
Abstract
Background:
Poor medication adherence challenges efficacy and costs in achieving treatment goals for rheumatoid arthritis (RA). This study aimed to determine the prevalence of treatment adherence and its related factors in Iranian RA patients.
Methods:
This cross-sectional study included RA outpatients referred to the rheumatology clinic of Shariati Hospital between March 2017 and September 2018, with the diagnosis based on the American College of Rheumatology (2010 ACR/EULAR) criteria. Treatment adherence was evaluated using the standardized Persian version of the 8-item Morisky Medication Adherence Scale (MMAS-8). Demographic and clinical information was extracted through the Iranian RA registry system (RHEUMATRY-RA).
Results:
Of 275 participants (222(81%) female), 20(7%) patients had active RA. Medication adherence was low in 138(50%) of patients, moderate in 81(30%) and high in 56(20%). In patients with disease duration ≤ 10 years, medication adherence was significantly associated with sex and occupation. It was observed that older patients (adjusted odds ratio (aOR) (95% confidence interval (CI): 1.01(0.98, 1.03)) and women (aOR (95% CI): 1.64(0.60, 4.45)) had more adherence. Patients on glucocorticoids demonstrated higher (aOR (95% CI): 1.76(0.81, 3.84)) and on methotrexate lower (aOR (95% CI): 0.58(0.18, 1.86)) adherence. The odds of disease activity were 21% lower in people who had adhered to medication (aOR (95% CI): 0.79(0.29, 2.15)).
Conclusion:
Despite the inherent complexity of adherence behaviors, this study identified a high prevalence of poor medication adherence among RA patients. Patients with better adherence may have lower disease activity, underscoring its role in effective disease management.
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disorder characterised by persistent inflammation affecting joints and extra-articular organs. 1 Joint inflammation in RA resulting from immune cell infiltration and excess proinflammatory cytokines can lead to cartilage and bone damage.2,3 Despite significant advancements, the precise cause of RA remains unclear. 4 However, recent evidence has suggested that genetic, epigenetic and environmental factors contribute to RA etiology.5,6 Recent discoveries in genetics and disease mechanisms, in addition to new advancements in disease assessment and therapeutic tools, have resulted in the introduction of various novel treatments 7 (such as targeted biologic and synthetic disease-modifying antirheumatic drugs (DMARDs)), which have improved outcomes. 8 Besides, in-time diagnosis and personalised approaches with thorough monitoring and management can enhance the likelihood of remission in RA patients. 9
One other significant challenge in achieving the treatment goal is the need for more adherence in chronic disorders like RA. Adherence is the process of patients following their medication prescriptions, encompassing drug initiation, regimen implementation and discontinuation. 10 Noncompliance leads to insufficient treatment response, treatment failure, disease exacerbation or relapse, as well as unwarranted alterations in treatment. It has been observed that adherence tends to diminish as time progresses.11,12 Patients’ optimistic expectations regarding disease outcomes before starting conventional synthetic DMARD treatment independently predict adherence. Patients’ beliefs about their disease and medication significantly predict early non-adherence, indicating that interventions addressing patient concerns and increasing awareness may enhance adherence. Furthermore, having two or more co-morbidities, 13 medication costs, regimen complexity or patient forgetfulness also can have effects on adherence rates. 14 Despite the various potential factors influencing adherence to RA treatment, the factors associated with adherence among RA patients exhibit inconsistency across studies that emphasise the requirement for further research. 15
Adherence has not been extensively studied in rheumatic conditions, and currently, there is a need for a gold standard to measure adherence. However, several approaches can help to evaluate patients’ adherence to treatments. Patient questionnaires like the Compliance Questionnaire in Rheumatology (CQR) offer a simple and cost-effective means to assess adherence and identify factors affecting compliance in RA. 16 The Morisky Medication Adherence Scale (MMAS) in both its 4-item (MMAS-4) and 8-item (MMAS-8) versions is also commonly used as a self-administered questionnaire. Additionally, the medication possession ratio (MPR) calculation offers a more objective means of adherence evaluation. However, no consensus has been reached on the optimal approach for evaluating treatment adherence in RA. 17 Also, past studies have yielded varying findings about factors affecting adherence. There is evidence indicating certain factors are linked to either low or high drug adherence among individuals. However, detecting patients at a high risk of non-adherence is still challenging. 18 Identifying any additional factors or obstacles that might be causing noncompliance is essential, and exploring strategies that could improve adherence and ultimately lead to better results. Therefore, this study aimed to estimate the prevalence of medication adherence and its associated factors among RA patients in the Tehran rheumatology clinic. This study advances the literature by utilising the validated Persian MMAS-8 scale and integrating registry-based data for a more robust analysis of adherence factors. Moreover, it aimed to investigate the relationship between adherence and disease activity. The primary objective of this study was to evaluate the distribution of treatment adherence among patients with RA from a referral centre in Iran, utilising data from the RHEUMATRY-RA registry. Given the correlation between disease duration and treatment duration, the secondary objective was to examine the association between demographic and clinical characteristics and medication adherence in two subgroups of patients (RA duration ≤10 years and >10 years), separately. Finally, medication adherence and its associated factors were assessed using both crude and adjusted analyses.
