
Abstract
Objective
To improve the rate of first-hour breastfeeding in term and near-term healthy neonates by a quality improvement (QI) study at Secondary Care District Hospital.
Design
QI study.
Setting
Labor room-operation theatre of a secondary care district hospital.
Participants
Stable newborns ≥35 weeks of gestation born by normal vaginal delivery and by cesarean section under spinal anesthesia.
Procedure
A team of nurses, pediatricians, obstetricians, and anesthetists analyzed possible reasons for delayed initiation of breastfeeding by flow chart and Fishbone analysis. Various change ideas were tested through sequential Plan-Do-Study-Act cycles.
Outcome measure
Proportion of eligible babies breastfed within 1 hour of delivery.
Results
The rate of first-hour initiation of breastfeeding increased from 69% to 88% in normal vaginal deliveries and from 17% to 61% in the cesarian section over the study period, which were sustained up to 80% in normal vaginal deliveries (NVD) and 55% in lower segment cesarean section.
Conclusions
A QI approach was able to accomplish sustained improvement in first-hour breastfeeding rates in normal and cesarean deliveries.
Introduction
Problem Description
Breastfeeding practices like initiation of breastfeeding within 1 hour of birth and exclusive breastfeeding for the first six months of life have immense public health importance. However, the status of breastfeeding practices is far from satisfactory in India where the rate of initiation of breastfeeding within 1 hour of birth is 41.6% while the exclusive breastfeeding rate is about 55%. 1
Less than one-fourth (21%) of children were breastfed within 1 hour of birth across the different districts of India. Findings suggest when women did not breastfeed their newborn within 1 hour after his birth, the odds of neonatal deaths were increased by nearly threefold in comparison with those neonates who breastfed within 1 hour of birth. Population Attributable Risk estimates that the risk of neonatal deaths could be reduced to a maximum of 15% when all babies are exposed to early breastfeeding from the present level of breastfeeding. 2
There is a significant rise in institutional delivery rate to more than 80%. So, we must try to find out the reason for the delayed initiation of breastfeeding in normal delivery and lower segment cesarean section (LSCS) at the institutional level. 3 Despite all the evidence-based facts regarding the importance of the early initiation of breastfeeding following birth, in reality, as mentioned above, the status of first-hour breastfeeding rates is far from satisfactory in India. Therefore, we had planned a quality improvement (QI) process involving a series of Plan-Do-Study-Act (PDSA) cycles to improve the rates of first-hour initiation of breastfeeding in babies born through cesarean section and normal delivery.
Available Knowledge
The World Health Organization (WHO) has recommended placing babies directly on the breast for at least 1 hour immediately after birth irrespective of the mode of delivery. 4 Breastfeeding in the first hour of life is associated with prolonged duration of breastfeeding5, 6 and reduction of infant mortality, especially in developing countries.7–9 Breastfeeding within the first hour of life prevents newborn death due to sepsis, pneumonia, diarrhea, and hypothermia. 10
The WHO and United Nations Children’s Fund recommend that breastfeeding should be initiated within 1 hour of birth because early initiation stimulates breast milk production, increases uterine activity, and may thus reduce the risk of heavy bleeding and infection. It also fosters mother-child bonding and increases the duration of breastfeeding. 11
Rationale
Existing literature shows that education and supportive interventions, both for breast-feeding mothers as well as for healthcare professionals, can increase the proportion of women who use exclusive breastfeeding, however, more evidence is needed on the effectiveness of group interventions. 12 In the present study, we tried to find out whether a QI approach is beneficial or not; whether the change of idea is accepted or rejected in a secondary care district hospital.
Methodology
It was a QI study. We were associated with the district hospital as a teaching hospital and providing secondary-level care since our medical college building was not ready at the time of the study.
Context
District hospital had been selected which is attached to our medical college. It caters almost more than 15 lacs population to provide health care facilities. It is a referral hospital for this district and the only government facility for LSCS. Our center labor room caters almost more than 500 deliveries per month. About four to five LSCS is conducted daily (more than 120 LSCS per month), comprising approximately 20%–30% of whole deliveries.
