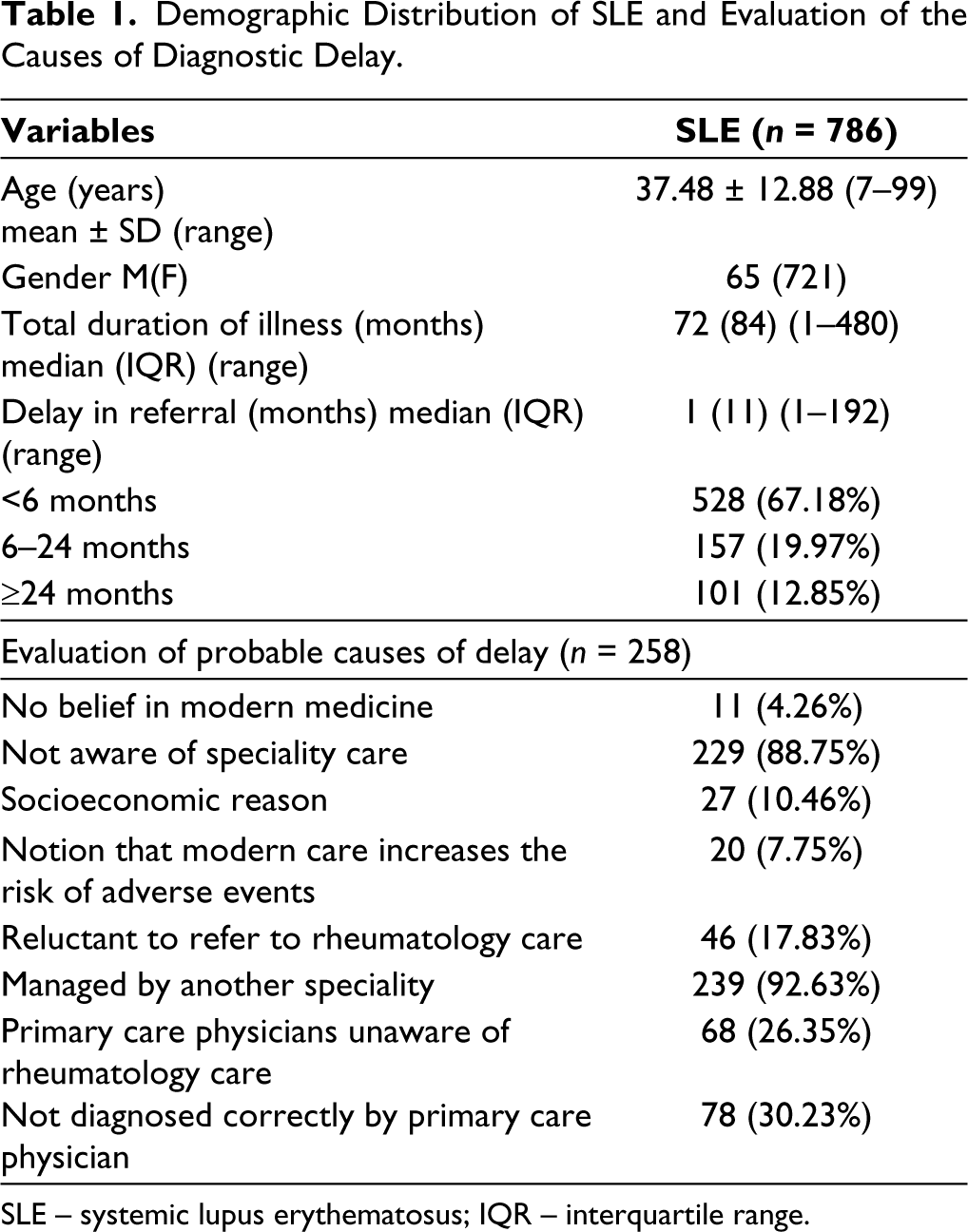
SLE – systemic lupus erythematosus; IQR – interquartile range.