Materials and Methods
Study Design
This observational cross-sectional study considered consecutive outpatients referred to the rheumatology clinic at Shariati Hospital (a tertiary referral centre), affiliated with Tehran University of Medical Sciences, between 16 March 2017 and 18 September 2018. The patients’ diagnoses were confirmed based on the American College of Rheumatology (2010 ACR/EULAR) criteria. 19 The inclusion criteria were age ≥18 years, confirmed diagnosis of RA by a rheumatologist and absence of cancer or other infectious diseases (as patients with these conditions often receive complex and diverse treatments). Exclusion criteria included refusal to participate or any uncertainty regarding the fulfilment of diagnostic criteria for RA. Patients in drug-free remission, those with a single visit who accessed the questionnaire but did not complete all items, were excluded from the analysis. Additionally, patients without data on RA disease activity were excluded from subsequent analyses.
Sample Size Calculation
According to the study by Gadallah et al. (2015), the prevalence of adherence to treatment in patients with RA was estimated at P = 9%.20,21 Using the following formula, with a 95% confidence level (Z = 1.96), a margin of error of d = 3.5%, and considering about 5% attrition rate, the final sample size was determined to be 275.
Data Collection
After obtaining informed consent from all patients, data were collected using a comprehensive checklist of demographics (age, gender, ethnicity, education level, occupation, marital status, physical activity, etc.) and clinical variables (treatment strategy, disease activity, etc.). All of this information was extracted from the Iranian Registry of Rheumatoid Arthritis (RHEUMATRY-RA), which is the first nationwide and multicentre, web-base RA registry and is supported by the Ministry of Health and Medical Education in Iran.
Self-reported medication adherence was measured using the standardized Persian version of the MMAS-8 in RA patients.20,21 This questionnaire is an extension of the MMAS-4 to assess medication adherence. MMAS-8, with its 0-8 scale, can provide more detailed insights into patient behaviour than MMAS-4’s responses. Its versatility and straightforward questions make it a preferred tool for assessing adherence across various diseases and populations. 22 The MMAS-8 consists of seven dichotomous questions (Yes = 0, No = 1 point) and one five-point Likert-type question (Never = 0, Rarely = 1, Sometimes = 2, Often = 3, Always = 4). One question (item 5) is reverse-scored. There are three categories of adherent patients: high adherence patients with a score of 8 on the scale, medium adherers with a score of 6 to < 8 and low adherers with a score of <6. A score of 6 or higher (the first two groups) was considered good medication adherence. The questionnaire is in a supplementary file. Illness duration was calculated by subtracting the disease diagnosis date from the date of study onset. Prednisolone was labelled as a glucocorticoid. Methotrexate, leflunomide, hydroxychloroquine and sulphasalazine were categorised as conventional synthetic DMARDs. Mycophenolate mofetil, as an immune suppressive drug, cyclophosphamide, azathioprine, etc., were considered other treatments. Disease activity of RA was evaluated by disease activity score using 28 joints (DAS28-ESR = (0.56 * sqr(Tender joint count (TJC))) + (0.28 * sqr(Swollen joint count (SJC))) + (0.7 * ln(ESR)) + (0.014 * Global health (GH))) which was classified in this study as follows: DAS28-ESR <2.6, remission; DAS28-ESR ≥2.6, active. Participants reported the days they performed ≥20 minutes of physical activity per week, coded as none or moderate to high (2-7 days).
