
Abstract
Objectives:
The aim of this study was to evaluate the correlation between nailfold capillaroscopic (NFC) findings and cardiac involvement in systemic sclerosis (SSc) using tissue Doppler echocardiography.
Patients and Methods:
Clinical, laboratory, NFC and echocardiographic examination were done for 30 SSc patients.
Results:
There was statistically significant difference between the three scleroderma pattern groups in terms of LV EF (left ventricle ejection fraction), PW (pulsed wave), Mit DT (mitral deceleration time), TAPSE (tricuspid annular plane systolic excursion), Mit A (Peak late transmitral filling velocity), Mit E/A, Tr E/A (ratio of early and late transmitral and transtricuspid filling velocities) and sPAP (systolic pulmonary artery pressure) when assessed using conventional echocardiography. There was a statistically significant difference between the three groups in terms of Em (early diastolic wave), Sm (myocardial systolic wave), Em/Am (late diastolic wave) and ET (ejection time) when assessed using tissue Doppler echocardiography. There was a significant strong correlation between capillary density and Em and moderate correlation between capillary density and Sm, Em/Am, Et, St (systolic time) and Et/At (acceleration time). There was a moderate correlation between avascular areas and Em/Am and St and between capillary neoangiogenesis and Sm, Em/Am, Et/At.
Conclusion:
Systolic and diastolic dysfunction were more common in late scleroderma pattern patients. Lower capillary density increased avascular areas and capillary neoangiogenesis were associated with cardiac dysfunction in SSc patients.
Keywords
Introduction
Systemic sclerosis (SSc) is an autoimmune disease associated with inflammation, endothelial dysfunction and fibrosis which leads to organ damage. 1 The incidence of CV (cardiovascular) disease is variable in literature (15%-30%), depending on its definition. CV diseases in SSc dramatically affect the prognosis and represent an important cause of mortality in SSc. 2 The main cardiac manifestations in SSc include pericarditis, rhythm abnormalities, conduction problems and myocardial dysfunction. 3 Additionally, cardiac problems in SSc can emerge as a complication of interstitial lung disease, renal involvement and pulmonary arterial hypertension (PAH). 4
Nailfold videocapillaroscopy (NVC) is a noninvasive diagnostic modality that allows the recognition of local microvascular changes in SSc. 5 Nailfold capillaroscopy (NFC) reflects the characteristic systemic vascular abnormalities, frequently before the appearance of systemic manifestations. 6 NFC has been developed as a marker for SSc progression. 7 Multiple studies showed that microvascular abnormalities may have correlation with internal organ involvement, especially the cardiopulmonary system. 8
Transthoracic Doppler echocardiography in addition to clinical assessment has been recommended for routine evaluation of the heart in SSc. But data showed that these modalities may be not helpful for diagnosis of cardiac affection in the preclinical stage in which treatment may be more effective. 9 More accurate evaluation of regional and global left ventricular (LV) and right ventricular (RV) function can be done by tissue Doppler echocardiography (TDE). 10 TDE measures contraction and relaxation velocities directly from the myocardium by assessing the myocardial structure velocity instead of blood flow. 11 Studying myocardial velocities by tissue Doppler is more accurate than conventional Doppler echocardiography as it allows localisation and identification of the extent of systolic and diastolic dysfunction. 12
The aim of this study is to evaluate the correlation between NFC findings and cardiac involvement using TDE in SSc patients.
Patients and Methods
Study Population
This is a cross-sectional, observational study which was conducted on 30 SSc patients during the period of October 2021 to October 2023. Patients were diagnosed according to the 2013 American College of Rheumatology/European League Against Rheumatism classification criteria for SSc. 13 Exclusion criteria included age <18 years, overlap syndrome, coronary artery or atherosclerotic heart disease, cardiomyopathy, atrial fibrillation, more than moderate valvular heart disease, dyslipidaemia, diabetes mellitus, hypertension, smoking, pregnancy and chronic kidney disease. Furthermore, patients who were incapable of having NFC examination, such as patients with very thick nailfold, injury or gangrene in more than four fingers were excluded.
Detailed history taking and clinical examination were performed to all patients. Evaluation of skin thickening was done using the modified Rodnan Skin Score (mRSS). The degree of skin thickening was graded in each region from 0 to 3 (0 = normal, 1 = mild thickening, 2 = moderate thickening and 3 = extreme thickening) with a maximum possible score of 51. 14 Laboratory investigations were performed including (complete blood picture, blood glucose, urine analysis, erythrocyte sedimentation rate (ESR), serum creatinine, serum bilirubin, alanine transaminase (ALT), rheumatoid factor, antinuclear antibody, anti Scl-70 antibody and anticentromere antibody). Chest X-ray, noncontrast computed tomography (CT) chest, electrocardiogram (ECG), NFC examination and echocardiographic examination were done for all patients.
Nailfold Capillaroscopic Examination
NFC was done by a rheumatologist experienced in NFC using Dino-Lite Capillaroscopy Pro (MEDL4N Pro) ×200 magnification. The resolution was improved by using immersion oil applied on the nailfold. All fingers of both hands were studied with exclusion of both thumbs and fingers with thick or ulcerated nailfolds. 15 The images were analysed using the software Dino Capture version 1.5.47.B. To ensure interobserver repeatability, the stored pictures were reviewed by the researcher in two separate periods.