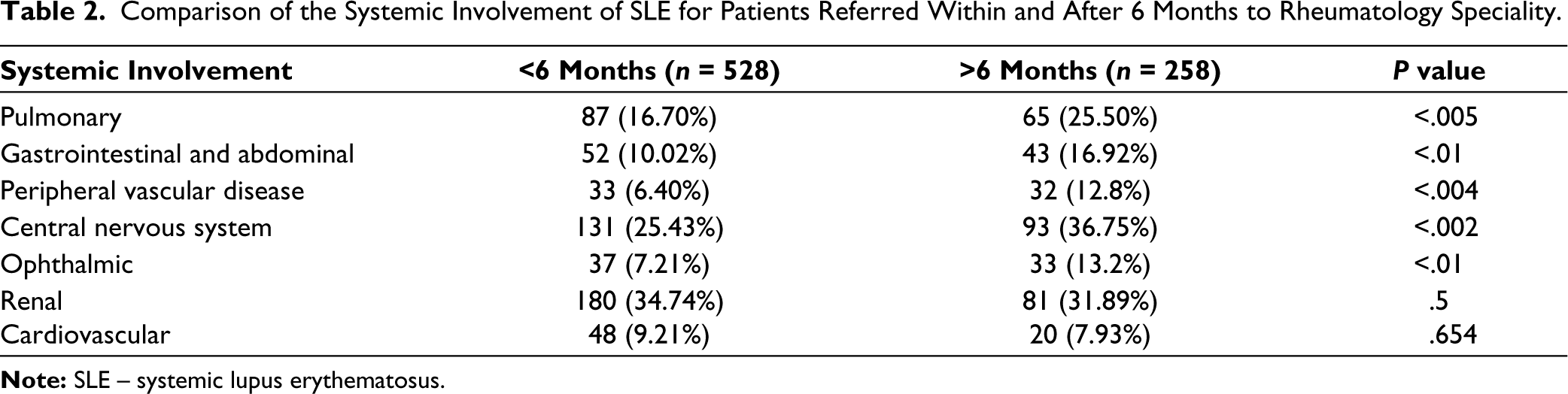
Analysis of the active systems involved in patients at the time of recruitment indicated that early referral within 6 months was associated with lower prevalence rates of systemic involvement. Statistically significant differences between patients referred within and after 6 months to rheumatology speciality were observed for pulmonary, gastrointestinal, peripheral vascular, central nervous system and ophthalmic involvement (Table 2). The differences noted in monthly income and economic strata demonstrated the potential influence of socioeconomic status on the timing of referrals to rheumatology speciality (see details provided in Supplementary Table 1).
Comparison of the Systemic Involvement of SLE for Patients Referred Within and After 6 Months to Rheumatology Speciality.
Analysis of the impact of the earliest attributable symptom of SLE revealed that patients with joint pain were more likely to be referred to speciality care within 6 months (49.51% vs. 19.64%; P = .013; odds ratio [OR] = 0.655). Similar findings were noted for those with hair loss (12.76% vs. 4.76%; P = .279; OR = 0.789) and weight loss (5.05% vs. 1.12%; P = .053; OR = 0.469). However, patients with lung involvement (0.56% vs. 0.98%; P = .042; OR = 3.938), Raynaud’s phenomenon (0.14% vs. 0.98%; P = .002; OR = 15.847) and thrombocytopenia (0.84% vs. 1.12%; P = .035; OR = 3.002) were more likely to be referred to other specialities within 6 months. Logistic regression analysis supported these findings, revealing that patients with fever, joint pain, fatigue, kidney involvement and weight loss were more likely to be referred to rheumatology speciality care within 6 months (see details provided in Supplementary Tables 2 and 3).
Discussion
The present study has noted that 67% of the patients with SLE accessed speciality care within 6 months, and the average delay in diagnosis noted was around 5 months. The aggressive nature of the disease could be one of the factors influencing the early referral of SLE to speciality care compared to the data from other secondary care centres. Management of SLE by other specialists and lack of awareness of speciality care among primary care physicians were identified as the major reasons for the delay in SLE diagnosis. Socioeconomic factors also influenced the utilisation of the rheumatology speciality.
