
Abstract
Background
Mother’s own milk for preterm infants is a complete nutrition. In NICUs, there is a delay in starting and decreased frequency of breast milk expression leading to inadequate supply of mother’s own milk for preterm babies. There is a lack of knowledge about the importance of mother’s own milk for preterm babies in the general population and a paucity of studies on this topic from Bangladesh. This quality improvement initiative will serve as a baseline study for increasing the use of mother’s own milk for preterm babies in our country.
Objectives
To observe the effects of the quality improvement initiative to increase the supply of mother’s own milk for preterm newborns admitted in the NICU.
Methods
This QI study was conducted in the Department of Neonatology, in collaboration with the Department of Obstetrics and Gynaecology, Bangabandhu Sheikh Mujib Medical University, Dhaka, over the period of 1 year. Inborn Preterm neonates ≤34 weeks and/or ≤1800 gm and mother dyads, anticipated to stay in NICU for ≥ 7 days, were included in this study. In the observation phase, baseline data were collected. The intervention phase was started with a comprehensive counseling package, the demonstration of breast milk expression, and the early (within 6 h of delivery) and frequent (2 h) expression of breast milk.
Results
A total of 96 preterm newborns and mother dyads were enrolled. There was an improvement in the percentage of mothers expressing breast milk within 6 h of birth and on day 1 from 0% to 100% and from 14.5% to 100%, respectively, after implementing the QI initiative. The amount of expressed breast milk on days 1, 3, and 7 in the intervention group was higher than that of the observation group. The percentage of neonates receiving only mother’s own milk on day 1 was increased from 14.5% to 100% after giving intervention.
Conclusion
A significant improvement in early expression of breast milk, an increase in total amount of expressed breast milk, and an exclusive mother’s own milk feeding among the preterm neonates admitted in the NICU were observed.
Introduction
Each year, about 15 million babies worldwide are born prematurely, that is about 1 in 10 children. Out of 3 million children born every year in Bangladesh, 0.6 million are born premature, and out of that 0.6 million premature births, 20,000 infants die. 1 More than half (54.5%) of the admitted newborns were premature in the NICU in the year 2022. Premature neonates face feeding challenges due to their immature GIT system, poor sucking and swallowing coordination, and delay in starting feed due to morbidities, leading to postnatal growth and nutritional failure. Mother’s own milk for preterm infants is a complete nutrition. Human milk refers to a combination of mother’s own milk and pasteurized donor human milk.2, 3 Use of donor milk is recommended when mother’s own milk is unavailable. It is a matter of great concern to help mothers in expressing and maintaining mother’s own milk through discharge. Premature newborns receiving mother’s own milk have a lower incidence of NEC, sepsis, and ROP than formula-fed preterm infants.4–6 In the long term, mother’s own milk reduces the risk of BPD and metabolic syndrome.7, 8 A positive relationship was seen between the quantity of breast milk received during hospitalization and neurodevelopmental outcomes in premature infants. 9 Mothers of the neonates admitted in the NICU face biological difficulties, stress related to NICU admission, and multiple challenges in establishing and maintaining an adequate supply of milk.10, 11 There is significant delay and less availability of mother’s own milk due to lack of effective communication, counseling, and lactation support. It is a real challenge for the health care team to overcome this constraint. Early and sustained availability of mother’s own milk will not only decrease overall morbidity and mortality but may also ensure adequate weight gain to prevent extrauterine growth retardation and lesser duration of hospitalization. 12 It is known that premature breast milk contain more protein, fats, calories, and antibodies than mature milk to meet the need of a premature baby and most of the time this shared breast milk is mature milk that is not tolerated by the premature gut. 13
Quality improvement initiatives have been shown to increase the proportion of preterm infants on mother’s own milk from 10% to 81% during the intervention phase at day 7 of admission and 66% during the sustenance phase. 14 Although the rates of human milk use in the NICU have improved during the last decade, efforts to help mothers in expressing and maintaining mother’s own milk is still lacking in our country. This study was designed to document the impact of quality improvement initiative by using a comprehensive counseling package to increase the supply of mother’s own milk for preterm newborns admitted in the NICU.
Materials and Methods
Study Design
This QI study was done in the Department of Neonatology, in collaboration with the Department of Obstetrics and Gynaecology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Shahbag, Dhaka, from March 2021 to February 2022, after getting the approval from the Institutional Review Board.
