
Abstract
Background
Though early enteral nutrition with Mother’s own milk (MOM) is the norm in preterms, it is a difficult challenge to get it into the intensive care unit due to various medical and logistic issues. Awareness about this among pregnant ladies and their caregivers from the antenatal period may help to overcome some of these difficulties.
Objective
To compare the effect of the implementation of an antenatal breast milk care bundle on the availability of adequate breast milk on day 7 for preterm babies ≤ 32 weeks when compared to a postnatal breast milk care bundle alone.
Methodology
This prospective study was conducted among neonates ≤32 weeks born in Government Medical College, Thiruvananthapuram from January 2021 to May 2022. Antenatal bundles were implemented in the antenatal OPDs and wards. Postnatal bundles were implemented in the NICU and postnatal wards. The outcome was compared among babies of mothers who got both the care bundles and those who received only the postnatal care bundle.
Results
A total of 110 babies were included in the study. There was a 1.32 times increase in the adequacy of milk volume on day 7 (CI: 1.04–1.68), a significant increase in the proportion of mothers expressing within 24 hours, and babies getting discharged on exclusive MOM in those who received the antenatal BMC bundles. The risk for inadequate milk volume was high in those who have <2 ml of milk at 48 hours (RR: 1.67, CI:1.26–2.20].
Conclusion
Antenatal breast milk care bundles can increase the availability of adequate MOM for preterm babies.
Introduction
With improving neonatal care, the survival of preterm neonates has improved significantly in the recent past. Providing optimum nutrition to a high-risk premature neonate is a difficult challenge. Mother’s own milk (MOM) is the preferred enteral feeding for these newborns. It helps in faster gastric emptying, less feed intolerance, and fewer days to achieve full feeds than preterm formula feeds. MOM also reduces the risk of Necrotising Enterocolitis (NEC), late-onset sepsis, and bronchopulmonary dysplasia (BPD).1, 2 But, insufficient supply of MOM in the early days of life will hinder the early initiation of enteral nutrition for these premature infants. Logistic issues are more in the public sector for obtaining expressed breast milk to the NICU at the appropriate time. The lack of awareness among the caretakers and the mother herself about the need for early expressed breast milk for the preterm baby, the separation of mother and baby, poor lactogenesis in preterm mothers, logistic difficulties for early expression, restriction in the number of caretakers in the public sector, etc., are some of the reasons. Its impact is more in the public sector dealing with a large volume of patients. Human milk banks are not available everywhere. Most of the time, it is impossible to start enteral nutrition on day 1 or 2. Counselling and other supportive measures from the antenatal period may help to overcome these logistic issues and also positively influence the mental comfort of the mother. Hence, this study was undertaken to compare the effect of the implementation of an antenatal breast milk care bundle on the adequacy and availability of breast milk for preterm babies.
Methodology
This prospective cohort study was done in the inborn neonatal intensive care unit (NICU), obstetric wards, and Outpatient Department of the Obstetrics and Gynaecology of our institution from 16 January 2021 to 30 May 2022 after getting clearance from the Human Ethics Committee. A consecutive sampling of all eligible preterm babies ≤32 weeks was done on day 7 of life after obtaining informed consent from the parent or the legally authorized representative till the sample size was met. Babies <25 weeks, babies having lethal anomalies, babies of mothers who were critically ill, unbooked mothers, and mothers <18 years were excluded.