The primary outcome of this study was treatment adherence, categorised as low, moderate and high, among patients with RA. The association between demographic and clinical characteristics and medication adherence was then analysed in two subgroups based on disease duration (RA ≤10 years and >10 years). Finally, patients were classified into two groups—adherent and non-adherent—and the relationship between demographic and clinical characteristics and adherence was further investigated.
Statistical Analysis
Quantitative and qualitative variables were presented as mean ± standard deviation (SD) and frequencies (%), respectively. The normality of quantitative data was assessed using the Kolmogorov–Smirnov test. Nonparametric tests, including the chi-squared test (with the Monte Carlo method applied in cases of sparse data) and the Kruskal–Wallis test, were used to compare variable distributions across the low, moderate and high treatment adherence groups. Given the correlation between disease duration and treatment duration, all comparisons were conducted separately for two subgroups of patients (RA duration ≤10 years and >10 years).
Finally, by merging the moderate and high adherence groups, good medication adherence was defined, and univariate and multiple logistic regression models were applied to estimate crude and adjusted odds ratios (aORs) along with their corresponding 95% confidence intervals (CIs). In the univariate analysis, each variable was individually included in the model. Based on clinical experience and significant associations observed in the univariate analysis, age, sex, occupation and disease duration were selected as adjusted variables in the multiple logistic regression model.
All statistical analyses were performed using IBM SPSS Statistics version 27, with a significance level of 5% applied to all tests.
Ethical Considerations
This study was designed under the Declaration of Helsinki and was approved by the Medical Ethics Committee of Tehran University of Medical Sciences (Code: IR.TUMS.VCR.REC.1399.510). Patients were enrolled in the study after informed consent, with anonymity ensured by excluding their names. In the dataset, each individual was identified with a unique code, and their names were removed. In compliance with medical ethics regulations, patient data were protected and not disclosed to unauthorised personnel.
Results
Patient’s Characteristics and Prevalence of Medication Adherence