Eligibility Criteria
Inborn Preterm neonates ≤34 weeks and/or ≤1800 g and mother dyads who were anticipated to stay in the NICU of BSMMU for more than 7 days were eligible for enrolment. Infants with gross congenital anomalies, any surgical condition where there is a contraindication of breast milk, non-availability of mother’s own milk because of maternal indication such as a critically sick mother admitted in the intensive care unit, postpartum psychosis, and a mother on anti-cancer medication were excluded from the study.
Data Collection Procedures
A written informed consent was obtained from parents and assurance about confidentiality was given. Demographic and socioeconomic information, date of admission, mode of delivery, gestational age, birth weight, number of fetuses, and maternal illness were collected.
This study was conducted in two phases. In the observation phase (March 2021−June 2021), baseline data were collected. Baseline data included antenatal counseling related to the importance of mother’s own milk for a preterm baby, demonstration of breast milk expression, postnatal age of first breast milk expression, frequency of breast milk expression, percentage of mothers expressed their breast milk within 6 h of birth on day 1, day 3, and day 7; amount of expressed breast milk on day 1, day 3, and day 7; and percentage of newborn fed on only mother’s own milk and frequency of using shared breast milk. The amount and type of breast milk (mother’s own milk and shared breast milk) were documented in the breast milk expression chart by the principal investigator, other team members, and on-duty nurses. Shared breast milk was taken from the mothers who gave birth at term and most of the time it was transitional and mature milk. Parents kept the name and address of each other to prevent the marriage between “milk-siblings” (breastfed from the same mother) in the future.
Preterm neonates ≤34 weeks &/or ≤1800 g and mother dyads who were included in the observation phase were regarded as the observation group. The intervention phase was started 2 weeks after the observation phase. During this intervening period, a quality improvement (QI) team was formed which consisted of one faculty in charge, one resident physician, and two senior staff nurses. The principal investigator was a part of the QI team as a resident physician.
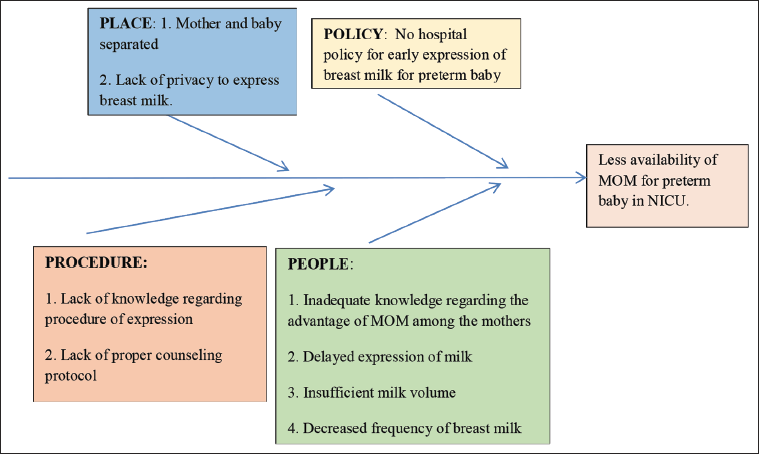
Fishbone analysis (Figure 1) was done to identify the possible factors for less availability of mother’s own milk in the NICU. Lack of antenatal counseling and demonstration of breast milk expression, delayed and less-frequent expression of breast milk, lack of privacy to express breast milk, and separation of mother and baby after birth due to NICU admission were found to be important root causes for less availability of mother’s own milk in the NICU.
