
Abstract
Background:
Idiopathic scoliosis is a common spine problem in young adults. Although the incidence of ankylosing spondylitis (AS) is less than that of scoliosis, it usually begins in adolescence and can be seen with scoliosis.
Methods:
The study prospective is a cross-sectional study. Patients who applied to physical therapy and rheumatology outpatient clinic with the diagnosis of AS were included in the study as a patient group; people of similar age and gender to the patient group, who with non-inflammatory low back pain, were included in the study as a control group; and Cobb angle was calculated from thoracolumbar radiograph using a program installed on the system.
Results:
A total of 311 people, 161 patients with AS and 150 people as the control group, were included in the study. While scoliosis frequency was 24.2% in the AS group and 6% in the control group, scoliosis was more frequent in the AS group as statistically significant (P < .01). Uveitis (P = .015, odds ratio (OR) = 4.229), C-reactive protein (CRP; P = .037 OR = 1.245) and bilateral grade 4 sacroiliitis (P < .01, OR = 1.556) were found to be associated with presence of scoliosis in binary logistic regression analysis in AS group. There was no difference between the groups in age, gender, medications, axial and axial plus peripheric involvement, HLA-B27 positivity, erythrocyte sedimentation rate, presence of enthesopathy, duration of disease and Bath Ankylosing Spondylitis Disease Activity Index (P > .05), according to the presence of scoliosis, in AS group.
Conclusions:
Our study revealed that scoliosis was more common in AS with a frequency reaching 24.2% of AS cases compared to 6% in the control group, but the presence of scoliosis was not associated with other parameters in disease activity except CRP and uveitis frequency; and with any change except the degree of sacroiliitis.
Keywords
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease primarily involving the axial skeleton, causing structural damage and functional limitation. 1 Patients are mostly diagnosed in the young adult period. In approximately 80% of cases, symptoms begin before age 30. 2 The prevalence of AS is about 0.9% in world. 3 Tuncer et al. reported the frequency of AS as 0.46% in the general population in Turkey. 4
Modified New York criteria are used for diagnosing AS and Assessment in SpondyloArthritis International Society (ASAS) criteria for diagnosing spondyloarthropathy. Modified New York criteria consist of clinical and radiological criteria. Clinical criteria include low back pain lasting at least three months, which improves with exercise and does not decrease with rest, limitation of lumbar spine movement in sagittal and frontal planes, and decreased chest expansion compared to normal values for age and gender. Radiological criteria are bilateral stage 2, 3 or 4 sacroiliitis and unilateral stage 3 or 4 sacroiliitis. A clinical and a radiological criteria are required for definitive diagnosis of AS. 5 In 2010, the ASAS group created new classification criteria for axial and peripheral spondyloarthropathies. According to the ASAS criteria, axial spondyloarthritis can be diagnosed in patients under 45 years old who have had low back pain for at least three months, along with sacroiliitis detected on imaging and at least one clinical spondyloarthritis criterion, or HLA-B27 positivity along with at least two clinical spondyloarthritis criteria. 6
Studies on the spine in AS patients are pretty limited, and these studies have examined mainly spinal changes specific to AS. Hyperkyphosis is the most common postural abnormality seen in AS patients. 7 In the later stages of the disease, syndesmophytes and ankylosis of facet joints occur. Bamboo spine is a late finding. 8 The characteristic conventional radiographic changes of AS in vertebrae develop gradually throughout the disease and are best illustrated by lateral radiographs. 9
Scoliosis is defined as the curvature of vertebrae in the coronal plane and is typically accompanied by varying degrees of spine rotation. 10 While the worldwide prevalence of scoliosis is between 1 and 4%, the incidence of adolescent idiopathic scoliosis (AIS)in 16,045 students was found to be 2.3% (3.1% in women, 1.5% in men) in a study conducted in Turkey in 2020.11,12 Cobb method is considered gold standard measurement method for degree of curvature. Cobb angle must be ≥10 degrees for scoliosis to be diagnosed. Cobb angle curves <10 degrees are within the normal range of spinal asymmetry, and none have long-term clinical significance.