Intervention
PDSA Cycles Protocol
Our basic aim was to improve quality care in this secondary care hospital to enhance first-hour feeding and to monitor it with repeated reinforcement over some time (four cycles of 15 days each for two groups of deliveries). If these changes have been adopted by hospitals it would improve neonatal morbidities and mortalities at the district level. The steps taken by us for this study were:
Measuring baseline rates of first-hour feeding in both normal vaginal deliveries and LSCS patients by asking the mothers after taking written informed consent. Identifying causes of delayed initiation of first-hour feeding. Making a team of pediatricians, obstetricians, anesthetists, nurses in charge of operation theatre (OT) and labor room, obstetric ward and investigator who was an Undergraduate MBBS student along with faculty members from the department of pediatrics as a guide. Conducting meetings of all stakeholders to identify the reason for delayed initiation with flow chart and fishbone analysis and possible solutions at every level from nursing staff to doctors. Conducting two cycles of the PDSA procedure conducted in the two groups of deliveries—NVD and LSCS. All possible solutions were first implemented in the labor room followed by the OT. The numbers of babies with initiation of feeding in both normal vaginal deliveries and LSCS were assessed after implementation of these changes. A sustenance phase of 15 days was also evaluated to see whether the change was accepted or rejected.
Sampling Technique and Sample Size
Inclusion Criteria
All the babies who were delivered at the center over two months were the target population. We included only babies with the following
Newborn with weight more than 2,500 g (term and near term beyond 35 weeks of gestational age).
Apgar scores more than seven at birth.
No maternal intrapartum and antepartum complications affecting baby feeding.
No medical disease/contraindications for feeding restrictions.
Exclusion Criteria
Hemodynamically unstable neonates and neonates need admission to the neonatal intensive care unit.
Patients with respiratory distress or severe birth asphyxia with feeding restrictions.
Mothers were sick, that is, eclampsia and unconscious mother.
Feeding was contraindicated due to congenital malformation or any medical condition.
Weight below 2,500 g and gestational age below 35 weeks.
Data Collection Procedure
All the neonatal data was collected from labor room-OT complex.
Study of Interventions
Descriptive statistics were used for analysis. Qualitative data analysis was also done after interviews with nurses, mothers and doctors. Reasons for delayed breastfeeding were studied via fishbone analysis in both NVD and LSCS.
Measures
Fishbone Analysis
The Ishikawa or fishbone diagram is used when a team seeks to understand the many potential causes contributing to the quality-of-care problem and focus improvement efforts on these causes. 13 We used this tool for the study of causes of delayed initiation of breastfeeding in both NVD and LSCS in each PDSA cycle.
Qualitative Assessment Protocol and Interview Guide
A series of interviews with six mothers, three pediatricians, three obstetricians, and six nursing staff were conducted to identify the reason for the delayed initiation of breastfeeding beyond 1 hour and possible solutions if any. A semi-structured interview guide was developed containing mostly open-ended and broad questions related to the topic. It was first prepared in English and then translated into the local language which was Hindi in this part of the country.
Data Analysis
Baseline Period (5 July 2019 to 20 July 2019)
Baseline rates of first-hour feeding in both normal vaginal deliveries and LSCS patients were measured by asking the mothers after taking written informed consent. Also, by asking the mothers and nursing staff, reasons for the delay in the initiation of breastfeeding were found in both cases. The data was collected by the MBBS student by asking the mothers in the post-delivery ward for NVD and the Postoperative ward for LSCS mothers. The data was collected at the same time for both LSCS and NVD. For NVD baseline average of first-hour breastfeeding was 69% and for LSCS was 17%.
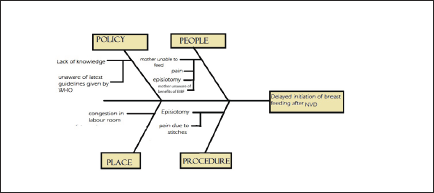
Fishbone Analysis for Causes of Delayed Initiation of Breastfeeding in Normal Delivery (Figure 1)
In the majority of the cases of delayed initiation in normal vaginal deliveries, the main cause was the inability of the mother to feed the baby because of the post-episiotomy pain. A strong connection was found between delayed initiation of breastfeeding and episiotomy. There were a few cases in which mothers didn’t feed the baby early as they didn’t know and were not informed about this by any health care provider. A few cases were found in which the mother couldn’t feed the baby due to crowd in the labor room.