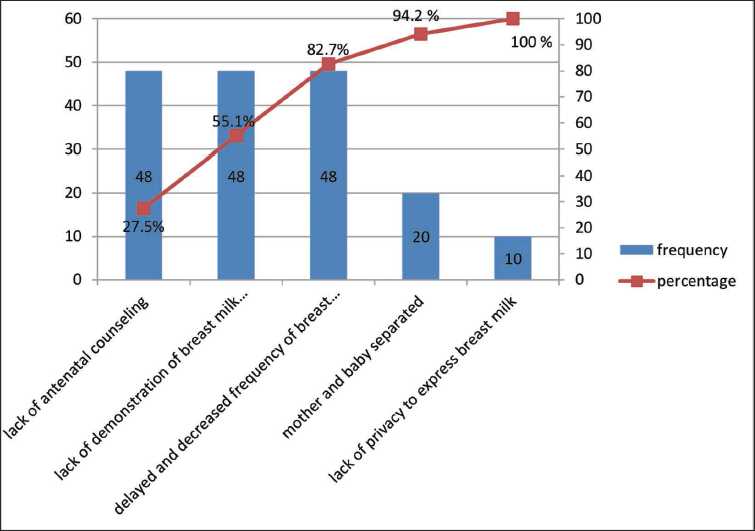
Pareto analysis (Figure 2) was done to choose a priority from the number of root causes. Bar charts present the actual data in descending order. The line graph presents the percentage of cumulative data in ascending order. Lack of antenatal counseling on early expression of breast milk, lack of demonstration of breast milk expression, and delayed and less-frequent expression of breast milk made an 82.7% contribution for less availability of mother’s own milk in the NICU. Thus, intervention was focused on these important root causes to eliminate them in order to increase the supply of mother’s own milk for preterm babies.
Pareto Analysis.
A quality improvement initiative was planned to increase the availability of mother’s own milk for eligible preterm neonates. This plan was shared with NICU health care professionals to sensitize them about the study.
The intervention phase (July 2021−February 2022) was started with the implementation of a quality improvement initiative. The component of the quality improvement initiative was comprehensive counseling package, demonstration of breast milk expression, and early (within 6 h of birth) and frequent (2 h) expression of breast milk.
In the intervention phase, counseling was done to all the eligible pregnant women who were anticipated to deliver ≤34 weeks of gestation, and the demonstration of breast milk expression was done to all the enrolled mothers (Intervention group). Counseling was done during the antenatal period in the antenatal ward, as well as during the admission in the NICU and throughout the hospital stay to keep the mothers motivated to express their breast milk. As a result, mothers found themselves emotionally connected to their babies admitted in the NICU which helped to reduce their anxiety and increase their mental strength. All these factors helped to initiate and maintain lactation.
Demonstration of breast milk expression was done both by hand and with the help of a manual breast pump. Hand expression was demonstrated during the antenatal period in the antenatal ward, after delivery in labor and post-operative rooms, and by breast pump from day 3 onwards in the NICU and postnatal ward. A practical demonstration using a dummy breast as well as on a mother’s breast and a video demonstration of the expression of breast milk through a mobile phone were delivered among team members, mothers, and caregivers. Mothers expressed breast milk in the post-operative and labor rooms just after birth, thereafter in the postnatal ward, in the NICU beside their babies’ beds, and also in the mother’s restroom.
Mother and caregivers were demonstrated the cleaning and sterilization procedure of the breast pump and milk container. They kept the breast pump and milk container in a food-grade plastic box with a lid.
Breast milk was expressed by hand during the first 2 days and measured by insulin syringe as colostrum was thick and small in amount. From day 3 onwards, breast milk was expressed by manual breast pump (Farlin Company) and measured by disposables syringes (10, 20, 50 mL). The amount of expressed breast milk was documented in the breast milk expression chart. Data on outcome variables were collected and a comparison was done between the two groups.
Data Analysis
After collection, data were entered into a personal computer, analyzed, and plotted in tables. Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 20. Quantitative data were expressed as mean ± SD for normally distributed data and median and interquartile range for data with skewed distribution. Categorical data were presented as frequency and percentage. Quantitative variables were compared by independent sample t-test for normally distributed data and the Mann-Whitney U test was used for non-parametric data. Categorical variables were compared by the Chi-square test and Fisher’s exact test. P-value <.05 was considered as significant.