There is no data in the literature regarding the incidence of scoliosis in AS. Both scoliosis and AS are frequently encountered in adolescence. Vertebral damage, possibly secondary to AS, triggers the formation of scoliosis. Scoliosis can affect mechanical load and cause secondary changes in sacroiliac joints and the lumbar spine. We thought that scoliosis was more common in patients with AS than in normal population, and we aimed to determine frequency of scoliosis in patients diagnosed with AS and to raise awareness that scoliosis may affect prognosis of disease.
Methods
Study Design
This prospective cross-sectional study was undertaken between February 2022 and August 2022. All patients gave written and verbal informed consent. The Ethics Committee Presidency approved the study protocol before the study.
Patients
Patients who met Modified New York criteria were consecutively seen in physical medicine and rehabilitation and rheumatology outpatient clinics, which were included in the study. Patients who did not meet Modified New York criteria, who had mental cognitive disorders at a level where communication and cooperation could not be established, and who did not accept thoracolumbar radiography were excluded from the study. After completing the surveys of patients with AS, the gender and age distribution of the patient group was determined. Patients who applied to the city hospital physical medicine and rehabilitation and rheumatology outpatient clinic with non-inflammatory low back pain, similar age and gender, and who accepted thoracolumbar radiography and sacroiliac radiograph to exclude sacroiliitis were included in the study as the control group. We did not include patients aged 50 and over in the study, both in the scoliosis and control groups, because the prevalence of scoliosis increased with age and rule out degenerative scoliosis. We did not include patients with asymptomatic radiographic sacroiliitis in the AS group. Seventeen patients were excluded from the study because their diagnosis was uncertain, twenty-two patients were excluded from the study because they did not accept thoracolumbar radiography, and two patients were excluded because their cognitive status was not good.
The following information was recorded for all participants: personal details (age, gender, occupation and education), general health data (smoking and alcohol use, history of chronic diseases, and current medications), and if there is scoliosis-related findings on X-ray (Cobb angle, location and aspect of scoliosis).
Additionally, for patients in the AS group, specific disease-related data were collected, including biological drug use history, family history, active complaints, age of symptom onset, age at diagnosis, type and radiological involvement, HLA-B27 status (if available), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) levels, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) score and history of peripheral joint involvement. Both scoliosis and control patients were asked whether they had ever had a uveitis attack, and the electronic patient card was scanned to see if the patient had previously been diagnosed with uveitis by the ophthalmology outpatient clinic. No additional deformity measurements were made on the patients. Our hospital’s normal biochemistry laboratory values were accepted as 0-4 U/mL, 0-8 mg/L for CRP and 0 mm/hour - 20 mm/hour for ESR.
Outcome Measurements
BASDAI Score
The BASDAI score was used to assess disease activity. The higher the BASDAI score, the greater the patient’s disease activity and disability. In the case of BASDAI ≥4, disease status is considered active. The validity and reliability of the BASDAI index in Turkish society were established in 2005. 13
Cobb Angle
The Cobb method is accepted as a standard measurement method in determining the degree of curvature. Cobb angle was calculated from an anteroposterior thoracolumbar radiograph using a program installed on the PACS (Picture Archiving and Communication Systems) system. Scoliosis was classified as thoracic, thoracolumbar, lumbar with right- or left-facing, depending on its location in spine, and patients with a Cobb angle of more than 10 degrees were considered to have scoliosis.
Statistical Analysis
Power analysis was performed using G-power 3.1.9.4 version. All analyses were carried out with SPSS 26.0 (IBM, USA). Based on comparing age variables between the groups of patients with or without scoliosis in the study of Mochizuk et al. 14 by T-test, it was calculated that 80 patients should be included in each group with an effect size of 0.519, an alfa error of 0.05 and 80% power. Our ethics committee recommends enrolling at least as many patients as in the power analysis and does not object to enrolling more, so we enrolled 161 patients in the study. The findings of the study are expressed as frequency and percentages. Normality analysis was carried out using Kolmogorov–Smirnov test. The variables that did not normally distribute are presented as median and interquartile range (IQR) with 25-75th percentiles. Numeric dependent variables with abnormal distribution were compared with the Mann–Whitney U test. Categorical variables were compared using the chi-squared test. Possible correlations of variables with scoliosis were analysed with binary logistic regression. Multiple linear regression analysis was performed to determine possible relations between the Cobb angle and potential variables. P < .05 was accepted for statistical significance.