Out of 275 patients analysed, 222 (81%) patients were women. The participants’ mean age and disease duration were 53.18 ± 11.95 years and 13.26 ± 10.00 years, respectively. The majority of patients were married (225 (82%)) and of Turkish ethnicity (120 (44%)). Most had a nonacademic education level (165 (60%)). Only 62 (23%) participants engaged in moderate-to-high physical activity levels. Additionally, the disease activity status of 255 (93%) patients was inactive. The treatment of 38 (14%) subjects was only with glucocorticoids, and 237 (86%) patients were on DMARDs at the time of completing the questionnaire (Table 1).
Demographic and Clinical Characteristics of the Study Population by Medication Adherence and Disease Duration.
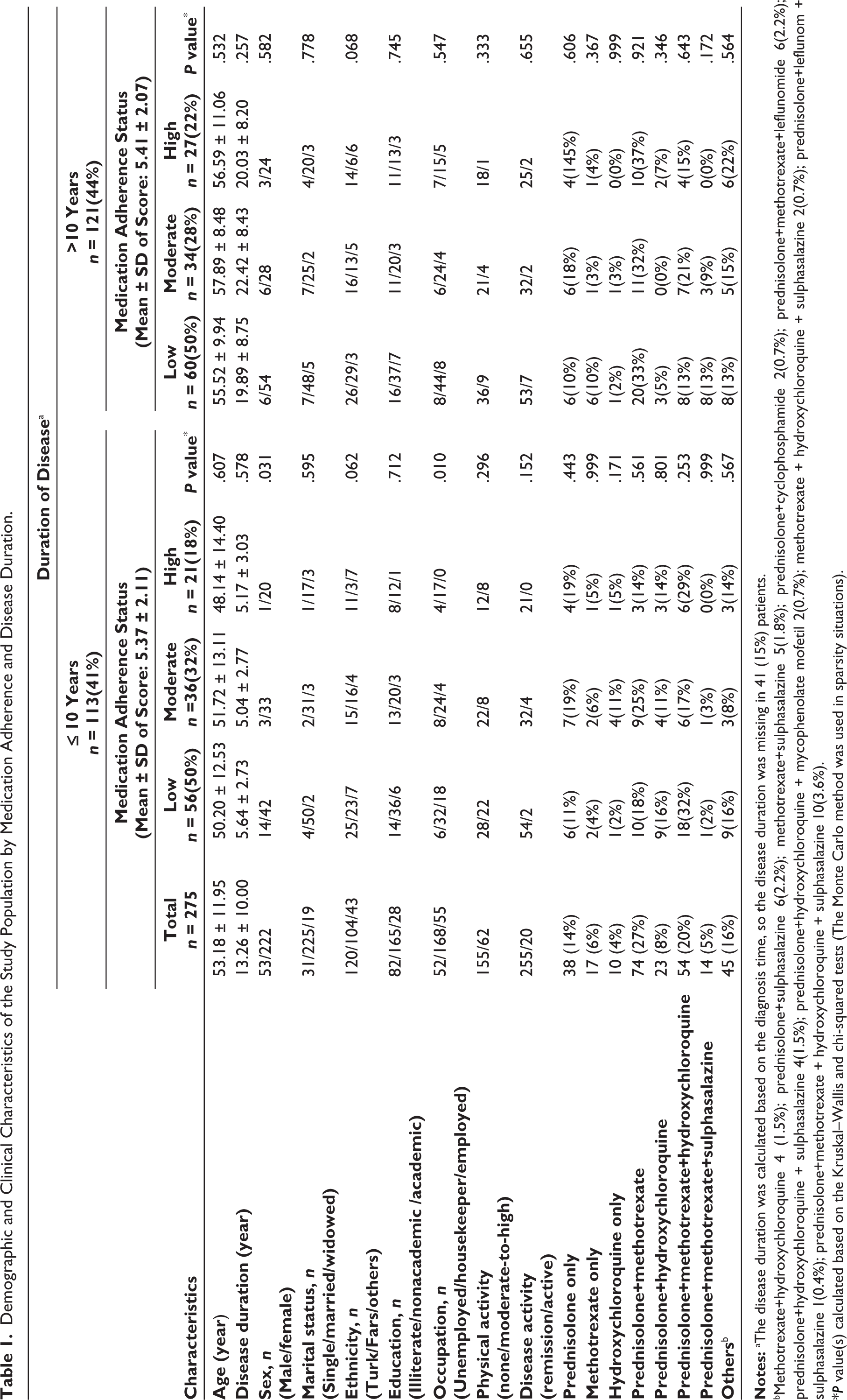
bMethotrexate+hydroxychloroquine 4 (1.5%); prednisolone+sulphasalazine 6(2.2%); methotrexate+sulphasalazine 5(1.8%); prednisolone+cyclophosphamide 2(0.7%); prednisolone+methotrexate+leflunomide 6(2.2%); prednisolone+hydroxychloroquine + sulphasalazine 4(1.5%); prednisolone+hydroxychloroquine + mycophenolate mofetil 2(0.7%); methotrexate + hydroxychloroquine + sulphasalazine 2(0.7%); prednisolone+leflunom + sulphasalazine 1(0.4%); prednisolone+methotrexate + hydroxychloroquine + sulphasalazine 10(3.6%).
*P value(s) calculated based on the Kruskal–Wallis and chi-squared tests (The Monte Carlo method was used in sparsity situations).
According to the MMAS-8, 138 participants (50%) exhibited low adherence, 81 participants (30%) showed moderate adherence and 56 participants (20%) exhibited high adherence to treatment. Additionally, 127 (46%) of patients sometimes forget to take their drugs, 95 (34%) of study sample miss taking their medicine for response other than forgetting over two past weeks, 92 (33%) of patients reduced or discontinued their medication without consulting their physician, 79 (29%) of patients sometimes forget to bring along their drugs during travel or leave home, 246 (89%) of patients said a positive response to this question ‘Did you take all your drugs yesterday?’, 69 (25%) of subjects stopped taking their medicine when they felt their symptoms were under control. Furthermore, 92 (33%) patients reported feeling burdened by adhering to their treatment regimen. (Results not shown).
Since disease duration would be correlated with the treatment duration, the study population was divided into two groups as follows: 113 patients with RA ≤ 10 years and 121 patients with RA > 10 years. In patients with disease duration ≤ 10 years, the medication adherence was significantly associated with sex and occupation. The complete results are summarised in Table 1.