Results
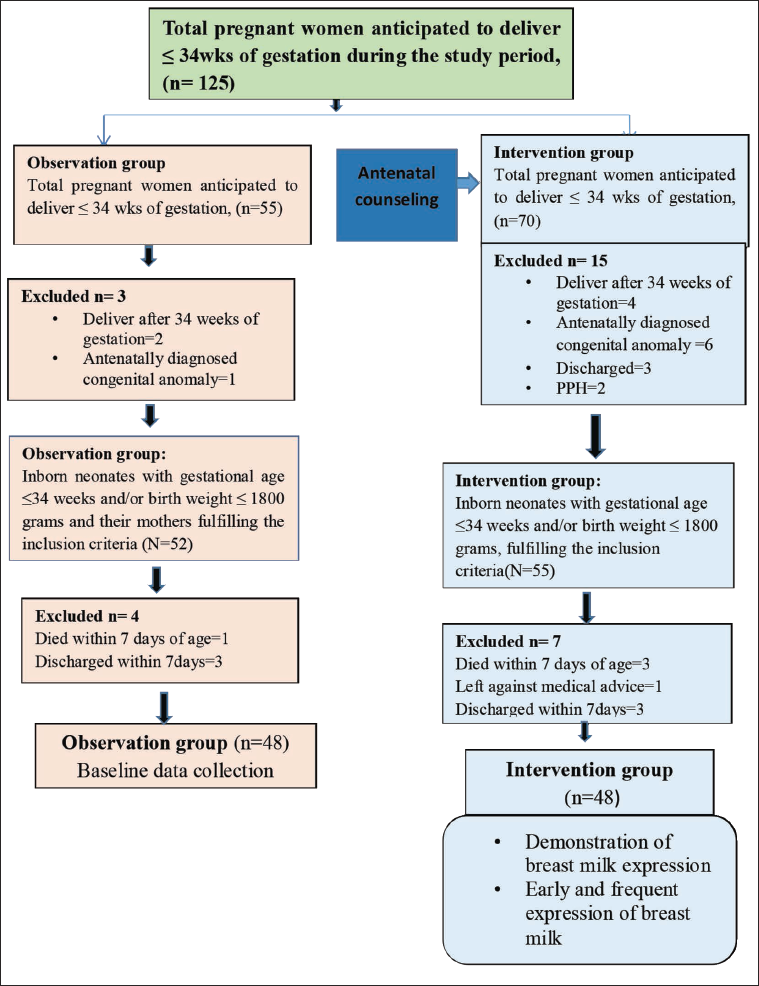
Patient enrolment process is shown in figure 3. A total of 125 pregnant women were anticipated to deliver ≤34 weeks of gestation during the study period. During the observation phase, 55 pregnant women were anticipated to deliver ≤34 weeks of gestation. Among them, 3 pregnant women were excluded due to delivery after 34 weeks of gestation and antenatally diagnosed congenital anomalies. In total, 52 preterm neonates ≤34 weeks and/or birth weight ≤1800 g and their mothers were included in the observation group. Among 52 preterm newborns, 4 were excluded during the study period due to death and discharge within 7 days. Finally, 48 preterm neonates ≤34 weeks and/or birth weight ≤ 1800 g and mother dyads were included in the observation group. During the intervention phase, 70 pregnant women were anticipated to deliver ≤34 weeks of gestation. Among them, 15 pregnant women were excluded. After delivery, 55 preterm neonates with gestational age ≤34 weeks and/or birth weight ≤1800 g and their mothers were included in the study. Among the 55 newborns, 7 were excluded during the study period due to death, discharge, and left against medical advice within 7 days. Ultimately, 48 neonates with gestational age ≤34 weeks and/or birth weight ≤ 1800 g and mother dyads were included in the intervention group.