Results
A total of 311 people, 161 patients with AS and 150 people in the control group were included in the study. Demographic characteristics and some clinical and radiological findings of patients are shown in Table 1. The female/male ratio and mean age of both groups were similar, and there was no statistical difference. Vertebral fractures were not observed in the control group but were observed in 3(1.86%) patients in the AS group. While scoliosis frequency was 24.2% in the AS group and 6% in the control group, scoliosis was more frequent in the AS group as statistically significant (P < .01). Thoracolumbar and right-sloping scoliosis were observed in the patient and control groups. Meanwhile, the median Cobb angle was 14 (12-18) in the AS group and 11 (10-13) in the control group (Table 1).
Demographic Features and Clinical and Radiological Findings of the Patients and Control Group.
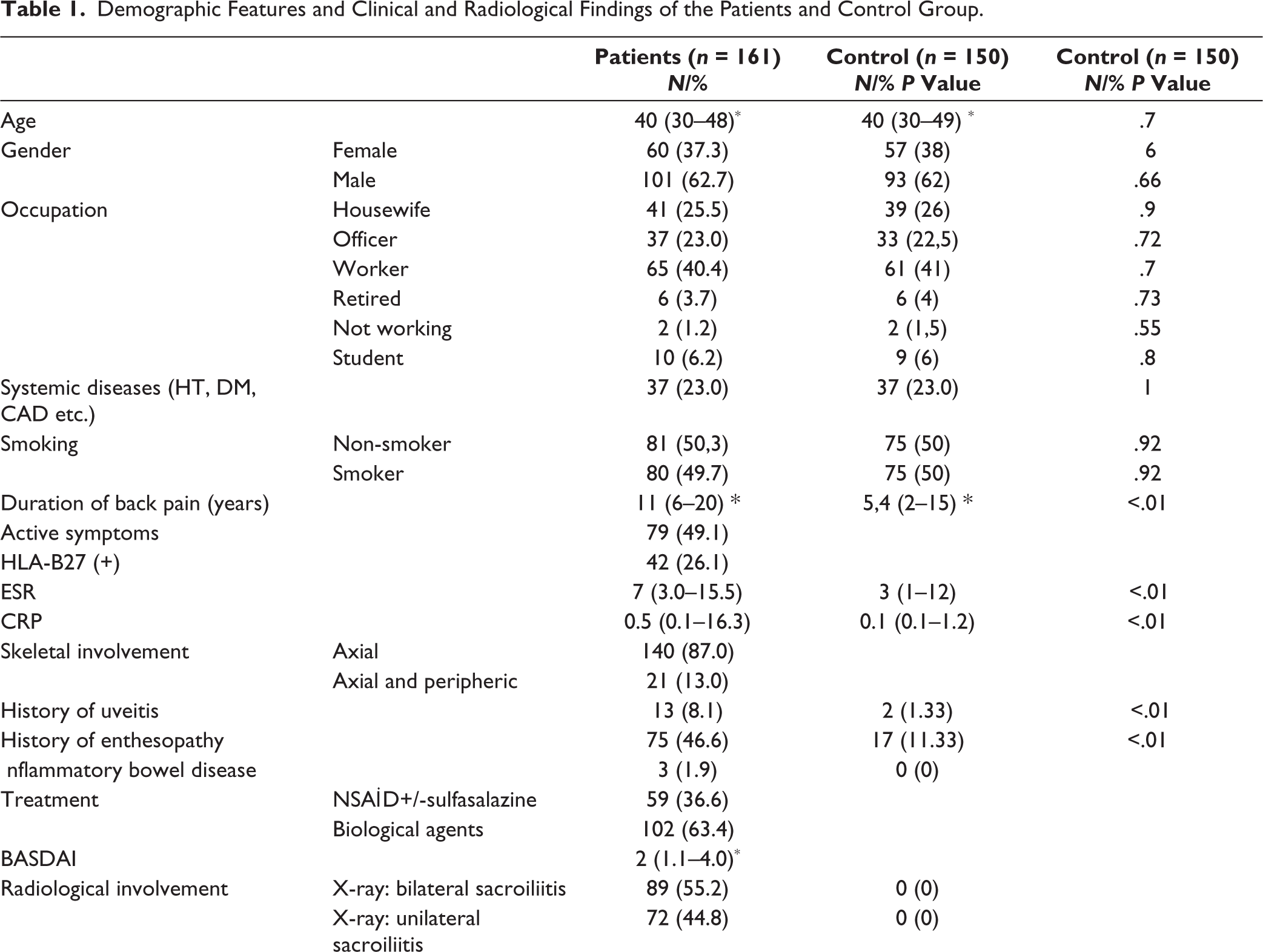
Notes:*Median (IQR, 25th-75th).
IQR: interquartile range; ESR: erythrocyte sedimentation rate, CRP: C-reactive protein; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index, HT: hypertension, DM: diabetes mellitus, CAD: coronary arterial disease, NSAID: nonsteroidal anti-inflammatory drug.
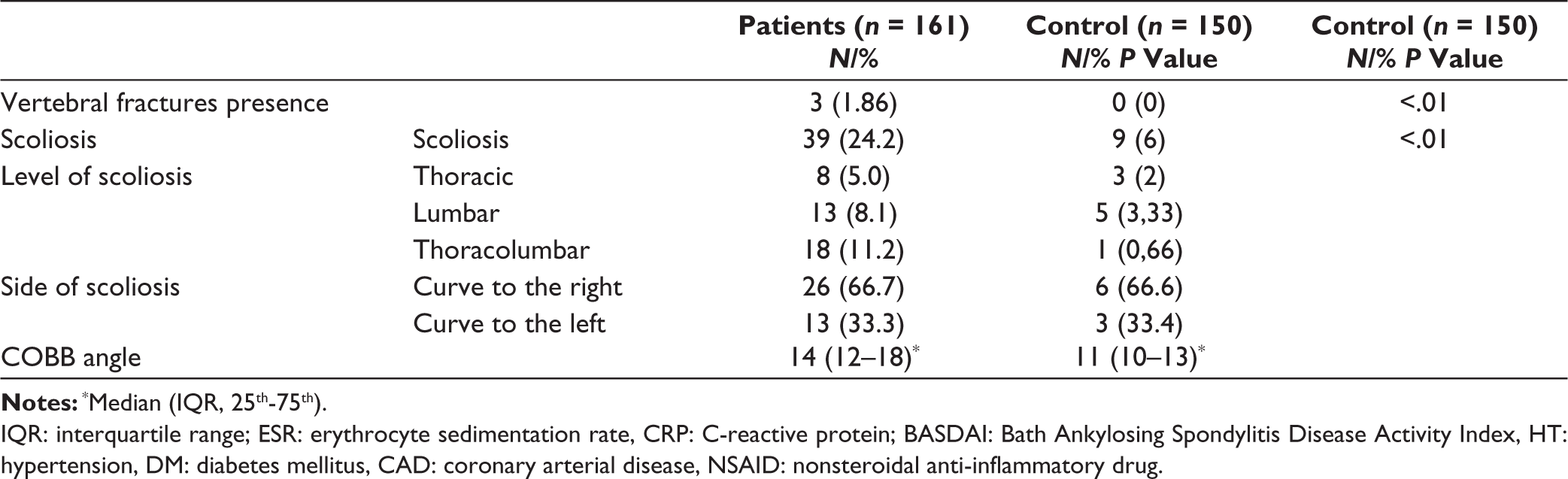
There are no differences between groups formed according to the presence of scoliosis in age, gender, smoking, medications, axial and axial plus peripheric involvement, HLA-B27 positivity, ESR, CRP, presence of enthesopathy, duration of inflammatory back pain and BASDAI (P > .05) in AS group. The frequency of uveitis and bilateral stage 4 sacroiliitis was significantly higher in the scoliosis-positive group (Table 2).