Numerous factors contribute to the optimal management of AIRDS, with primary care physicians playing a central role as they are often the initial and frequent point of contact for patients. A 2023 study by Chatterjee and Aggarwal 13 suggested that inadequately staffed primary and secondary healthcare centres could be contributing to ineffective referrals, resulting in diagnostic delays. The present study findings corroborate this in the Indian context. Furthermore, the majority of primary care physicians possess limited knowledge about SLE. Gergianaki and Bertsias 14 underscored the importance of multidisciplinary shared-care pathways involving collaboration between specialists and different levels of care (primary, secondary and tertiary) for the optimal clinical management of patients with SLE.
The delay in referral in AIRDS has been reported by studies across the globe, but the reasons are often zone-specific.15–17 In underdeveloped countries like Africa, SLE is underestimated due to poor healthcare access, low awareness and lack of speciality care. 17 The median diagnostic delay noted in SLE in Africa was approximately 2 years, and worsening of intervention/comorbidities and diagnostic delay were the key factors that contributed to increased mortality in such patients. 18 Patients with SLE who had an early diagnosis in <6 months had lower disease flares than those who had a late diagnosis. 19
The current study highlighted that delayed referral to rheumatology is linked to a higher incidence of systemic complications in SLE, including pulmonary, gastrointestinal, peripheral vascular, central nervous system and ophthalmic involvement. Analysis of initial symptoms associated with referral delays reveals that patients presenting with joint pain, fever, fatigue and renal involvement are more likely to be referred to a rheumatology speciality. In contrast, patients with classical skin rashes and mucocutaneous involvement were 10%–20% less likely to be referred to rheumatology, although this difference was not statistically significant. Symptoms like lung involvement, Raynaud’s phenomenon and thrombocytopenia often led to referrals to other specialities rather than directly to rheumatology. This trend may reflect a lack of awareness or a lower index of suspicion for SLE in these contexts, potentially resulting in delays in appropriate management and impacting overall disease outcomes. Logistic regression analysis corroborated these findings, indicating that fever, joint pain, fatigue, kidney involvement and weight loss are significant predictors of early referral to rheumatology speciality care.
The median delay noted in an England-based study from the appearance of the first musculoskeletal symptom to SLE diagnosis was 26.4 months (IQR: 9.3–43.6). The diagnosis was delayed with increasing age and less severe disease. 20 In a study from the USA, misclassification of diagnosis either to RA or SLE was found in 44.6% of the subjects. Age and investigation results significantly influenced the diagnosis, whereas no significant delay in concluding the diagnosis was noted for rheumatic disease. 21
According to the current study results, over 93% of patients were managed by specialists other than rheumatologists. This could be attributed to either the referral of primary care physicians to other specialities or patients themselves seeking care from other specialists. An observational study published in Saudi Arabia observed a delay of less than 1 month in seeking primary care in 68.2%, while it was around 33.4% for patients seeking speciality care. Furthermore, the delay exceeded 1 year in 25.8% of patients. Over 80% of the SLE diagnosis was made by rheumatologists, and the delay was more predominant in dermatology, orthopaedics and primary care. 22 An Italian study reported a median (IQR) total delay of 24 (54) months between symptom onset and SLE diagnosis. Only 28.4% of diagnoses were made within 6 months, while 55.6% were made after 12 months. 23 In contrast, the present study observed a median delay in referral to a specialist of just 1 month, with an IQR of 11 months, although the delay varied from 1 to 192 months. This discrepancy may be attributed to differences in referral systems between regions. In European countries, well-defined referral strategies facilitate timely access to secondary and tertiary care. In India, major obstacles to appropriate referrals include the lack of strict regulations on the referral system, which often results in minor cases being directed to secondary or tertiary care hospitals. Additionally, the absence of universal initial screening methods for directing patients to secondary and tertiary specialities further complicates the situation. 24
Schlencker et al. 2 identified six thematic clusters for the optimisation of patient pathways in SLE. The researchers have recommended the implementation of an appropriate and timely referral strategy, dedicated consultation and coordinated care based on disease activity, severity, organ involvement and patient care. The practical implementation of structured referral strategies in India is challenging, with only a few organisations mandating speciality referrals before consultations with specialists. To address these challenges, it is crucial for regulators and stakeholders, including professional organisations like the IRA, to develop and implement guidelines or tools that facilitate more appropriate and timely referrals.