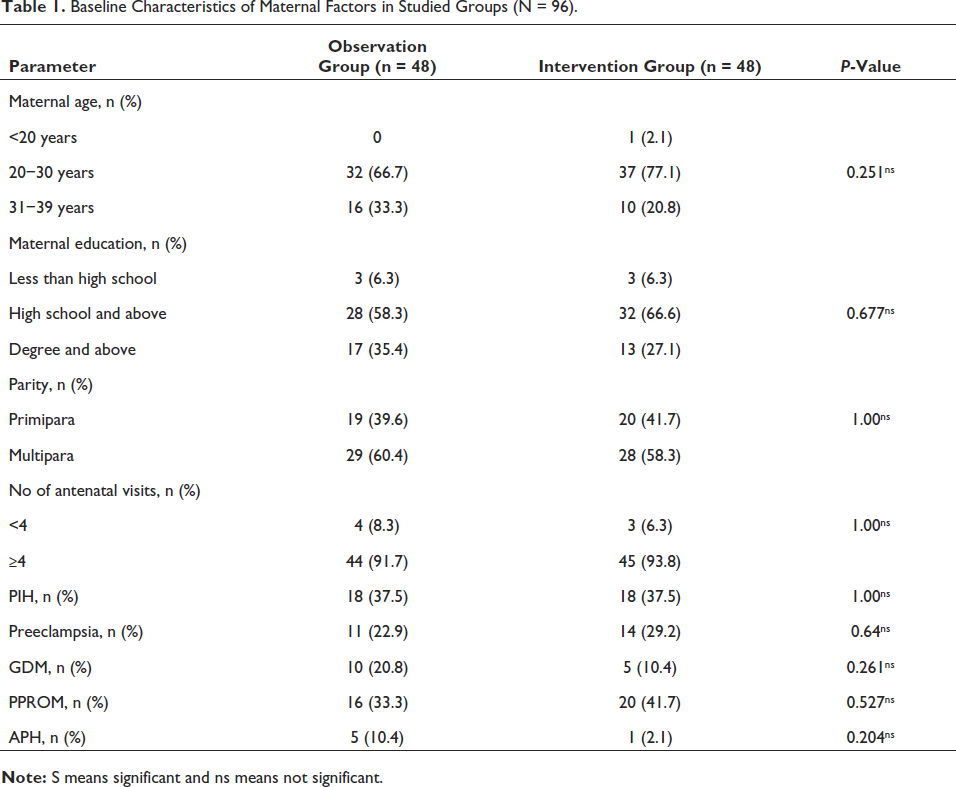
General characteristics of mothers were shown in Table 1. Baseline characteristics were comparable between the two groups.
Baseline Characteristics of Maternal Factors in Studied Groups (N = 96).
General characteristics of newborns were shown in Table 2. Mean gestational age, fetal growth, and birth weight were comparable between the two groups. Gender distribution reflected slight female predominance in the observation group.
Baseline Characteristics of Neonates in Studied Groups (N = 96).
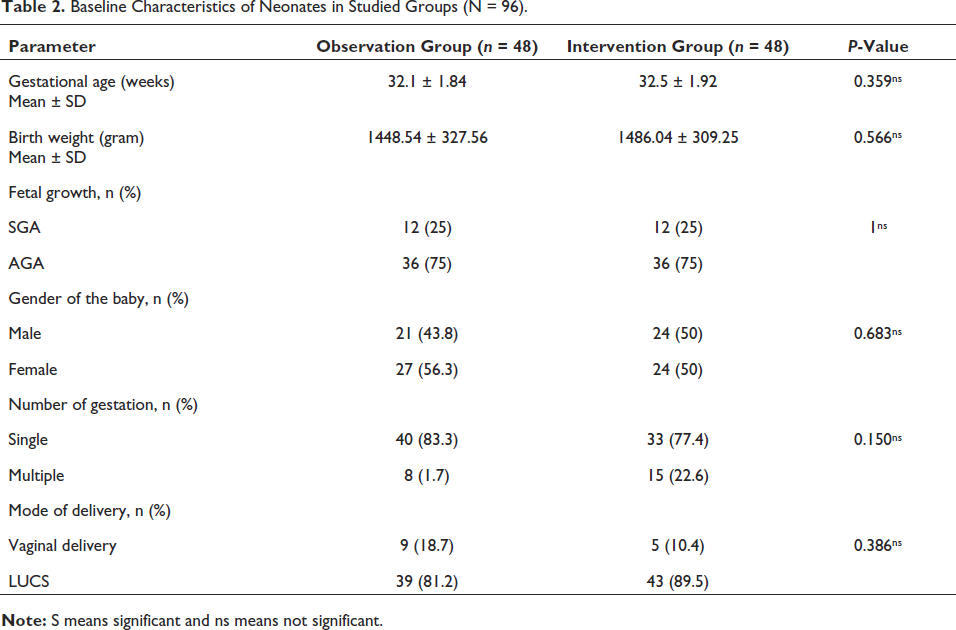
Table 3 shows that there was a statistically significant difference seen on the result of breast milk expression within 6hrs of birth and on day 1 between the two groups. Mothers in the observation group did not express breast milk within 6 h of birth, whereas all mothers expressed breast milk within 6 h of birth in the intervention group. In the observation group, 7 (14.5%) mothers expressed breast milk on day 1, but all mothers expressed breast milk on day 1 in the intervention group. There was no statistically significant difference seen in the result of breast milk expression on day 3 and day 7.