Comparison of the Clinical and Demographic Findings Between the Groups Formed According to the Presence of Scoliosis in Ankylosing Spondylitis Group.
bChi-squared test.
IQR: interquartile range; ESR: erythrocyte sedimentation rate, CRP: C-reactive protein; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; l˙BP: inflammatory back pain.
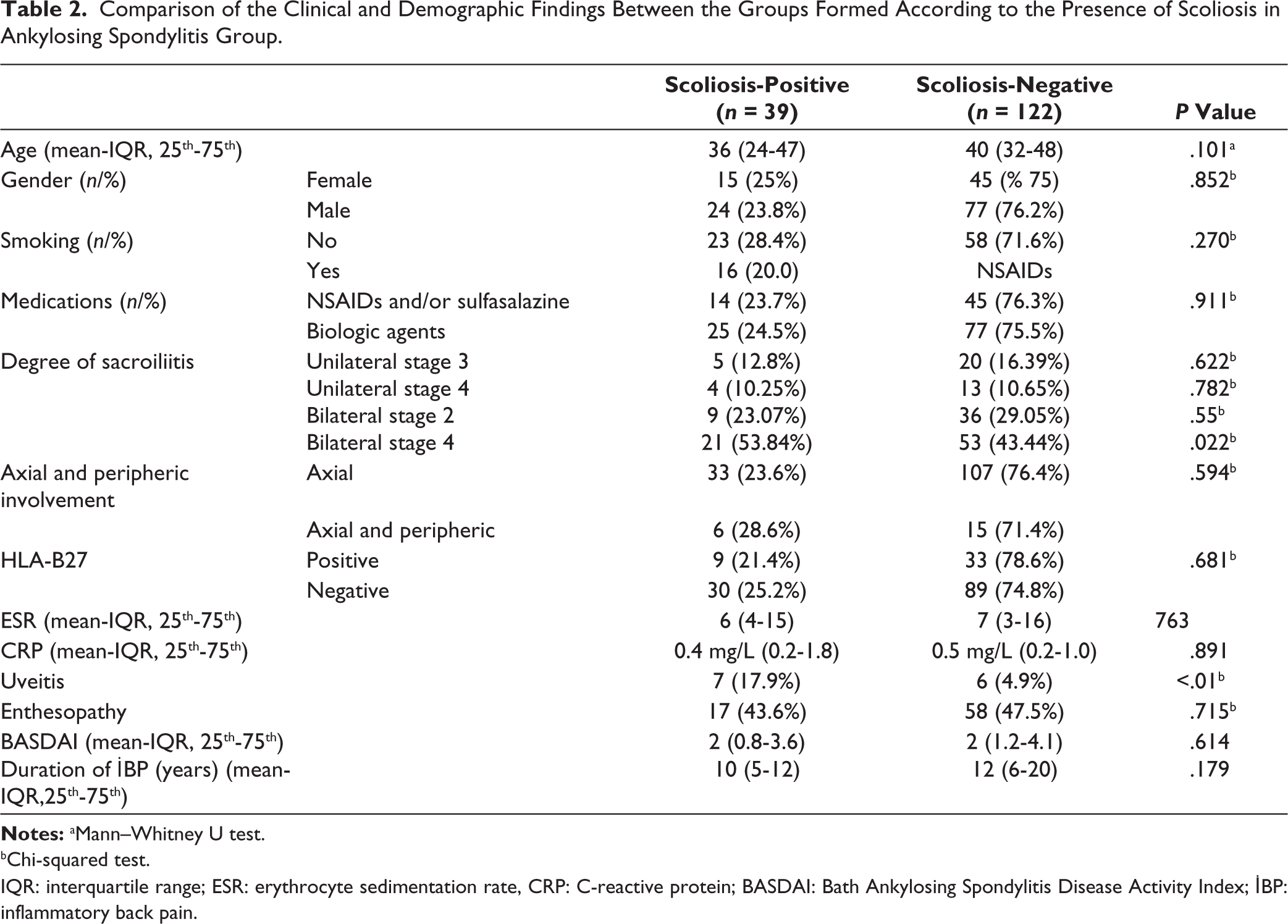
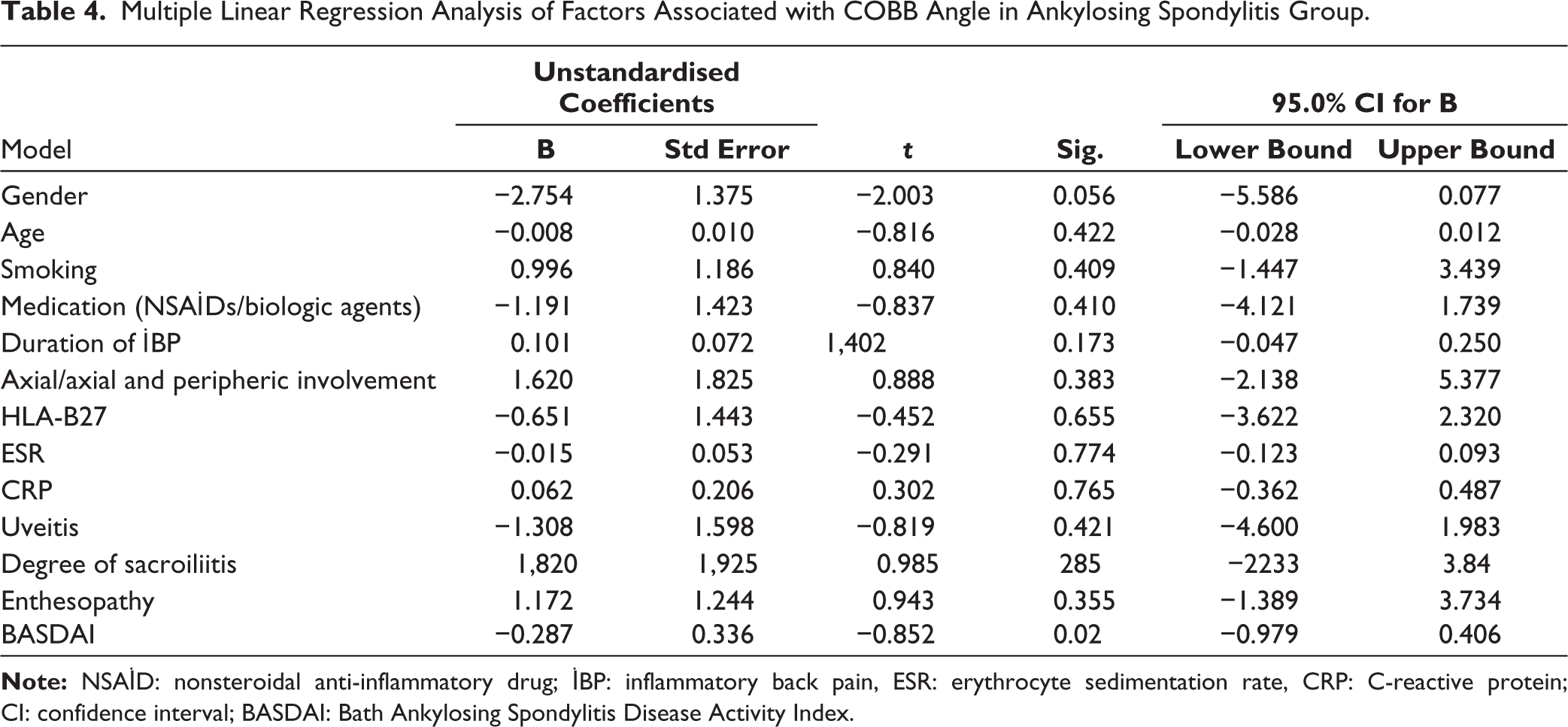
Binary logistic regression analysis revealed that uveitis (P = .015, odds ratio (OR) = 4.229), CRP (P = .037 OR = 1.245) and bilateral grade 4 sacroiliitis (P < .01, OR = 1.556) significantly increased the risk of the presence of scoliosis in the AS group (Table 3). However, multiple linear regression analysis found no variables associated with degree of Cobb angle (P > .05) in AS group (Table 4).