Fishbone Diagram of Possible Reasons for Delayed Initiation of Breastfeeding After Normal Vaginal Deliveries
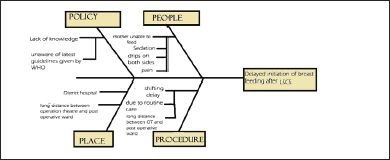
Fishbone Analysis for Causes of Delayed Initiation of Breastfeeding in LSCS (Figure 2)
In cesarean section, the most prevalent cause of delayed initiation was found to be the time taken to shift the mother from the OT to the post-operative room. In the chosen hospital this delay is firstly, due to routine care and secondly, due to the distant placements of the OT and the post-operative ward. Another reason was the condition of the mother. Most of the time due to sedation, and/or due to drips in both forearms: the mother after the C-section was not in a state to breastfeed the baby by herself.
Fishbone Diagram of Possible Reasons for Delayed Initiation of Breastfeeding After Cesarean Delivery.
PDSA Cycles: NVD
PDSA #1 (21 July 2019 to 4 August 2019)
Pictorial infographics were sent personally to the duty nursing staff via WhatsApp regarding the benefits of first-hour breastfeeding, before their duty hours. One offline meeting was held at the labor room nursing station in the presence of the nurse in charge in the morning hours. Reminders via phone calls in the evening. The reasons for the delayed initiation of breastfeeding were
Due to post episiotomy pain. Lack of knowledge. Crowd in the labor room.
PDSA 2# (5 August 2019 to 19 August 2019)
The first meeting was conducted on 5 August 2019, in which nursing staff was taught to counsel mothers that breastfeeding will also help them in relieving pain due to episiotomy. They were instructed to breastfeed the baby just after episiotomy. The staff was also instructed to counsel the mothers about the importance of first-hour breastfeeding. The second remainder meeting was held seven days after the first meeting, that is, on 12 August 2019. The nursing staff ensured that the baby was fed just after the episiotomy.
Sustenance Phase (20 August to 3 September 2019)
An average of
PDSA Cycles: LSCS
PDSA #1 (21 July 2019 to 4 August 2019)
We planned to sort out the reasons for the delayed initiation of breastfeeding in a LSCS delivery. The reasons were:
Shifting delay from OT to post-op ward/long distance from OT to post-operative ward. Sedation of mother and/or drips in both hands. Lack of knowledge among healthcare staff as well as mothers.
Pictorial infographics were sent personally to the duty nursing staff via WhatsApp regarding the importance of first-hour breastfeeding and also about the guidelines that it does not depend on the mode of delivery, before their duty period. One offline meeting was held at the labor room nursing station in the presence of the nurse in charge in the morning hours. The nursing staff were trained regarding the latest guidelines by WHO regarding the early initiation of breastfeeding. The nursing staff was told to feed the baby in the OT after the basic newborn care. The nursing staff was also instructed to help and teach the attendants of the mother to assist the feeding by holding her baby even if she was sedated or had drips in her hands (in the postoperative ward).
PDSA 2# (5 August 2019 to 19 August 2019)
In PDSA 1, the nurse who tried to feed the baby in OT said that she was facing difficulty in feeding the baby during the operation. Also, the doctors were not comfortable.
Therefore, the OT nursing staff was told to wait till the completion of the suturing process and then breastfeed the baby in the OT. The baby was fed with the help of the Pediatric Nurse who attended the baby, after the basic newborn care. The feeding also continued after shifting the mother to the postoperative ward at 2-hour intervals.
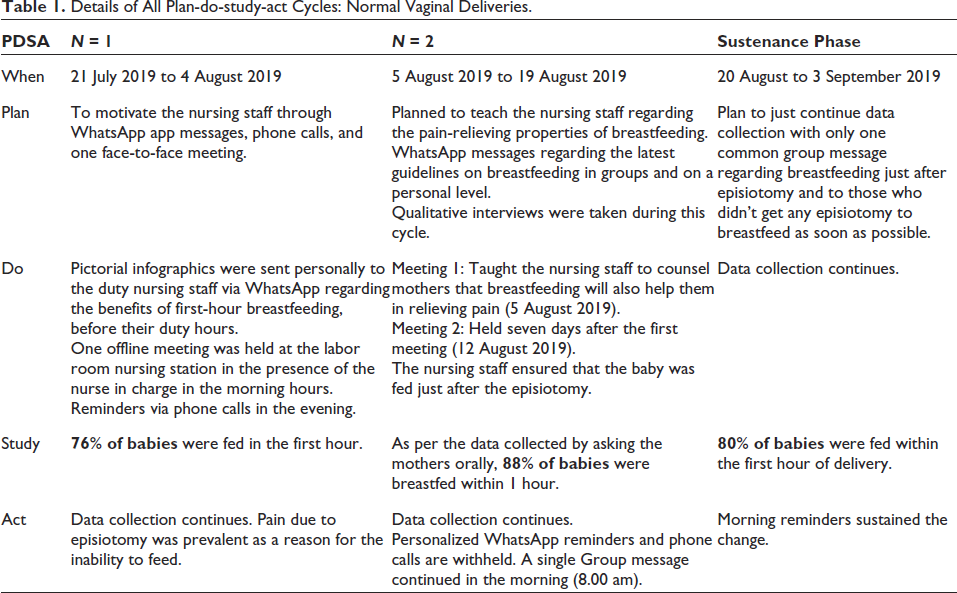
Details of All Plan-do-study-act Cycles: Normal Vaginal Deliveries.