The evaluated NFC parameters included capillary density, distribution, length, diameter, shape, microhaemorrhages, avascular areas and subpapillary venous plexus. Capillary density means the number of capillaries in a linear millimetre. Avascular area means that the distance between two capillaries is more than 500 µm and was evaluated as present or absent. Capillary distribution was evaluated as normal or abnormal. Capillary length was evaluated as normal or elongated (≥ 300 µm). Capillaries were considered dilated when there is increase in capillary diameter of 20 µm or more and giant capillaries were defined as a capillary with a homogeneously enlarged loop with a diameter of 50 µm or more. 16
Capillary shape was evaluated as normal hairpin, slight change including tortuosity and abnormal capillaries including meandering, ectasia and neoangiogenesis. Microhaemorrhages mean the presence of one or more dark red areas caused by hemosiderin deposits due to injury or thrombosis of the capillaries. Patients were classified according to the presence of subpapillary venous plexus into either absent or present. 17 The sum of successive images for each finger was used for mean capillaroscopic feature calculation. Then, all fingers’ values were added together and divided by the number of examined fingers. 18
The whole findings were classified as normal, nonspecific changes or specific changes as early, active and late scleroderma pattern. When there are infrequent giant capillaries, capillary microhaemorrhage and preserved capillary architecture with no significant capillary loss, the patient is defined as having early scleroderma pattern. Active scleroderma pattern was considered when there are large number of giant capillaries and capillary haemorrhages, moderate loss of capillaries, mild disturbed capillary architecture and absent or few ramified capillaries. Irregular widening of the capillaries, few or absent giant capillaries and haemorrhages, significant loss of capillaries with extensive avascular areas, disturbed capillary architecture and frequent capillary neoangiogenesis were defined as late scleroderma pattern. 19
Echocardiographic Examination
All echocardiographic studies were performed by the same physician who is experienced in echocardiography, using ultrasound machine TOSHIBA Xario (SSA-660A) (Japan). Patients were offered 20-minute rest before examination. The examination was done by the predefined protocol which includes a number of observations and measurements made according to the American Society of Echocardiography recommendations. 20 To ensure interobserver repeatability, the stored pictures were reviewed by the researcher in two separate periods.
M-Mode and Two-dimensional Echocardiography Measuring
LV cavity dimensions and wall thickness including End-diastolic diameter, end-systolic diameter and thickness of septum and posterior wall were evaluated. LV ejection fraction (EF) was estimated by the method of Simpson (LVEF <55% was considered abnormal). Diameter of left atrium calculated in the parasternal view and diameters of right ventricle (RV) and right atrium (RA) were evaluated. Pulmonary arterial pressure (PAP) was estimated from the transtricuspid pressure gradient, as evaluated by continuous wave Doppler, after the addition of an estimated 10 mm Hg right atrial pressure (systolic PAP >40 mm Hg was defined as abnormal). Patients with high pulmonary artery systolic pressure (>40 mm Hg) were not included in this study. 21 The tricuspid annular plane systolic excursion (TAPSE) (defined as the difference in the displacement of the RV base from end-diastole to end-systole) was attained from the apical four chamber view. TAPSE <16 mm denotes RV dysfunction. 22
Conventional Doppler Echocardiography
The transmitral and transtricuspid diastolic flow tracings were estimated from the apical four-chamber view by using pulsed Doppler echocardiography with the sample volume located at the tips of the mitral and tricuspid leaflets. Peak early transmitral (Mit E) and early transtricuspid (Tr E) filling velocity, peak late transmitral (Mit A), and late transtricuspid (Tr A) filling velocity and their ratio (Mit E/A, Tr E/A, respectively) and Deceleration time of peak early transmitral velocity (Mit DT) were recorded. 23
Tissue Doppler Imaging
Pulsed wave tissue Doppler myocardial motion velocities were assessed in the apical four-chamber view from the lateral mitral annular sites and the tricuspid annulus at the RV wall. Pulsed TDE was characterised by a myocardial systolic wave (Sm, St) and two diastolic waves (early diastolic (Em, Et) and late diastolic (Am, At). Several cardiac cycles were assessed, and the best three successive ones were analysed and averaged. 21 Isovolumic contraction time (IVCT), isovolumic relaxation time (IVRT) and ejection time (ET) derived by TDE were also taken. Those time intervals were required for the estimation of the myocardial performance index (MPI) which provides an index of global RV and LV function. Em/Am and Et/At of both mitral and tricuspid valve were calculated as an index of LV and RV filling pressure, respectively. 24
Statistical Method
Data analysis was done using the Statistical Package of Social Sciences (SPSS) for Windows (SPSS version 25). Numbers and percentages were used for the description of qualitative data. The presentation of continuous variables was in the form of mean ± SD (standard deviation) for parametric data and median (min-max) for nonparametric data. Normality of distribution of continuous variables was tested using Shapiro–Wilk test. The significance of differences between two groups was determined using T test for variables with normal distribution and Mann–Whitney U test for variables with non-normal distribution. For the detection of difference between more than 2 groups, one-way analysis of variance (ANOVA) was used for normally distributed variables and Kruskal–Wallis test was used for non-normally distributed variables. The correlation between continuous variables was done using Pearson’s or Spearman correlation. Statistical significance was defined as P value < .05 in this study.