Factors Associated with Medication Adherence
The prevalence of medication adherence was estimated to be 50%. Table 2 shows the results of comparing demographic and clinical characteristics between medication-adherent and nonadherent groups. The mean age and disease duration were lower in participants with nonadherence (52.25 ± 11.6 years and 13.01 ± 9.70 years, respectively). This study’s univariate and multiple logistic regression results showed no statistically significant relationship between patient characteristics and medication adherence, except for the job status (aOR (95% CI): 0.31 (0.12, 0.81); P = .017) and number of drug used (aOR (95% CI): 0.69 (0.50, 0.97); P = .031) when adjusted by sex, age and disease duration. Consequently, employed patients demonstrated approximately 70% lower adherence to treatment compared to their unemployed counterparts. Additionally, reducing the number of medications by one resulted in a 30% increase in medication adherence.
Medication Adherence and Their Associated Factors Among Iranian Patients with Rheumatoid Arthritis.
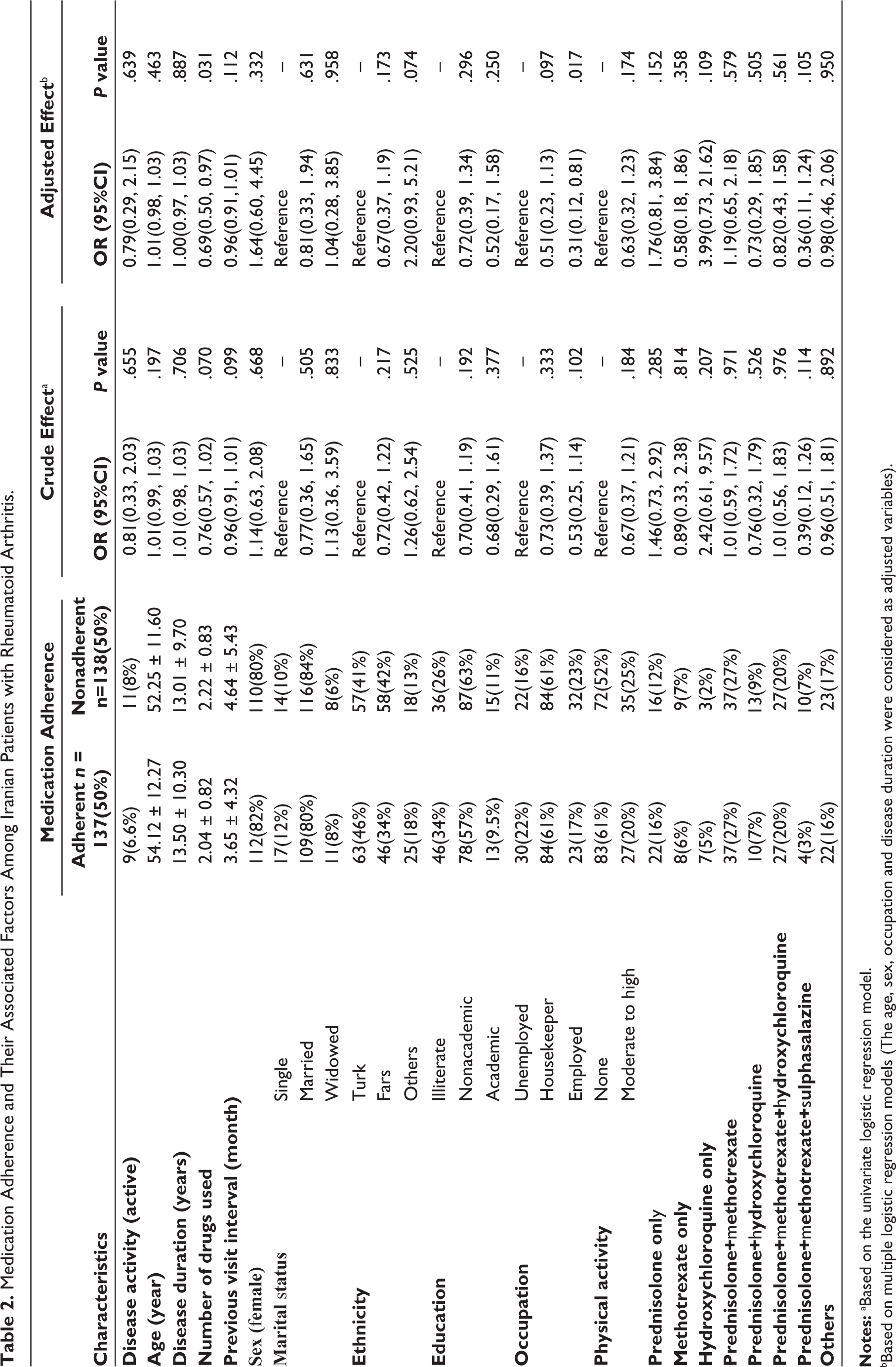
Notes: aBased on the univariate logistic regression model.