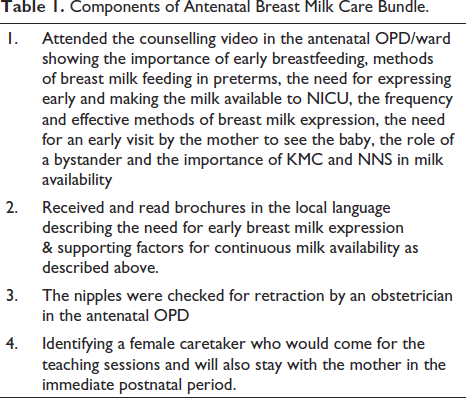
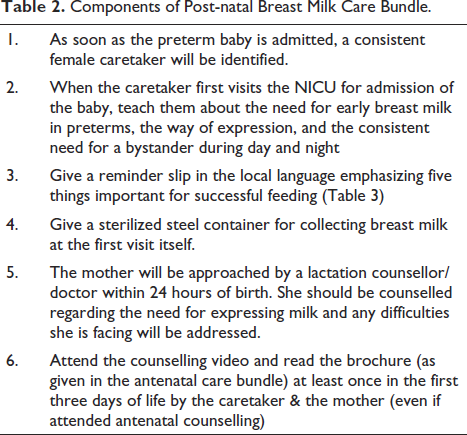
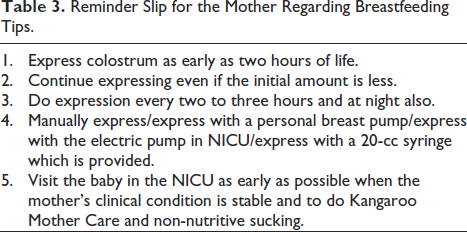
As a part of the study ‘Breast milk care bundles’ (BMC bundles) were formulated. It included an ‘antenatal breast milk care bundle’ and a ‘postnatal breast milk care bundle’ as given in Tables 1 and 2. Antenatal BMC bundles were given to all the antenatal patients above 24 weeks gestation and their caretakers attending the obstetrics outpatient department and to those who were admitted to wards. Special emphasis was given to those who were anticipating preterm delivery. Counselling was done by the principal investigator or the lactation counsellor or the residents posted in the antenatal wards and obstetrics OPD on all days on a rotatory basis. Regular postnatal BMC bundles were given to all mothers of preterm babies irrespective of whether they have received antenatal care bundles. The mothers who were booked antenatally in the study center received both antenatal and postnatal BMC bundles (full intervention group) but those who were booked outside and referred at the time of delivery received only postnatal BMC bundles (partial intervention group) (Table 3).
Components of Antenatal Breast Milk Care Bundle.
Components of Post-natal Breast Milk Care Bundle.
Reminder Slip for the Mother Regarding Breastfeeding Tips.
The major outcomes measured were milk volume in milliliters expressed at 48 hours post-delivery and the average volume of breast milk per session on day 7. For babies ≤32 weeks with an approximate birth weight of 1.25 kg, at least 20 ml breast milk per session will be required for an adequate intake of 150–200 ml/kg/day. Hence adequacy of MOM on day 7 was taken as at least 20 ml per session.3, 4 Exclusive breastfeeding status was also assessed at discharge.