Comparison of Expression of Breast Milk Among Mothers within 6 h of Birth, Day 1, Day 3, and Day 7 Between the Two Groups (N = 96).
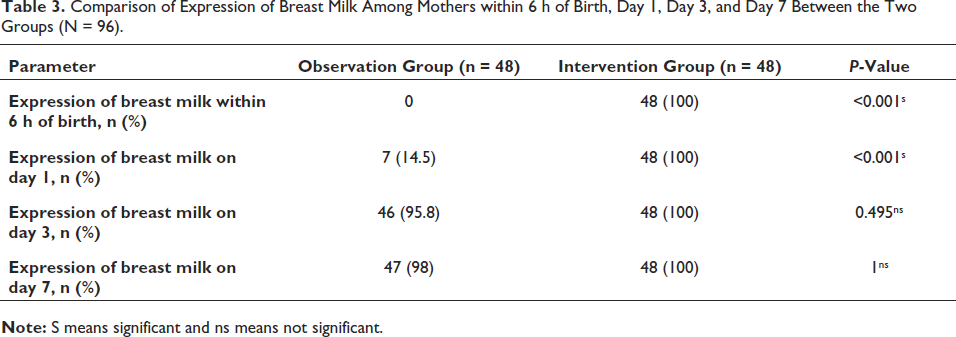
Table 4 shows that the amount of expressed breast milk on day 1, day 3, and day 7 in the intervention group was significantly higher than that in the observation group. The amount of expressed breast milk on day 1 increased from a median of 0 mL to 7 mL in the intervention phase. The amount of expressed breast milk increased from a median of 10 mL to 101.75 mL and 60 mL to 475 mL on day 3 and day 7, respectively.
Comparison of Amount of Expressed Breast Milk on Day 1, Day 3, and Day 7 Between the Two Groups (N = 96).
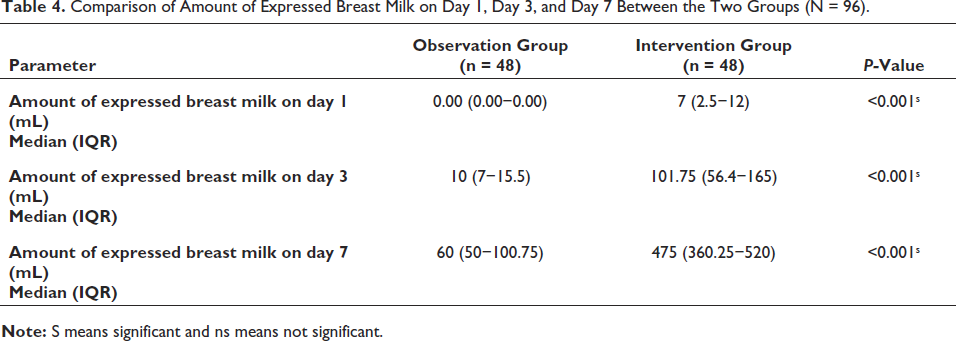
Table 5 compares the newborns fed on only mother’s own milk (MOM) on day 1, day 3, and day 7 between the two groups. The percentage of newborns fed on only mother’s own milk on day 1 increased from 14.6% to 100% which was statistically significant. However, the percentage of neonates on exclusive mother’s own milk on day 3 and day 7 did not show a significant difference between the two groups.
Comparison of Newborns Fed on Only Mother’s Own Milk on Day 1, Day 3, and Day 7 Between the Two Groups (N = 96).