Sustenance Phase (20 August to 3 September 2019)
The average percentage of early initiation of breastfeeding in the sustenance phase was 55%.
Qualitative Data Analysis
Interview 1 (Mother Breastfeeding in the Post-operative Room)
A mother whose baby
Interview 2 (Mother with Breastfeeding in the Operation Theatre)
Another lady whose baby
Interview 3 (Sick Newborn Critical Unit Staff Nurse)
The nurse who first started feeding the baby in the operation theatre, “In normal deliveries almost all babies are breastfed within one hour. In cesarean sections, there may be some delay during shifting the mother from OT to the post-operative ward. But now I have started putting the baby on the mother’s breast in the operation theatre just after suturing, but till then I have to wait.” She then added, “There come many patients who don’t know to see the watch, so there will be cases where they gave wrong information to you about the timing of breastfeeding.”
Interview 4 (Senior Resident in Dept. of Pediatrics))
He was unaware of the latest guidelines regarding early initiation of breastfeeding for cesarean deliveries. He knows the old guidelines of breastfeeding within 4 hours in cesarean cases. He then added, “At this district hospital, due to lack of knowledge, all babies are not breastfed in the first hour.” He felt a need to educate the nurses regarding breastfeeding the baby in the operation theatre.
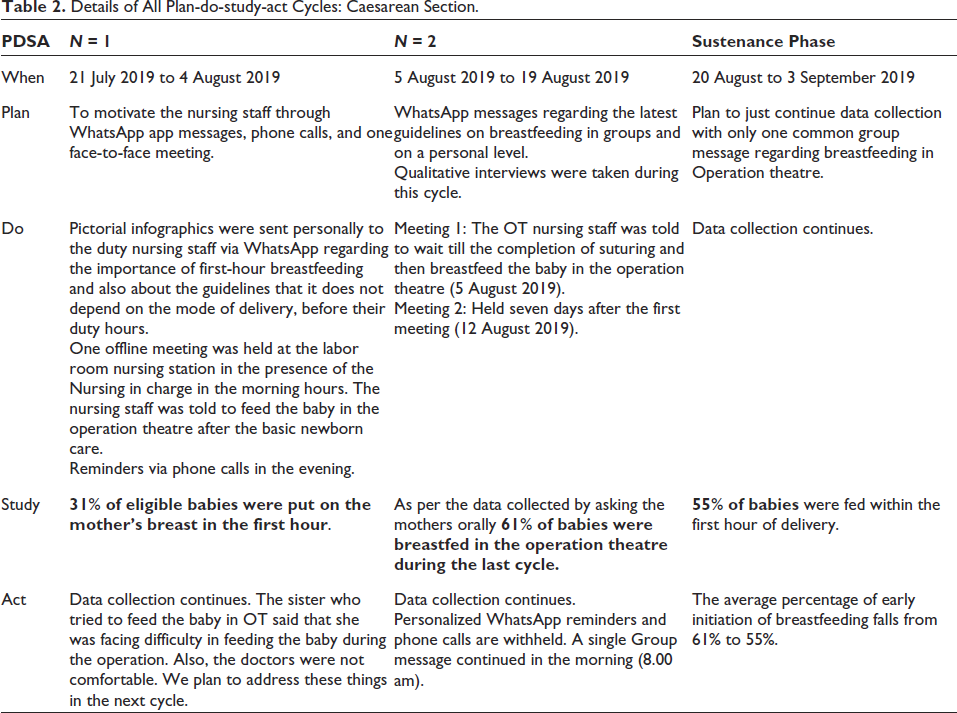
Details of All Plan-do-study-act Cycles: Caesarean Section.
Ethical Consideration
Permissions from the Institutional Research Committee and then from the Institutional Ethics Committee were taken before starting the study.