From a recent study by Bagga et al., the proportion of neonates ≤32 weeks receiving adequate MOM on day 7 before and after implementation of the quality improvement program was 46.7% and 73.3%, respectively. 5 The sample size calculated from the formula
{(Z1 – α/2 + Z1 – β) 2 (P1 Q1 + P2 Q2)} / (P1 – P2) 2 with an α error of 5%, a power of 80% and an expected attrition of 10% was 58 in each group.
Statistical Analysis
The analysis was done in SPSS version 26. The continuous variables were expressed as mean with standard deviation or as median & and IQR according to the normality of the data. Categorical data were summarized as frequencies and percentages. Association between continuous variables was done by Mann Whitney U-test. The outcome was analyzed as both a continuous and categorical variable. Univariate analysis was done by the chi-square test and the strength of association was calculated by relative risk and its 95% confidence interval. Logistic regression was done to adjust for confounders affecting the adequacy of breast milk.
Results
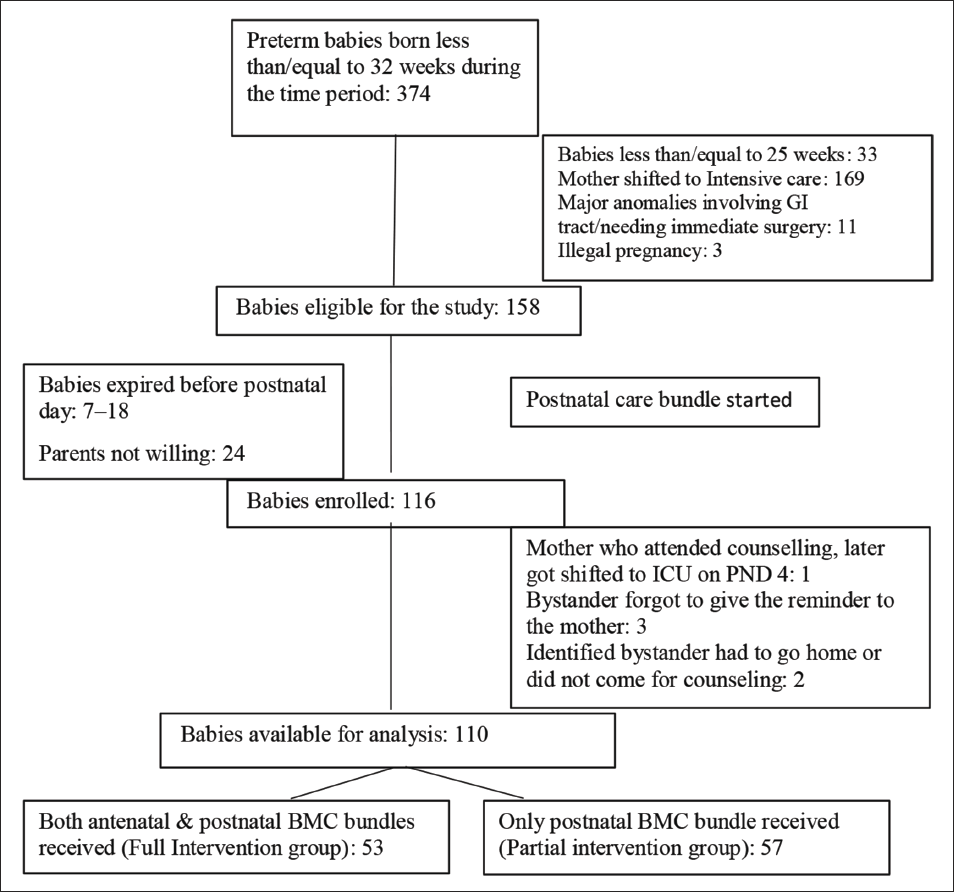
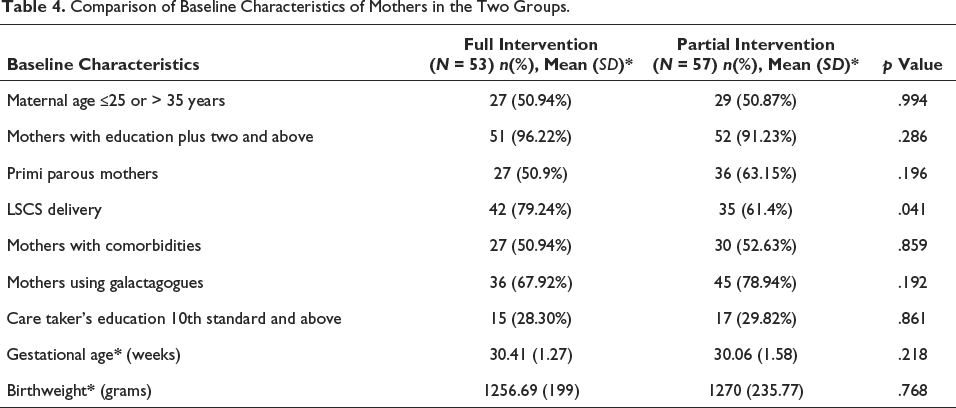
Among 116 babies who were included in the study, 110 babies were available for analysis with 53 babies in the full intervention group and 57 in the partial intervention group as shown in Figure 1. The mean gestational age of our study cohort was 30.2 (1.4) weeks. The mean birth weight was 1263.59 (218.02) grams. Primi mothers constituted 57.3% and the mode of delivery was by LSCS in 70%. Mothers who were educated above class twelve were 93.6%. Maternal age was below 25 years in 48.18% and only 2.7% were above 35 years. Comorbid conditions were present in 51.8% of mothers. The two groups were comparable in the basic characteristics except for the mode of delivery as shown in Table 4.
Study Flow Chart.
Comparison of Baseline Characteristics of Mothers in the Two Groups.