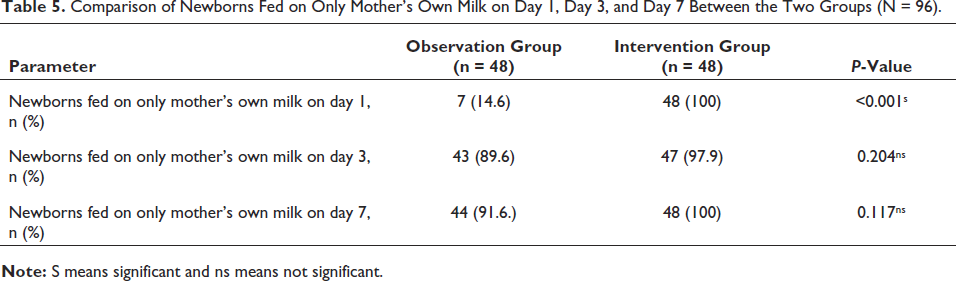
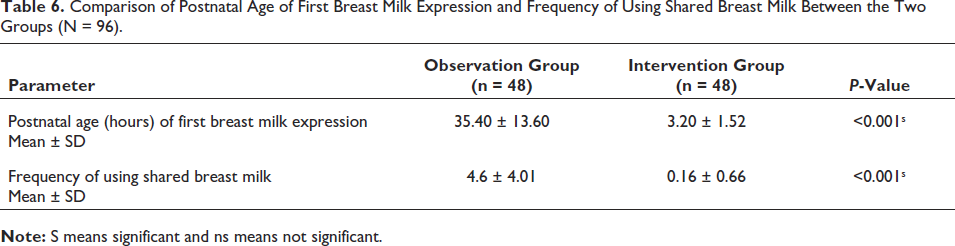
Table 6 shows that the mean postnatal age of first breast milk expression decreased from (35.40 ± 13.60) hours in the observation group to (3.20 ± 1.52) hours in the intervention group, which was statistically significant. The use of shared milk (term and mostly transitional milk) over a period of 7 days was significantly decreased in the intervention group, and it was higher (4.6 ± 4.01 times) in the observation group, whereas it was (0.16 ± 0.66times) in the intervention group.
Comparison of Postnatal Age of First Breast Milk Expression and Frequency of Using Shared Breast Milk Between the Two Groups (N = 96).
Discussion
This quality improvement study was done to increase the supply of mothers’ own milk for preterm babies admitted in the NICU, BSMMU, over a period of 12 months. Similar quality improvement initiatives to increase early milk expression in mothers of preterm babies have been published previously. They compare the use of mother’s own milk with formula milk and decrease the use of formula milk by 50%. 15 Some studies compare the use of mother’s own milk with donor human milk which showed a decreased incidence of LONS, NEC, and a shorter duration of hospital stay in preterm neonates fed on mother’s own milk. 16 But in our center, we neither have the provision of using formula milk nor have a human milk bank. That’s why mothers rely on shared breast milk most of the time due to inadequate milk volume.
Hence, the goal of this study was to increase the amount of mother’s own milk for preterm babies and decrease the use of shared breast milk, which was most of the time term and mature breast milk and did not contain the same amount of nutrients and immune factors as that of premature breast milk. A previous study showed that babies discharged on mother’s own milk improved significantly from 48.3% in the observation group to 77.4% in the continuation phase. The number of babies receiving total parenteral nutrition decreased significantly from 54.6% to 26.7% with the quality improvement initiative. 17
This quality improvement initiative demonstrated that structured counseling and demonstration of breast milk expression helped to increase the early and frequent milk expression in mothers and hence increase the exclusive mother’s own milk feeding in preterm babies.
“Liquid Gold (LG) lactation care bundle” resulted in a significant surge of breastfeeding initiation in African-American mothers (30% in Baseline to 78% in LG group). There was an increasing trend of mother’s own milk exclusivity at discharge over time. 18
During the observation phase, we found some root causes responsible for delayed milk expression and poor milk volume in mothers of preterm babies. Previous studies also found the same root causes like lack of antenatal counseling and demonstration of breast milk expression and also delayed (sometimes no milk up to the first 24–48 h) and less-frequent (2–3 times a day) breast milk expression.15, 19, 20
Evidence suggests that both health care professionals and peer support for mothers contribute to the success of breastfeeding in babies.21, 22 The literature also proposes a positive effect of education and lactation support on maternal decision to provide exclusive mother’s own milk for very low-birth-weight infants.23–26 We have counseled all the mothers of the intervention group from the antenatal period regarding early and frequent breast milk expression, the difference between term and preterm milk, and the benefit of mother’s own milk for preterm low-birth-weight babies, and lactation support was given after delivery. Counseling was also done in the postpartum period to encourage mothers for milk expression and maintenance of lactation. A previous study by Nitasha Bagga and her team showed that 60% of the mothers received antenatal counseling in the intervention phase. Antenatal counseling did not make an impact on the expression or quantity of milk on days 1, 3, and 7. 19 The reasons could be the small sample size and the short duration of the study, which were the limitations of that study. On the other hand, in our study, there was an impact of antenatal counseling on expression and quantity of milk on days 1, 3, and 7. This is because of receiving antenatal counseling by all mothers of the intervention group and they were sensitized from the antenatal period. In this study, all mothers expressed breast milk within 6 h of birth irrespective of the age of initiation of feed in the intervention group, whereas none of the mothers expressed breast milk within 6hrs of birth in the observation group. This result is consistent with that of a previous study done by Amanpreet Sethi and his team. 15 In another study, the first milk expression (≤6 h) was observed in 83.3% of cases after the implementation of the quality improvement initiative. 19 First milk expression ≤6 h after birth was improved from an average of 24% before the ‟Wee Pump” campaign to 41% afterward. 27 Most of the studies preferred 6hrs within birth for first breast milk expression because of more availability of mothers in a stable and awake state after delivery as most of the babies are delivered prematurely by LUCS because of maternal complications.18–20, 27 Mothers started to express breast milk within 3hrs of birth in a study done by Sethi et al. in 2017. 15