Results
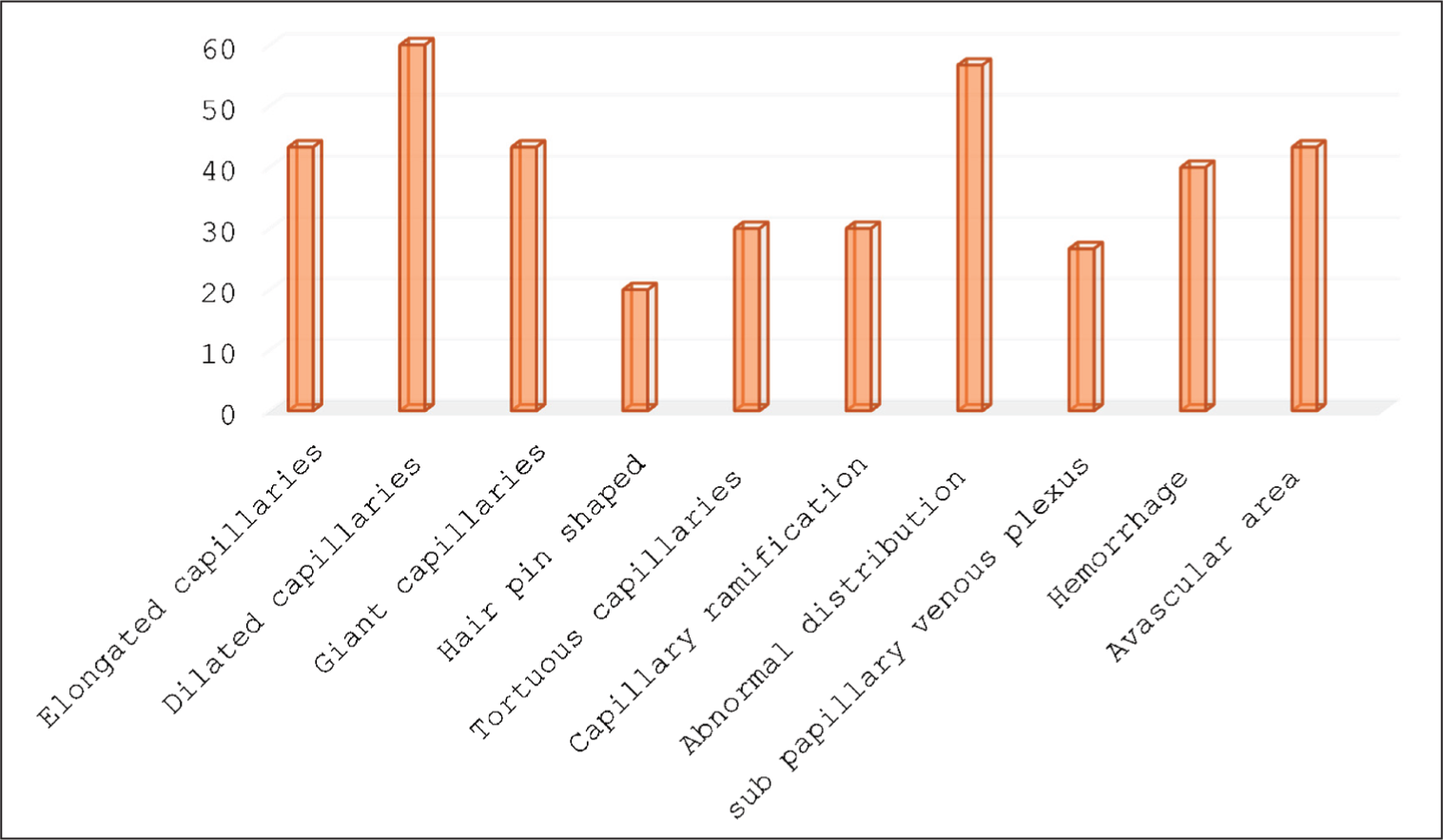
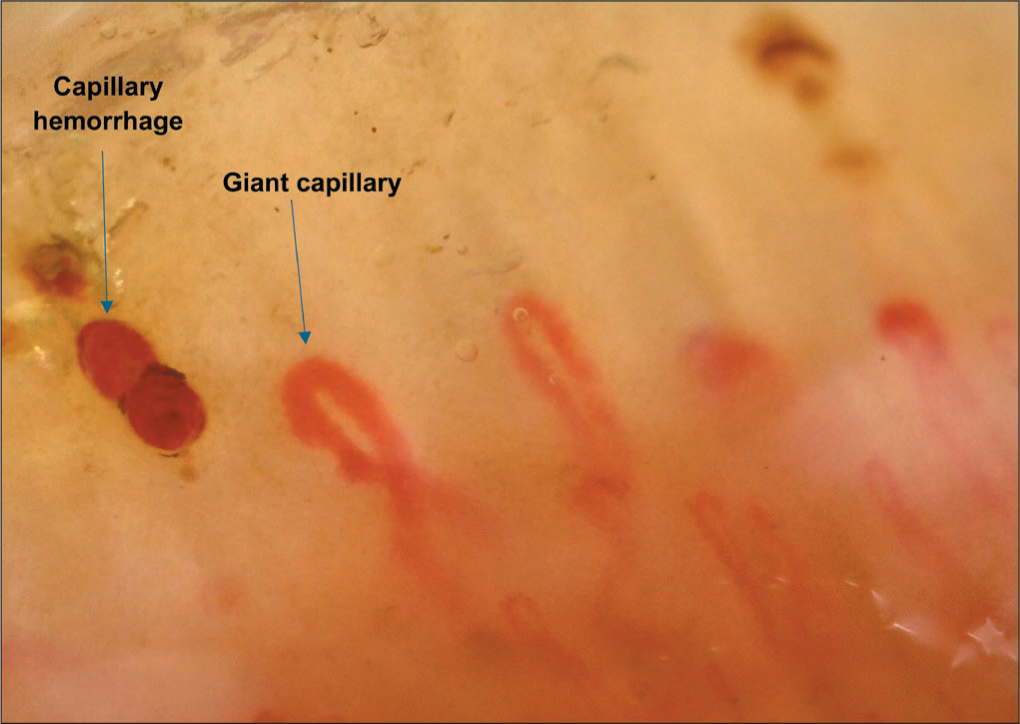
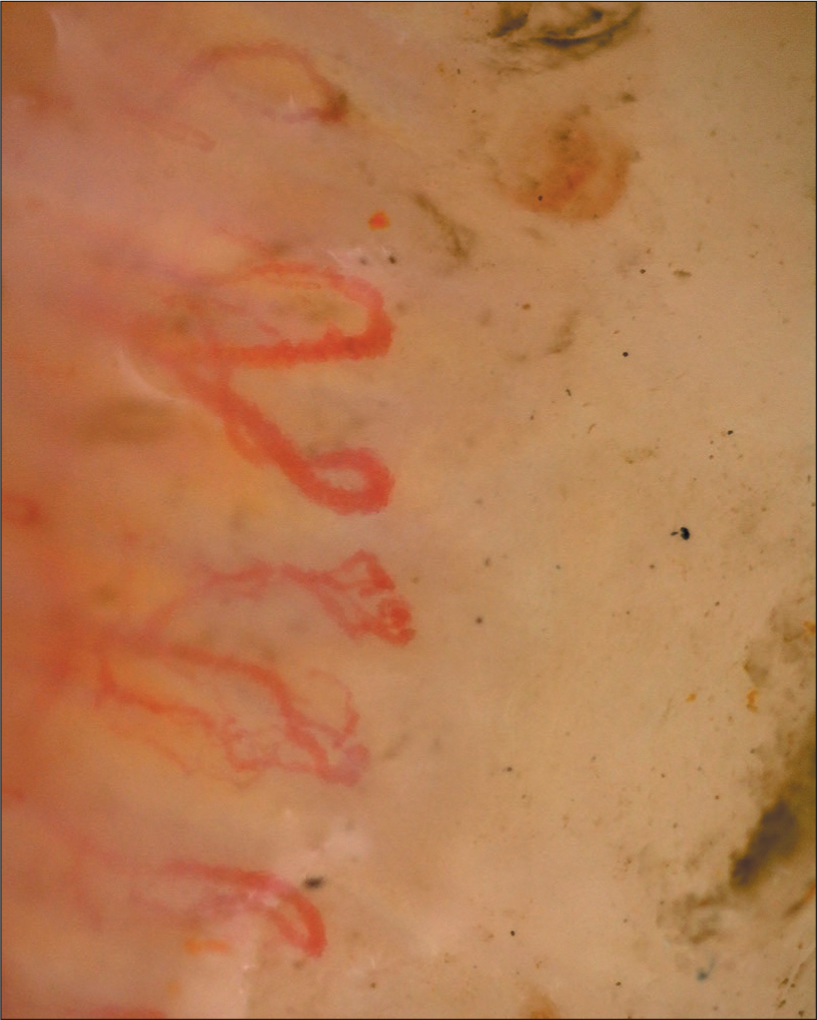
Capillaroscopic findings of the studied patients are summarised in Figure 1. Patients were classified according to NFC into three scleroderma patterns. Early scleroderma pattern was found in 10 patients (33.3%) as in Figure 2, active scleroderma pattern was found in 12 patients (40%) as in Figure 3 and late scleroderma pattern was found in 8 patients (26.7%) as in Figure 4. There was a significant difference between SSc patients with different scleroderma patterns as regard body weight (P = .028), body mass index (BMI; P = .046), mRSS (P = .008), presence of pitting scars (P = .013), digital ulcers (P = .01), dysphagia (P = .026), dyspnoea (P = .04) and palpitation (P = .006) as demonstrated in Table 1.