Results
Normal Vaginal Deliveries
During our course of study, the baseline rates that we found were that about 69% of babies were fed within the first hour of their life. In the remaining 31% of cases, the major reasons for not feeding were mothers undergoing episiotomy, lack of knowledge, not told by the nurses, baby was not crying. After the interventions in subsequent PDSA cycles, the average no. of cases of early breastfeeding increased to 76% and 88% in PDSA 1 and PDSA 2 respectively. In the sustenance phase, the rates dropped to an average of 80%. Overall, the change of idea that we planned to put in the system was retained as the average rates of first-hour initiation of breastfeeding were increased from 69% in the baseline period to 80% in the sustenance phase.
Cesarean Section
In cesarean section, initially, an average of 17% of babies were fed within the first hour of LSCS delivery. Most were used to feed when their mothers got shifted to the post-operative ward. In the majority of the cases, this shifting period is almost 1–1.5 hours. Even after that, some attendants waited for the mother to wake which also took an extra 0.5–1 hour. After the intervention, the nursing staff started helping the mother to breastfeed the baby in the OT herself. In PDSA 1, the average no. of cases of early initiation increased to 31%, then in PDSA 2 to 61%. In the sustenance phase, the rates were 55%. In cesarean section, the change of idea was retained as the baseline rates were 17% and they increased to 55% in the sustenance phase.
Chart 1 shows improvement in both normal deliveries and cesareans after 2 PDSA cycles in each group.
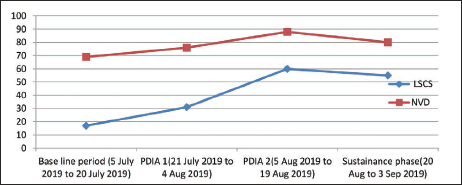
X-axis—Timeline showing baseline period, PDSA cycles, and sustenance phase.
Discussion
Normal Vaginal Deliveries
In normal vaginal deliveries, we were able to raise the first-hour breastfeeding rates from the baseline of 69%–88% in the second PDSA cycle which falls to 80% in the sustenance phase. The change of idea was accepted by the system but not to the extent that we expected. Delays in the time of repair of episiotomy and labor duration less than 12 hours were associated with early breastfeeding initiation. 14 The present study shows that pain due to episiotomy was one of the hurdles in the early initiation of breastfeeding.
Routine and successful nursing is crucial for the health of infants and is influenced by maternal education. 15 Provision of training to the birth attendants and other obstetric health workers including nurses and midwives on breastfeeding promotion, education, and counseling can be critical for increasing the effective initiation breast feeding (EIBF). Evidence shows that the presence of a breastfeeding-trained delivery assistant during childbirth increases the rates of EIBF in Nigeria. 16 Our results show that the rate of EIBF is 61% higher among women who along with their child received postnatal care from a healthcare provider within 1 hour of birth. This practice is strongly supported by the WHO recommendation—that postnatal visits should happen as early as possible after birth. 17
In the present study, it was shown that proper support given by the nursing staff to the mothers within the first hour helped to increase the percentage of first-hour breastfeeding. In the study, in each group (NVD and LSCS), we have done 2 PDSA cycles of 15 days duration each, with a sustenance phase of the next 15 days. Due to a very slow improvement rate, there should be a greater number of such cycles and a longer sustenance phase to confirm whether the newly implemented process is continuing or not even after the completion of the study period.
Cesarean Section
About 83% of babies born via LSCS were fed about one and a half hours after the delivery when the mother was shifted out of the OT into the post-operative hall. In 17% of cases, the shifting delay is between 45 minutes and 1 hour, so only such mothers will be able to breastfeed their baby at or within 1 hour. We need to replace this usual incorrect process by the WHO recommended guidelines of putting the newborn in the mother’s breast for feeding within 1 hour irrespective of the mode of delivery. 1
A very similar study, done by Dudeja et al., was able to improve the initiation rates of first-hour breastfeeding from 0% to 93%. 18 In the present study, we were able to bring a change from 17% to 60% in PDSA 2 while an average of 55% in the sustenance phase in the cesarean section. The reason behind different results may be due to different settings. The previous study was conducted in a tertiary care hospital while the present one was accomplished in a secondary care district hospital.