bBased on multiple logistic regression models (The age, sex, occupation and disease duration were considered as adjusted variables).
By adjusting the effect of other variables using multiple logistic regression models, it was observed that older people (aOR (95% CI): 1.01 (0.98, 1.03); P = .463) and women (aOR (95% CI): 1.64 (0.60, 4.45); P = .332) had more adherence to treatment (1% higher than young and 64% more than men respectively). Patients on only prednisolone (aOR (95% CI): 1.76 (0.81, 3.84); P = .152), only hydroxychloroquine (aOR (95% CI): 3.99 (0.73, 21.62); P = .109) and both prednisolone and methotrexate (aOR (95% CI): 1.19(0.65, 2.18); P = .579), demonstrated higher, and on other drugs especially among patients that use only methotrexate (aOR (95% CI): 0.58 (0.18, 1.86); P = .358) were lower adherence. The odds of disease activity were 21% lower in people who had adhered to medication (aOR (95% CI): 0.79 (0.29, 2.15); P = .639), but these differences were not statistically significant (P > .05).
Discussion
This study evaluated medication adherence and associated factors among 275 patients with RA, revealing notable information regarding adherence and influencing variables. The study subjects were predominantly female and middle-aged, with suboptimal adherence. Common barriers to adherence included forgetfulness, self-adjustment of dosages and treatment burden. Notably, employment status and polypharmacy had a significant association with low adherence. Although results suggested higher adherence among older adults and women, as well as variations by drug regimen, these associations were not statistically significant. Similarly, disease activity and sociodemographic factors, except occupation, were not independently related to adherence. These findings underscore the complex nature of adherence, where other healthcare-related factors may play a greater role than demographic or clinical characteristics. Moreover, they highlight the need for considering practical barriers such as polypharmacy and occupational demands to optimise treatment outcomes in RA management.
Patients’ Overall Adherence in Rheumatoid Arthritis
The overall low adherence in RA patients in this study aligns with previous studies. Gadallah et al. conducted a study to evaluate treatment adherence rates in RA patients utilising the 8-item Morisky scale. Their findings indicated that 90.6% of participants exhibited low adherence, while 9.4% were moderately adherent, with no highly adherent individuals. 23 In the other study on 207 RA patients, 66.7% of participants were nonadherent to medication. 15 A cohort comprising 859 patients in a study by Pombo-Suarez et al. demonstrated an adherence rate of 79%. 24
Demographic Status
In this study, in the ≤10 years disease duration group, patients were generally younger compared to those with a longer disease duration, though age differences across medication adherence levels were not significant. However, in the study by Gadallah et al. demographic factors such as younger age (P = .002) and increased levels of general satisfaction (P = .02) were associated with improved adherence. 23 In the other study, the adherence rates in RA patients, age, sex, marital status, education level and smoking did not significantly affect adherence. 25 In this study, females were more prevalent in both groups, with a notable gender difference in the early disease stage, suggesting possible gender-related variations in disease presentation or diagnosis. However, gender differences were not significant in the longer disease duration group across different adherence levels. Additionally, there are variations in medication adherence among different marital statuses. Although these differences did not reach statistical significance, they suggest the potential influence of family support before marriage on drug adherence. In another study by Marras et al. it was indicated that male gender and younger age have an independent correlation with a higher risk of non-adherence. One in five RA patients, as identified by the CQR, were detected at a risk for non-adherence, being more prevalent among younger individuals and males. 26 In a study on RA, various factors like age, income, comorbidities, functional status as measured by the Health Assessment Questionnaire (HAQ) and treatment regimens showed significant links to medication noncompliance. Yet, in a further analysis, only age and HAQ remained negatively associated with noncompliance. 27 Other studies have also presented different findings regarding factors associated with noncompliance. Xia et al. indicated that individuals’ income were significant contributors to noncompliance. 28 Zhang et al. on the other hand, observed that adverse drug effects and the utilisation of alternative therapies were inversely linked to adherence. 29 These findings highlight the complexity of factors influencing medication adherence and underscore the need for tailored interventions to address individual patient needs and challenges in adhering to treatment regimens.