Nailfold Capillaroscopy Findings in Studied Cases.
Nailfold Capillaroscopy Showing Dilated Tortuous Capillaries, Giant Capillary, Capillary Density 7 Capillaries/mm (Early Scleroderma Pattern).

Nailfold Capillaroscopy Showing Giant Capillaries, Capillary Haemorrhage and Loss of Capillaries (Active Scleroderma Pattern).
Nailfold Capillaroscopy Showing Capillary Neoangiogenesis with Loss of Capillaries and Disorganisation of Capillary (Late Scleroderma Pattern).
Difference in Clinical and Laboratory Data Between Scleroderma Patients with Different Capillaroscopic Scleroderma Patterns.
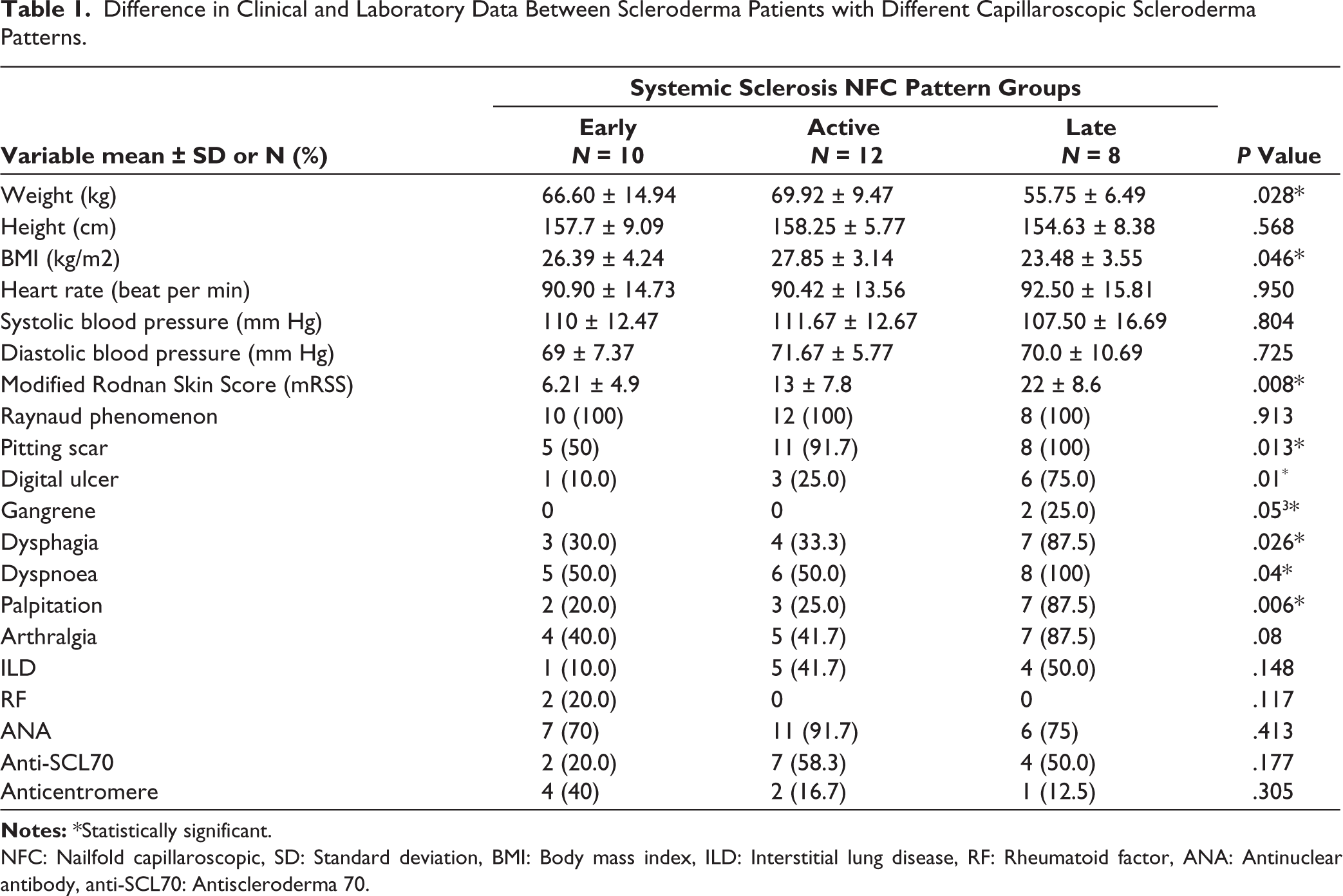
NFC: Nailfold capillaroscopic, SD: Standard deviation, BMI: Body mass index, ILD: Interstitial lung disease, RF: Rheumatoid factor, ANA: Antinuclear antibody, anti-SCL70: Antiscleroderma 70.