Univariable Binary Logistic Regression Analysis for Variables Associated with Scoliosis in Ankylosing Spondylitis Group (n = 161).
Multiple Linear Regression Analysis of Factors Associated with COBB Angle in Ankylosing Spondylitis Group.
Discussion
Our study is the first to investigate the frequency of scoliosis in AS. The Cobb angle was used as a measurement method and is a gold test used to evaluate scoliosis. The frequency of scoliosis has been reported to be approximately <5% in normal population studies.12,15 While scoliosis frequency was 24.2% in the AS group and 6% in the control group, scoliosis was more frequent in the AS group as statistically significant (P < .01) in our study. It is known that AS generally affects young population and male gender involvement is at forefront. Similarly, our study found that the mean age was 38 years, while the male ratio was 61.5% in 39 scoliosis-positive patients and 63.1% in 122 scoliosis-negative patients.
The typical hunchback posture seen in a patient with AS is caused by the presence of neck flexion deformity, thoracic hyperkyphosis, loss of normal lumbar lordosis and hip flexion deformities together. 16 The patient tries to compensate for lumbar flexion with hip movement, which forces the hip into flexion. When the gait of patients with AS was compared with healthy controls, decreased step length in the sagittal plane, increased pelvic movements and lower extremity angles, and flexion contractures of the hip were found. 17 Significant postural changes are seen in AS, such as downward and forward displacement of the centre of gravity with increased thoracic kyphosis, hip flexion secondary to ankle and knee flexion. 18 As the prognosis of the disease progresses in AS, the centre of gravity shifts forward and downward due to kyphosis; the body tries to bring the centre of gravity back above the base of support by performing knee flexion, ankle plantar flexion and hip flexion; and thus flexion contractures may develop in the hip. 19 Hyperkyphosis is the most common postural abnormality in AS. Squaring of a vertebra is an early radiographic sign of spinal involvement in AS. In later stages of AS, syndesmophytes and ankylosis occur in facet joints. Bamboo spine often develops in late AS. 9 When we look at relationship between disease activity, and clinical evaluation parameters and posture in patients with AS, we see that there are limited studies in literature. Rosu et al. reported that the pain score was higher in patients with kyphosis and scoliosis in AS patients, Bath Ankylosing Spondylitis Functional Index (BASFI) score was significantly higher in patients with kyphoscoliosis, while Bath Ankylosing Spondylitis Metrology Index (BASMI) score was lower in patients with scoliosis. 20 Kurtoğlu et al., in Turkey in 2019, scanned 44 AS patients and 44 healthy volunteers using a Zebris CMS20 three-dimensional ultrasonic system and found that angle of thoracic kyphosis had a statistically significant positive correlation with age of onset of symptoms and distance from tragus wall-distance (P < .05). 21 Unlike this study, we did not find any association of lumbar scoliosis with clinical features and disease activity in our study.
Studies of scoliosis in the normal adolescent population appear quite frequently in literature. The frequency of AIS was investigated in Sao Paulo; 2562 people between the ages of 10-14 were evaluated for scoliosis and scoliosis was detected in 1.5% of adolescents. 22 Sixteen thousand forty-five students were evaluated for scoliosis and prevalence of AIS was found to be 2.3% (female, 3.1%; male, 1.5%) in a study conducted in Turkey. They stated that the most common single type of curvature was the lumbar curve, and 90.5% of cases with AIS had a mild (between 10 and 19 degrees) Cobb angle. 12 Unlike this study, in our research, 18 (11.2%) of 39 patients with scoliosis had thoracolumbar scoliosis, and similar to this study, 89.22% of patients with scoliosis had a mild 14 (12-18) Cobb angle in the AS group.