The present study findings also showed that nearly 25% of primary care physicians were unaware that diseases like SLE were managed in rheumatology specialities, and a quarter of subjects were misdiagnosed under primary care. According to a recent single-centre retrospective analysis, 7%–17% of patients with early SLE were misclassified utilising just one of the three sets of criteria—European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) 2019, SLICC 2012 or ACR 1982/1997.5,25,26 However, combined use of all three sets ensured the correct classification of 94%–98% of patients. 26 Due to the absence of specific diagnostic criteria, SLE classification criteria are often used in clinical practice to identify some of the disease-specific clinical features for concluding the diagnosis. The aforementioned literature studies have also underscored the lack of consensus on the exact time frame between the onset and disease diagnosis for SLE. Early diagnosis based on clinical and laboratory characteristics and referral to speciality care is warranted to customise the course of treatment, thereby improving the treatment outcomes.
The current study found that over 50% of patients were directed to other specialities, while 5%–8% of patients were sceptical regarding modern medical care. Addressing the misconception that modern medicine carries higher risks and educating patients about medical care can help overcome these obstacles through counselling and education. The accessibility was slightly higher for patients with SLE with higher education status and those belonging to upper socioeconomic strata. The accessibility of speciality care was not significantly affected by the affordability, as data were collected from both public fund-supported institutions and the private sector.
Similar studies conducted by the current authors on RA SpA, SSc and Sjögren’s syndrome (accepted for publication) revealed a significant delay in seeking rheumatology speciality care in Indian settings. Nearly 50% of the PsA subjects availed of speciality care within 6 months, whereas it was only 35% among SpA patients. 27 More than 60% of the patients with SSc and Sjögren’s syndrome had availed rheumatology speciality care after 6 months of disease onset. For RA, approximately 39% of patients were referred to rheumatology within 6 months of disease onset, while 26% reported later, with 34% reporting over 2 years. In the present study, approximately 67% of patients with SLE accessed speciality care within 6 months. The mean referral delay noted in PsA and SpA subjects was 16.3 ± 34.35 months and 17.48 ± 33.59 months, respectively. Patients with SSc were referred to speciality care 10.63 ± 24.67 months after the onset of the first attributable symptom, whereas the mean delay in referral was 5.91 ± 44.47 months for Sjögren’s syndrome.27–29 The earlier referral of SLE noted in the current study, compared to other rheumatic diseases such as RA, SpA, Sjögren’s syndrome and scleroderma, could be attributed to the aggressive nature of the disease and its more distinctive features.
The major strengths of the current study include multi-centre data collection, larger sample size and involvement of both academic and private settings, which allowed for the representation of individuals belonging to different socioeconomic statuses. However, limitations of the study include non-uniformity in the number of patients recruited from different centres and the study cohort not being representative of the geographic population, which restricts the generalisation of the study findings. The potential bias due to researchers’ discretion in gathering reasons for the delay in referral through the recall method cannot be excluded. Providing sufficient training on data collection could have minimised this bias.
Conclusion
According to the study findings, <30% accessed speciality care after 6 months. The primary reasons for delays in referring patients with SLE to rheumatology are initial referrals to other specialities and a lack of knowledge about rheumatology, underscoring the critical importance of timely specialist care. The study also highlights the need for enhanced education among primary care providers about rheumatological conditions, especially SLE, and the importance of early specialist referral.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors thank Debashish Dhanda and Aman Sharma for their participation in administrative roles in the IRA database. The authors also acknowledge the help of Research Assist (
Author Contributions
All the authors have contributed equally to the conceptualisation, data capturing and development of the content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the institutional committees of all participating centres.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received educational and research grants from Novartis India.
Patient Consent
Written informed consent was obtained from all the selected patients prior to the study, as per the respective institutional recommendation.