In our study, during the intervention phase, all mothers expressed breast milk on day 1 in comparison with the observation phase where only 14.5% of mothers expressed breast milk on day 1. In a study, all mothers expressed milk within 24 h of age in the study group. 19 Another QI study done by Sethi et al. showed that 12.5% and 86.6% of mothers expressed breast milk on day 1 in the observation and intervention phases, respectively. 15
In our study, during the observation phase, 95.8% and 98% of mothers expressed breast milk on day 3 and day 7, respectively, in comparison with the intervention phase where 100% of mothers expressed breast milk on day 3 and day 7. In a study, on day 3, 25% of mothers expressed breast milk in the observation phase whereas 100% of mothers expressed breast milk in the intervention phase. 15 This difference in the observation phase from their study is due to the use of formula milk in their unit. They were able to decrease the requirement of formula milk by almost 50% after the first week of the intervention phase.
In our study, the amount of expressed breast milk on day 1, day 3, and day 7 was significantly higher in the intervention group. Similar findings were found in a quality improvement study by Sethi et al. and Bagga et al.15, 19
During the observation phase in our study, on day 1, only 14.5% of preterm babies were on mother’s own milk which increased to 100% in the intervention phase, which is consistent with a study done by Bagga et al. 19 The proportion of neonates who received mother’s own milk within first 24 h improved from 24% in retrospective controls to 82.9% in the initiation phase. 17 In a study before the implementation of any comprehensive communication bundles, the percentage of VLBW neonates received mother’s own milk as the first feed was 19%, and after intervention, this improved to 91.3%. 12
In our study, percentage of newborns fed on only mother’s own milk on day 3 was 89.6% in the observation group and 97.9% in the intervention group, and on day 7, it was 91.6% in the observation group and 100% in the intervention group, which was not statistically significant. Another study showed a significant difference on days 3 and 7. 28
In our study, mean postnatal age (hours) of first breast milk expression decreased from 35 to 3 h after implementing the quality improvement initiative. This result is consistent with a study done by Sethi et al., which showed that the mean postnatal age (hrs) of first breast milk expression was 3 h in the intervention phase whereas in the observation phase, it was 24 to 48 h. 15 Another study showed that the median time of first milk expression decreased from 9 to 6 h after the implementation of the quality improvement initiative. 29
The quality improvement study done in our NICU suggests that a comprehensive counseling package aids in the early and frequent expression of breast milk and increases the amount of mother’s own milk, thereby increasing the supply of mother’s own milk for the preterm baby admitted in the NICU. The strength of the study is that this QI initiative can be implemented at any NICU without changing the infrastructure and human resources.
Limitations
Two hourly expression of breast milk could not be strictly maintained.
Breast milk expression could not be strictly supervised at night.
We could have evaluated the sustainability of the use of mother’s own milk till discharge.
If we had used a hospital-grade electronic breast pump instead of a manual breast pump, it would have been more effective in maintaining lactation.
Conclusion
This quality improvement initiative has made a significant improvement in the early expression of breast milk, an increase in the total amount of expressed breast milk, and an exclusive mother’s own milk feeding among the preterm neonates admitted in the neonatal intensive care unit.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
As per international standard or university standard, written ethical approval has been collected and preserved by the author(s).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.