Patients’ Occupation
After adjusting for other variables, employed patients exhibited lower motivation for medication adherence. Similarly, Ghosh et al. in a survey study showed that employed patients had lower motivation on the Modified Morisky adherence scale. 30 Zhang et al. also observed that employment status and having a job with light-to-moderate physical demands were inversely linked to adherence. 29 On the other hand, studies by SharMa and Bharthi found no link between job status and adherence,31,32 which may be due to differences in the scales used for job status and adherence.
Number of Medications
Our study found that the number of prescribed medications was linked to adherence in RA patients. Nonadherent patients used slightly more drugs (2.22 ± 0.83 vs. 2.04 ± 0.82), and after adjustment, this association was statistically significant (P = .031), which was aligned with a study by Pombo-suarez et al. that demonstrated the number of drugs was an independent predictor of adherence. 24 Xia et al. also found that individuals’ total number of DMARDs were significant contributors to noncompliance. 28 This finding highlights the role of adherence in RA, since RA treatment strategies often rely on the combined use of steroids, conventional DMARDs (cDMARDs), and biologic DMARDs (bDMARDs).
Differences Between Medications
Based on the aORs in this cohort, hydroxychloroquine monotherapy had the highest likelihood of adherence (nearly fourfold compared to others), followed by prednisolone monotherapy, while prednisolone+methotrexate and combination therapy showed intermediate adherence levels. Other combination therapies generally showed intermediate-to-low adherence levels. Methotrexate monotherapy or in combination with multiple drugs appeared to be associated with lower adherence, with the prednisolone-methotrexate-sulphasalazine combination showing the lowest adherence tendency. Although the adjusted analysis of medication adherence across different treatment regimens revealed no statistically significant associations between specific therapies and adherence status, it may reflect underlying differences in tolerability, dosing convenience and patient perceptions. Adherence to medications is significantly influenced by the patient’s beliefs and perceptions about their medications. 33 For instance, the observed disparity in adherence between hydroxychloroquine and methotrexate monotherapy may be due to the more favourable side effect profile, daily dosing and minimal monitoring requirements of hydroxychloroquine, which may seem as a well-tolerated option for patients. In contrast, frequent gastrointestinal toxicity, weekly dosing (which is prone to errors) and the need for regular blood tests of methotrexate make it often perceived as a high-risk medication.33,34 These factors may contribute to higher discontinuation rates and lower adherence compared to hydroxychloroquine. The reason for low-to-moderate adherence ratios for combination therapies is possibly due to the complexities of adhering to a multidrug regimen, cumulative side effects or dosing burdens, though this association warrants further investigation.