Regarding conventional echocardiography, there was statistically significant difference between SSc patients with early, active and late scleroderma patterns regarding LV EF (P = .035), PW (P = .001), Mit DT (P = .001), TAPSE (P = .007), Mit A (P = .001), Mit E/A (P = .001), Tr E/A (P = .006) and sPAP (P = .036) as demonstrated in Table 2. As regard TDE, there was a statistically significant difference between patients with different capillaroscopic scleroderma patterns regarding Em (P = .001), Sm (P = .02), Em/Am (P < .001) and Et (P = .005) as shown in Table 3.
Difference in Conventional Echocardiography Between Systemic Sclerosis Patients with Different Capillaroscopic Scleroderma Patterns.
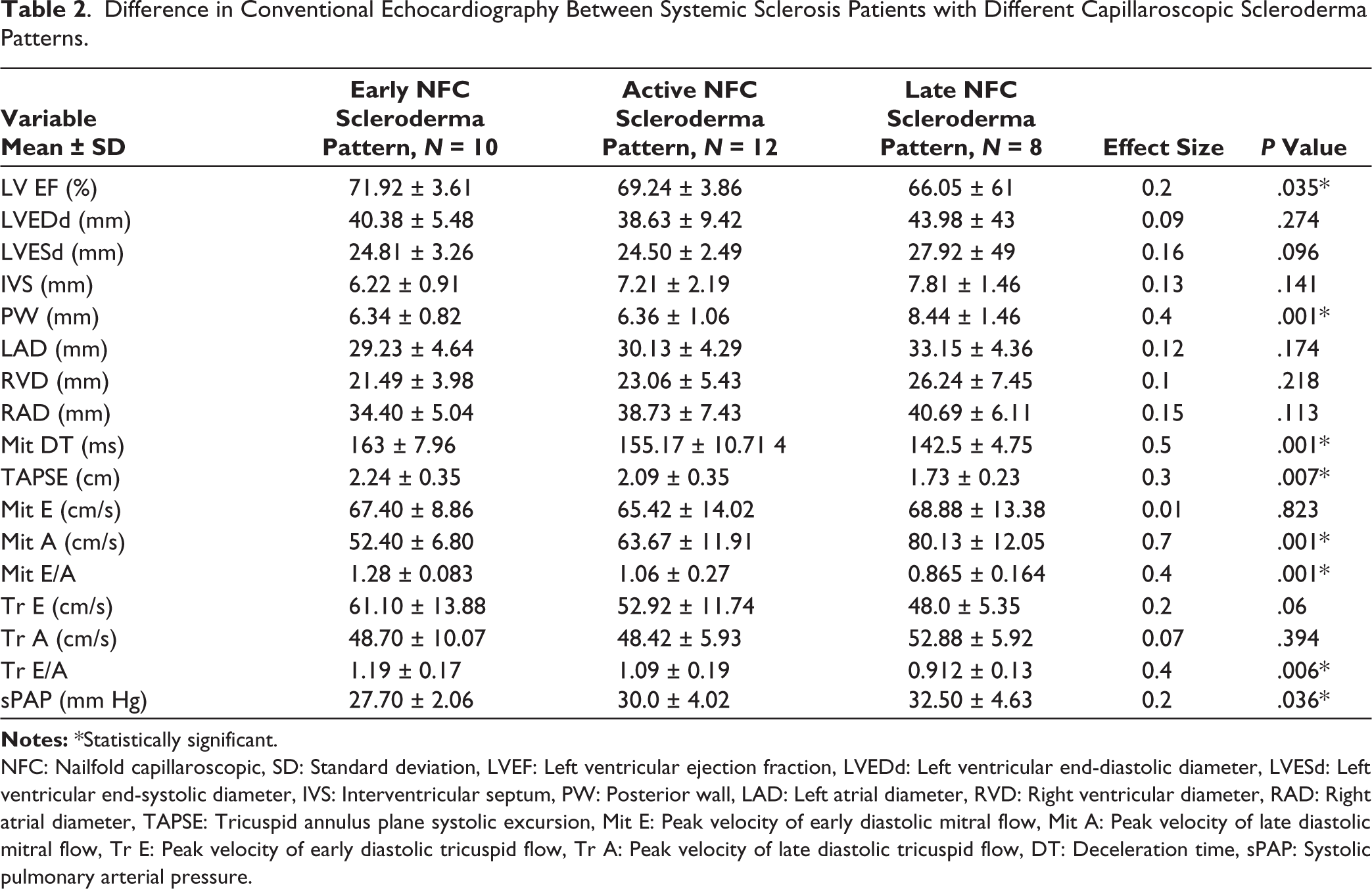
NFC: Nailfold capillaroscopic, SD: Standard deviation, LVEF: Left ventricular ejection fraction, LVEDd: Left ventricular end-diastolic diameter, LVESd: Left ventricular end-systolic diameter, IVS: Interventricular septum, PW: Posterior wall, LAD: Left atrial diameter, RVD: Right ventricular diameter, RAD: Right atrial diameter, TAPSE: Tricuspid annulus plane systolic excursion, Mit E: Peak velocity of early diastolic mitral flow, Mit A: Peak velocity of late diastolic mitral flow, Tr E: Peak velocity of early diastolic tricuspid flow, Tr A: Peak velocity of late diastolic tricuspid flow, DT: Deceleration time, sPAP: Systolic pulmonary arterial pressure.
Difference in Tissue Doppler Echocardiography Between Systemic Sclerosis Patients with Different Capillaroscopic Scleroderma Patterns.