Another QI initiative was undertaken from July 2016 to January 2017 at a 50-bedded secondary care hospital by Kaur et al. taking NVD as the study population. 19 They demonstrated The rate of early initiation of breastfeeding improved from 52% at baseline to 97% in the immediate post-training phase; after an initial fall due to the shortage of staff, the EIBF rate was sustained at 91% after six months. This study was similar to the NVD section of our study.
A study conducted from October 2018 to December 2020 by Nagendla et al. showed a significant improvement in delayed cord clamping (DCC) (median) from a baseline of 25%–96% over a two-year period. As a co-process, EBFI improved (median) from a baseline of 50%–97% without any major intervention in the system. 20 This study includes sensitization, making DCC part of the pre-birth checklist, and recording outcomes on a dashboard daily which helped to implement and sustain the processes over two years. The prebirth checklist, outcome recording, and a longer sustenance phase could have been the reason for better results which were not present in the present study.
Initially, opposition was faced against the practical implementation of the correct timing of breastfeeding. The opposition was due to the difficulties faced by the nurses. The duty nurse has to attend both caesarian sections as well as normal deliveries. For feeding the baby in the OT they have to cover a large walking distance between the OT and the labor room. They also find the OT table too small to be able to breastfeed the baby at the time of suturing. This may not be a genuine reason as the size of the OT table is identical all across the country.
On discussion with the nursing staff about the problems they faced and the possible solutions were implemented in the next PDSA cycle. The benefits of early breastfeeding were taught to them as well as the harms to the baby if not getting the early breast feed. The change in the process was that the circulating nurse would wait till the suturing process and then she would breastfeed the baby on the table, after the basic newborn care, before handing over the baby to the attendant. The nurses agreed to wait as they would do their writing work during this time.
Simultaneously the pediatricians, obstetricians, and gynecologists were requested to ensure whether the baby was breastfed in the OT or not. All junior and senior residents were also requested to ensure the first-hour breastfeeding while attending the deliveries. In the district hospital perhaps, this change came for the first time and the nursing staff and even doctors were not aware that it could even be possible practically that the babies born in cesarean section can be breastfed on the OT table in the OT itself.
Perinatal and neonatal nurses should be leaders in changing practice to incorporate early skin to skin contact into routine care after cesarean birth. 21 The current study supports that skin-to-skin contact was feasible during breastfeeding after cesarean and could be provided for healthy mothers and infants immediately after cesarean birth.
Limitations
There were some limitations of the present study too. First, the data collection was done based on asking the mothers directly about the timing of first breastfeeding just after the delivery. There may be some chances that some mothers had talked about the false timing due to confusion or any other reason. There was a conflict in the saying of mothers and the nursing staff. When we talked to the labor room nursing staff, they said that they were feeding all the babies timely. When we asked a mother about when she breastfed her baby she said after 1 hour, when the same question was asked to her by a labor room sister she said, within 1 hour.
The second limitation may be that the study population was changing every day. However, this could not affect the study as it is trying to improve the quality at the institutional level which remains constant throughout the study period. One more difficulty that was faced by the investigators was to locate the mothers who delivered in the past 24 hours who were shifted to very different wards. Every day there was always a possibility of missing one or two mothers from asking them about the first hour breast feeding of their baby. Fourthly, the study had also a shorter period of intervention; 15 days of PDSA cycles with only 2 PDSA cycles. The sustenance phase can also be of longer duration to assess more accurately the rejection or acceptance of the idea.
Conclusion
By the present study, we can conclude that the methodology used in the study to improve the rates of first-hour breastfeeding in both normal vaginal deliveries and cesarean sections is found to be effective in a secondary care district hospital and can also be applied in other secondary as well as tertiary care hospitals. This study can be more effective if done with more PDSA cycles, with a longer duration of sustenance phase; ensuring the continuity of the new change even after the study duration. The study has revealed that there is a dearth of knowledge among the health care providers—including doctors as well as nursing staff—about the latest guidelines by the WHO. Lack of information about the latest updates is also a major factor that hinders the implementation of correct methods regarding any healthcare facility.
Abbreviations
EIBF: effective initiation breast feeding
LSCS: lower segment cesarean section
OT: operation theatre
PDSA: Plan-Do-Study-Act
QI: quality improvement
WHO: World Health Organization
Footnotes
Acknowledgments
The authors would like to acknowledge the study participants for their time and engagement in this study. The authors are also grateful to the Nurses and Midwives who made data collection possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Research Committee and the Institutional Ethics Committee of Atal Bihari Vajpayee Government Medical College, Vidisha, Madhya Pradesh, India.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.