A descriptive study by BART et al. also showed that, considering the assessment tool employed, 68%–60% of patients have adherence to DMARDs. 25 In Pombo-Suarez et al.’s study, there were no differences in adherence among patients receiving bDMARDs versus those receiving cDMARDs or those receiving intravenous therapies compared to alternative routes of administration. Additionally, no differences in adherence were noted between individuals treated in specific day hospitals versus polyvalent day hospitals. 24
Disease Activity
In this study, no statistically significant association was observed between disease activity and medication adherence. However, patients with adherence showed a slightly lower disease activity. This lack of association may be attributed to the high proportion of patients in remission, with only 20 individuals exhibiting active disease. Moreover, like other factors, there are some conflicting variables regarding the correlation between drug adherence and disease activity. 15
In a Meta-analysis by Li et al. on 1963 adult RA patients, they found substantial heterogeneity across studies reporting disease activity and adherence. The analysis showed that the DAS-28 score, erythrocyte sedimentation rate and tender joint count were significantly lower in adherent compared to nonadherent patients. 35 In line with these findings, Nakagawa et al. observed that among patients with a disease duration of less than 4.6 years, DAS28-ESR and the risk of disease flare in patients with the highest adherence were significantly lower than in those with the lowest adherence. 36 However, the relationship between adherence and disease activity may appear inconsistent across different populations. For instance, a study in North Africa found no association between RA activity and adherence to biologic drugs. 37 On the contrary, Owen et al. in a comprehensive observational study conducted in the United Kingdom involving 178 RA patients reported that individuals exhibiting higher disease activity tend to adhere to their treatment regimens more than those with lower disease activity. 38 The heterogeneity in the literature regarding this association may arise from differences in measurement tools, varying cutoffs (e.g., ≥80% adherence), study populations, medication regimens and the multifactorial nature of adherence itself. Conducting longitudinal studies, standardising adherence assessment tools and controlling confounders in the future could help better understand the role of adherence in the severity of disease activity of RA.
Barriers to Adherence
In this study, nearly half of the participants reported occasional forgetfulness regarding medication intake, particularly during travel or being away from home. Furthermore, a notable proportion of patients (33%) reported self-adjusting or discontinuing their medication without consulting a healthcare provider, suggesting potential gaps in patient-provider communication and shared decision-making processes. Moreover, a substantial subset of patients (33%) feeling burdened by their treatment regimen indicates a need for simplified schedules, patient education, support to improve adherence and consideration of patient preferences in treatment planning. In previous studies, critical barriers to adherence included concerns about side effects, cost of medications and psychological factors, such as the belief that medication is only necessary during acute episodes. Additionally, lifestyle factors, including demanding schedules that lead to neglecting healthcare or prioritising other responsibilities, can further compromise adherence. These studies also noted that better adherence correlated with positive medication beliefs, greater healthcare satisfaction and reduced disease activity.23,39 In another study by Marras et al. patients with beliefs in low medication efficacy exhibited an elevated likelihood of non-adherence (P = .012). 26 In the study by BEMT et al. nonadherence did not correlate with demographic or clinical factors, satisfaction with information, concerns about drugs or coping strategies. This suggests variability across populations and underscores the complex nature of adherence and needs further evaluations. 25
This study contains various strengths and limitations. Its representative sample of 275 RA patients and the utilisation of the standardised Persian version of the 8-item Morisky Medication Adherence Questionnaire, which enhances consistency in measuring adherence levels, are significant strengths. The comprehensive data collection covering demographic information, medical history and medication adherence also allows for a thorough understanding of adherence behaviours. Clinical confirmation conducted by rheumatology specialists enhances the validity of the findings. However, limitations like the cross-sectional design, limiting causal inference and potential self-reporting bias in medication adherence data may affect validity. The study’s single-centre setting may limit generalisability. Some findings that do not reach statistical significance warrant cautious interpretation. While the study provides valuable insights into medication adherence among RA patients, these limitations should be considered when interpreting the results.
In conclusion, this study of 275 participants reveals significant insights into medication adherence among RA patients. With 50% of participants exhibiting low adherence, the findings indicate a pressing need for interventions to improve compliance. Notably, adherence was significantly associated with demographic factors, such as sex and occupation, particularly in patients with a disease duration of 10 years or less. Older individuals and women showed higher adherence rates, while those on glucocorticoids demonstrated better adherence compared to those on methotrexate. Importantly, the study found that adherence to medication was linked to a 21% reduction in disease activity, highlighting the critical role of medication compliance in managing RA effectively. These results underscore the necessity for targeted strategies to enhance adherence, ultimately improving treatment outcomes for RA patients.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Data Availability
All data generated or analysed during this study are available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was designed in accordance with the Declaration of Helsinki guidelines and was approved by the Medical Ethics Committee of Tehran University of Medical Sciences (Code: IR.TUMS.VCR.REC.1399.510). Patients were enrolled in the study after informed consent, with anonymity ensured by excluding their names. In compliance with medical ethics regulations, patient data were protected and not disclosed to unauthorised personnel.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The written informed consent was signed by all participants before enrolling in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.