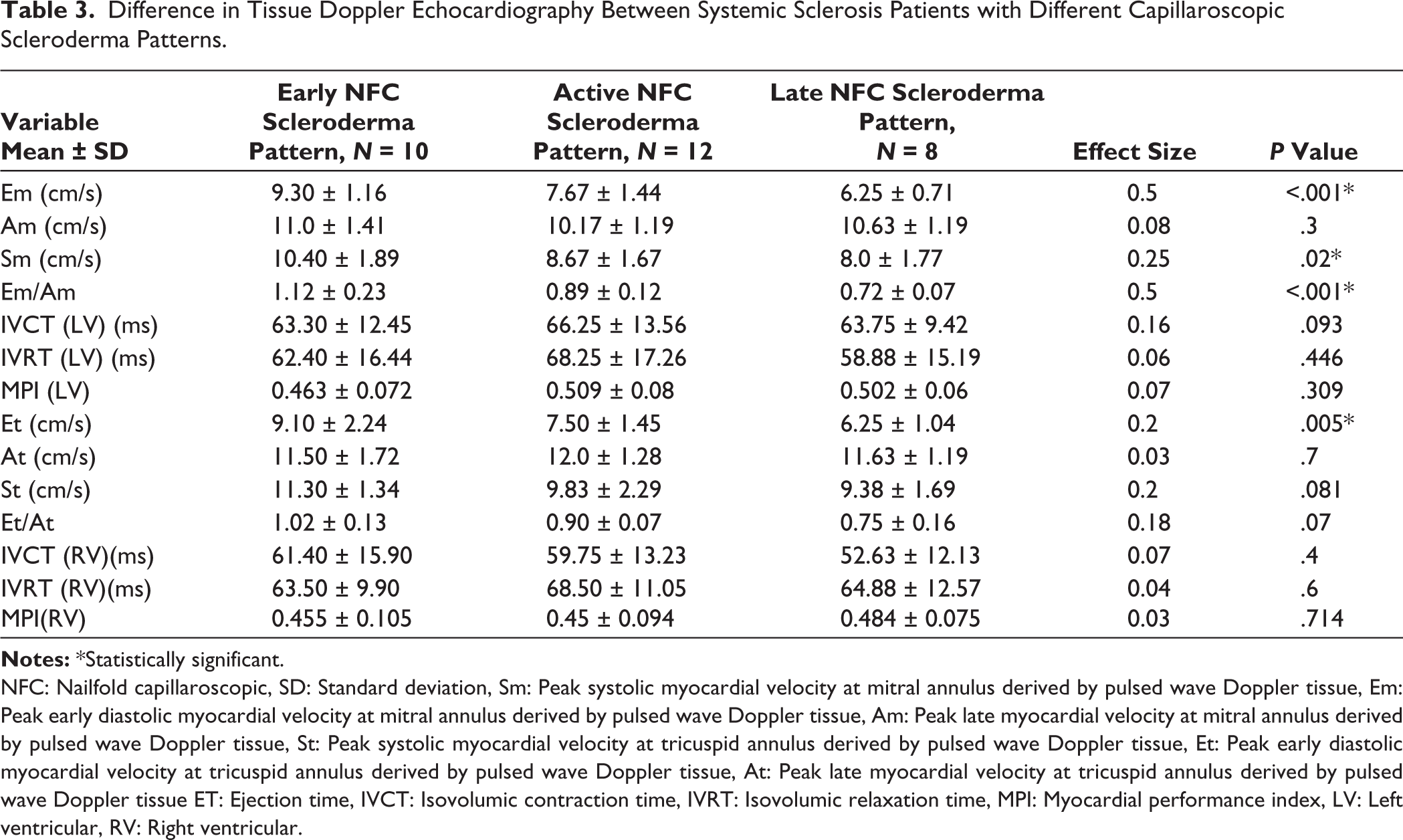
NFC: Nailfold capillaroscopic, SD: Standard deviation, Sm: Peak systolic myocardial velocity at mitral annulus derived by pulsed wave Doppler tissue, Em: Peak early diastolic myocardial velocity at mitral annulus derived by pulsed wave Doppler tissue, Am: Peak late myocardial velocity at mitral annulus derived by pulsed wave Doppler tissue, St: Peak systolic myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, Et: Peak early diastolic myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, At: Peak late myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue ET: Ejection time, IVCT: Isovolumic contraction time, IVRT: Isovolumic relaxation time, MPI: Myocardial performance index, LV: Left ventricular, RV: Right ventricular.
There was statistically significant correlation between capillary density and Em (R = 0.77, P = .001), Sm (R = 0.51, P = .004), Em/Am (R = 0.62, P = .001), Et (R = 0.48, P = .007), St (R = 0.37, P = .04) and Et/At (P = .39, P = .04). There was statistically significant correlation between avascular areas and Em/Am (R = −0.68, R < 0.001) and St (R = −0.43, P = .02). There was statistically significant correlation between capillary neoangiogenesis and Sm (R = −0.43, P = .02), Em/Am (R = −0.44, P = .02), Et/At (R = −0.49, P = .006) as shown in Table 4. After doing regression analysis, avascular areas were found to be the main predictor for Em/Am (B = −0.6, P = .04) and capillary density was the main predictor for Et/At (B = −0.4, P = .03) as shown in Table 5.
Correlation Between Nailfold Capillaroscopy Findings and Tissue Doppler Echocardiography Among Studied Cases.