The incidence of axial spondyloarthritis in patients diagnosed with scoliosis and control patients over seven years was investigated in a retrospective longitudinal cohort study conducted in Taiwan in 2022; the incidence of axial spondyloarthritis was found to be 141/100,000 people in the scoliosis group and 46/100,000 in the control group. 23 Lumbar scoliosis was found in 28 (7.7%) of 360 patients who met ASAS axial spondyloarthropathy criteria, and the mean Cobb angle was 3.2 ± 5.0. They found that lumbar scoliosis was not associated with inflammatory or degenerative changes in patients with early disease suggestive of axial spondyloarthropathy. 24 Unlike this study, we found that the frequency of scoliosis was higher in our study (7.7% / 24.2%); this may have been due to the smaller number of patients, the higher average age since degenerative scoliosis may develop, and the fact that we included AS patients who developed sacroiliitis on direct radiography instead of axial spondyloarthropathy (the disease is more advanced and may cause kyphosis and scoliosis).
No study in the literature has examined the relationship between scoliosis and uveitis. We reviewed the articles that studied uveitis in adolescence since there are no studies in the literature on the association of scoliosis with uveitis in adult patients, and since AS and scoliosis often begin in adolescence. Studies on uveitis in adolescence were mainly related to juvenile idiopathic arthritis, the most common chronic arthritis of childhood. It is known that the most common extra-articular manifestation of juvenile idiopathic arthritis is uveitis. Uveitis was found in 24 (6.7%) of 354 juvenile idiopathic arthritis patients. 25 In our study, 13 (8.1%) patients had a history of uveitis and only uveitis was only variable associated with higher prevalence of scoliosis. Although uveitis was found to be related to the presence of scoliosis in binary logistic regression analysis, no association was found between uveitis and Cobb angle in multivariate logistic regression analysis. The weak association between the presence of scoliosis and uveitis may be due to the severity of AS disease, not due to scoliosis.
We do not have certain information about why scoliosis increases in AS. Both scoliosis and AS are frequently encountered in adolescence. Vertebral damage, possibly secondary to AS, triggers the formation of scoliosis. Scoliosis can affect mechanical load and cause secondary changes in sacroiliac joints and lumbar spine. 24 Future studies are expected to shed light on this issue.
The limitations of the study were that it was single-centred, that there were no other inflammatory patient groups were not used as a control group, failure to evaluate data related to BASMI and BASFI, and that the patients were not followed for a long time to investigate whether high CRP, bilateral stage 4 sacroiliitis and uveitis affect the prognosis of the disease in the scoliotic group.
Conclusion
Our study revealed that scoliosis was more common in AS, reaching 24.2% of AS cases compared to 6% in the control group. The presence of scoliosis was not associated with disease activity parameters, except for CRP levels, uveitis and the degree of sacroiliitis. Further research is needed to confirm and explain the association of higher frequency of CRP, uveitis findings and higher sacroiliitis degree among AS cases with scoliosis.
Footnotes
Authors’ Contribution
GDK helped in designing the study, collecting, analysing the data and writing the manuscript.
OCI was involved in analysing the data and writing the manuscript.
FB helped in designing the study, analysing the data and coordinating the study.
ESB contributed to data collection and interpretation.
All co-authors of the study take full responsibility for the integrity of the final version of the manuscript.
Code Availability
Not applicable.
Consent for Publication
Not applicable.
Data Availability
Will be sent by the corresponding author upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ankara City Hospital No. 2 Clinical Research Ethics Committee Presidency (E. Kurul-E2-22-1301). All procedures performed in studies involving human were in accordance with the ethical standards of the institutional research committee (Ankara City Hospital No. 2 Clinical Research Ethics Committee Presidency) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written and verbal informed consent was obtained from all patients.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.