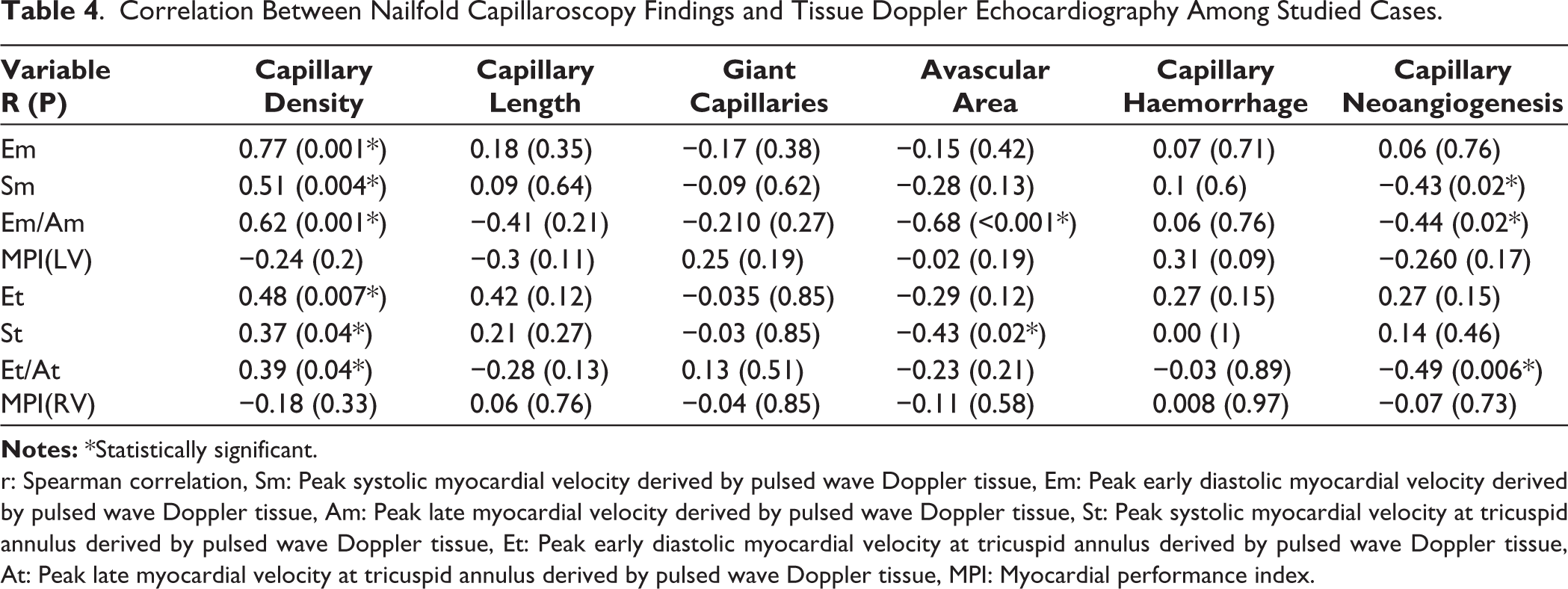
r: Spearman correlation, Sm: Peak systolic myocardial velocity derived by pulsed wave Doppler tissue, Em: Peak early diastolic myocardial velocity derived by pulsed wave Doppler tissue, Am: Peak late myocardial velocity derived by pulsed wave Doppler tissue, St: Peak systolic myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, Et: Peak early diastolic myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, At: Peak late myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, MPI: Myocardial performance index
Linear Regression Analysis for Nailfold Capillaroscopic Predictors for Diastolic Dysfunction by Tissue Doppler Echocardiography in the Studied Patients.
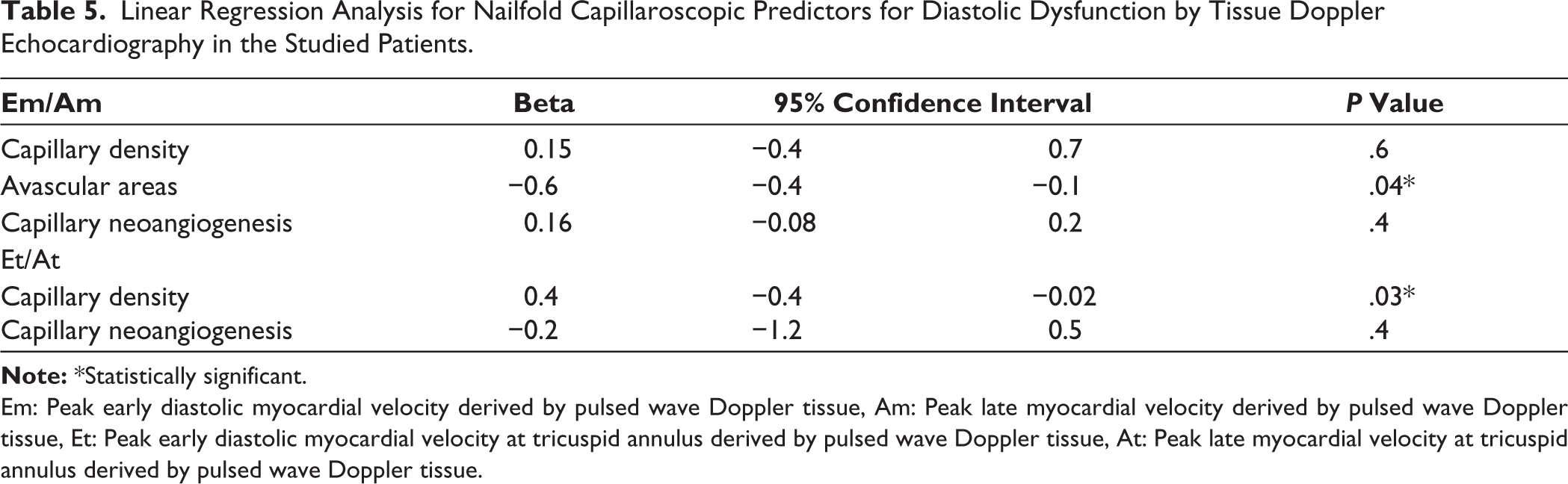
Em: Peak early diastolic myocardial velocity derived by pulsed wave Doppler tissue, Am: Peak late myocardial velocity derived by pulsed wave Doppler tissue, Et: Peak early diastolic myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue, At: Peak late myocardial velocity at tricuspid annulus derived by pulsed wave Doppler tissue.
Discussion
SSc is a chronic autoimmune disease characterised by immune dysfunction, vasculopathy and progressive fibrosis. 25 Cardiac involvement is associated with higher risk of mortality. Thus, early detection and follow-up of CV involvement are very important in the management of SSc. 26
In this study, most patients (40%) had an active NFC scleroderma pattern followed by an early pattern (33.3%); however, late NFC scleroderma pattern was detected in only 26.7% of patients. Similarly, active scleroderma pattern was the most frequent pattern in other studies.6,27,28 Similar to this study, Caramaschi et al. reported that late pattern was the least frequent pattern 27 ; however, early scleroderma pattern was the least frequent pattern in other studies.6,28,29 Patients with gangrene, thickening or ulceration affecting more than four fingers were excluded from the study and this may lead to decreased number of patients with late scleroderma pattern.
Body weight and BMI were significantly lower in patients with late scleroderma pattern than patients with early and active scleroderma patterns. These findings were compatible with a study done by Yalcinkaya et al. on a 134 SSc patients where they found that SSc patients with medium-to-high risk for malnutrition had more frequent late scleroderma pattern than those with low risk for malnutrition. Also, low capillary density (≤ 6/mm) was shown to have independent association with medium-to-high risk for malnutrition. 30
Digital ulcer, pitting scar, gangrene, dysphagia, dyspnoea and palpitation were significantly more common in patients with late scleroderma pattern than patients with early and active scleroderma patterns. Similarly, other studies reported a significant association between future significant organ involvement and nailfold capillaroscopy pattern, with higher correlation for late pattern and lower for early pattern.31,7 Also, Sulli et al. found a significant correlation between the progression of NFC pattern and organ involvement in SSc patients after 12 years follow-up. 32 Additionally, another study reported a positive correlation between active and late scleroderma patterns and cardiopulmonary involvement. This association suggests a common pathogenic mechanism leading to microvascular affection at different levels. 33 In the same line with these results, Duarte et al. found a significant association between late scleroderma pattern and higher number of digital ulcers and more oesophageal involvement. 34
To evaluate whether the peripheral microvasculature is a mirror for similar pattern of cardiac vasculopathy, reflected by systolic and diastolic dysfunction, NFC pattern was correlated with the echocardiographic characteristics in this study. There was a statistically significant difference between all the three groups regarding LV EF, Mit DT, TAPSE, Mit A, Mit E/A, Tr E/A and sPAP denoting significant difference in RV and LV function. The relationship between nailfold capillaroscopy pattern and LV and RV function was also evaluated using Doppler tissue imaging and found that there was significantly worse LV systolic and diastolic function in patients with late scleroderma pattern compared to active and early scleroderma pattern groups. In addition, impaired RV function was more common in patients with late scleroderma pattern. The results of this study are in line with Caramaschi et al. study which reported progressive increase in cardiac involvement with progression of capillaroscopic scleroderma patterns from early to late. 27
Similarly, in a cohort study performed on 40 patients with SSc, there was a significant correlation between different grades of NFC and CV events during follow-up. More frequent grade 4 NFC and less frequent grade 2 NFC were found in patients with CV events. NFC pattern more than grade 2 was significantly higher in the CV event group. These results indicate that NFC has an important clinical value in CV risk stratification of SSc patients. According to these findings, impaired local microvasculature of fingers is probably associated with global microvascular impairment reaching peripheral arterial circulation leading to peripheral arterial ulcers, coronary microcirculation leading to systolic and diastolic dysfunction and pulmonary circulation leading to precapillary pulmonary hypertension (PH). 35
Several TDE-derived parameters were correlated with capillaroscopic characters and clinical features in another study. Multiple regression analysis of baseline data revealed that Em/Am < 1 was associated with age, New York Heart Association (NYHA) functional class II and late capillaroscopic pattern which seemed to be in line with the findings in this study. 36 Additionally, Markusse et al. have reported the predictive role of NFC and specific autoantibodies in cardiopulmonary involvement. Specifically, higher pro-BNP (brain natriuretic peptide) and increased systolic dysfunction were more in patients with active and late scleroderma patterns. 37
Limited number of previous studies had evaluated the association between NFC findings and systolic and diastolic function parameters on echocardiography. This study correlated quantitative NFC finding with parameters of cardiac function including Em, Sm, Em/Am, LV MPI, Et, St, Et/At and RV MPI. It was found that capillary density, avascular areas and capillaries with neoangiogenesis were the most common NVC findings to be correlated with cardiac function parameters. Several studies are in line with the results of this study which reported that the development of a more active and destructive microangiopathy in the form of progressive capillary loss has been independently recognised as an indicator of poor prognosis and organ progression. 32,33,38
Cardiac function (LV and RV both systolic and diastolic) was inversely correlated with avascular area score and number of capillaries with neoangiogenesis in this study. In agreement with this study, Vos et al. found that eʹ lateral velocity and E/eʹ ratios were negatively correlated with nailfold capillary density (NCD). On cardiac magnetic resonance imaging (MRI), both the indexed LV mass and the LA reservoir strain were negatively correlated with NCD. In addition, pro-BNP levels were negatively correlated with NCD. However, no correlations were found with LV systolic function or RV volumes and function. 39
Also, Zanatta et al. found that coronary flow reserve was inversely correlated with NFC-avascular score. Avascular and capillary ramifications scores were significantly higher in patients with coronary microvascular dysfunction than in those without. This may explain worse systolic and diastolic function with increasing avascular score. 40
Additionally, sequential quantitative NFC revealed that progressive capillary loss from baseline was predictive for disease progression, digital ulcer, lung vascular progression defined as new onset of precapillary pulmonary hypertension on right heart catheterisation, skin fibrosis and Medsger severity score worsening. 33 This may support the results of this study that destructive lesions on nailfold capillaroscopy reflect systemic affection and both share similar mechanisms. This study correlated nailfold capillaroscopic changes to cardiac affection using conventional and TDE. Capillary density and presence of avascular areas were the main predictors for systolic and diastolic dysfunction in SSc patients.
This study has some limitations—this is a single-centre study with a rather small number of patients, which may limit the power of statistical analysis. However, patients are referred from multiple areas for evaluation in Mansoura University hospital as it is a tertiary centre. Also, NFC is an operator-dependent method; however, all patients were examined by one operator who was blinded to other clinical and echocardiographic parameters.
Conclusion
Systolic and diastolic dysfunction were more common in patients with late scleroderma pattern. Low capillary density increased avascular areas and a higher number of capillary neoangiogenesis were correlated with impaired cardiac function in patients with SSc. NFC is a simple inexpensive procedure which can be used as a screening tool for prediction of cardiac affection and severity of disease in patients with SSc. Presence of avascular areas or decreased capillary density are predictors of cardiac dysfunction in SSc patients and thus echocardiographic evaluation is strongly recommended in these patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Mansoura University (IRB code number: MD.21.10.546).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Explanation of the study was provided to all the participants, and an informed consent was taken.