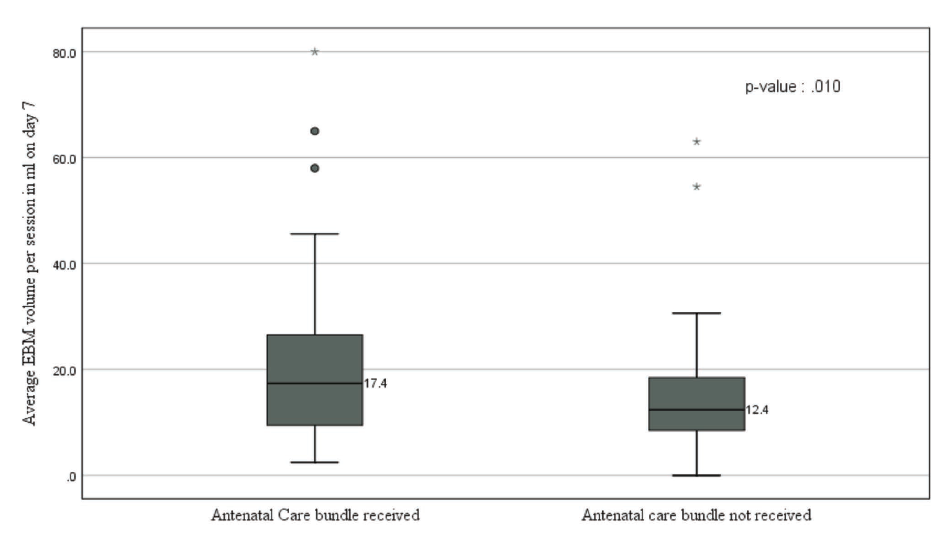
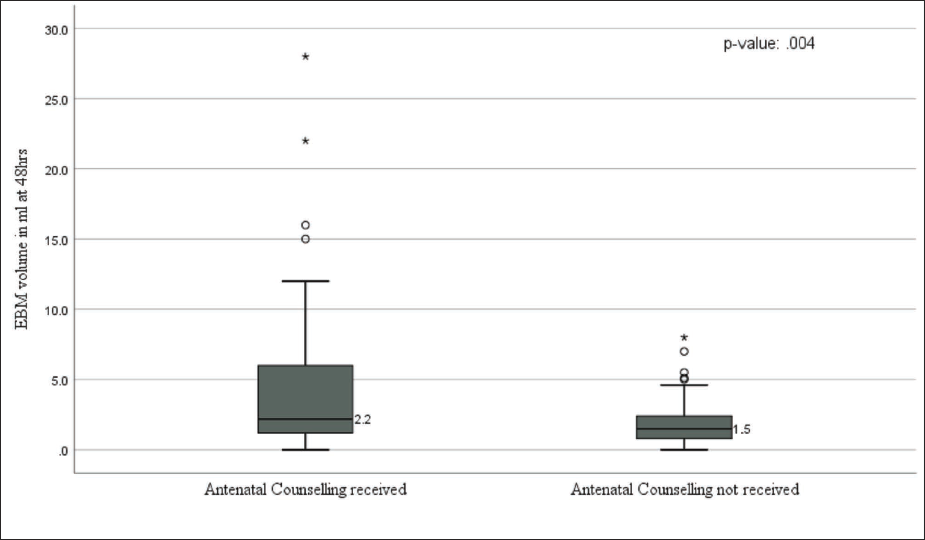
The average milk volume per session on day 7 and the milk volume at 48 hours of life in the full intervention and the partial intervention group was as given in Figures 2 and 3. The median value of MOM per session on day 7 was 17.4 ml (IQR 18) in the full intervention group and 12.4 ml (IQR 10) in the partial intervention group. Milk Volume at 48 hours had a median value of 2.2 ml (5.85) in the full intervention and 1.5 (1.7) ml in the partial intervention group. These differences were statistically significant.
Box and Whisker Plot Depicting MOM Volume per Session on Day 7 in both Groups.
Box and Whisker Plot Depicting Expressed Breast Milk Volume at 48 Hours in both Groups.
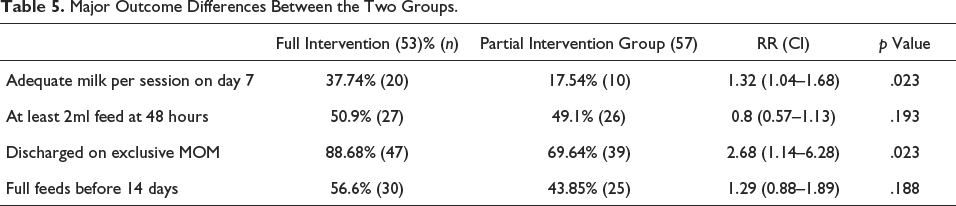
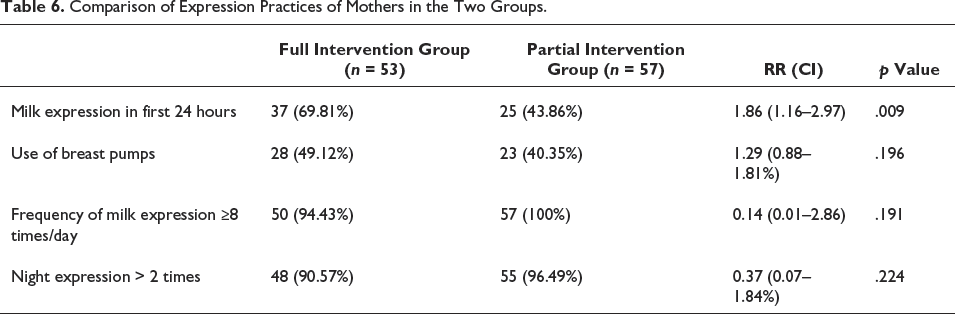
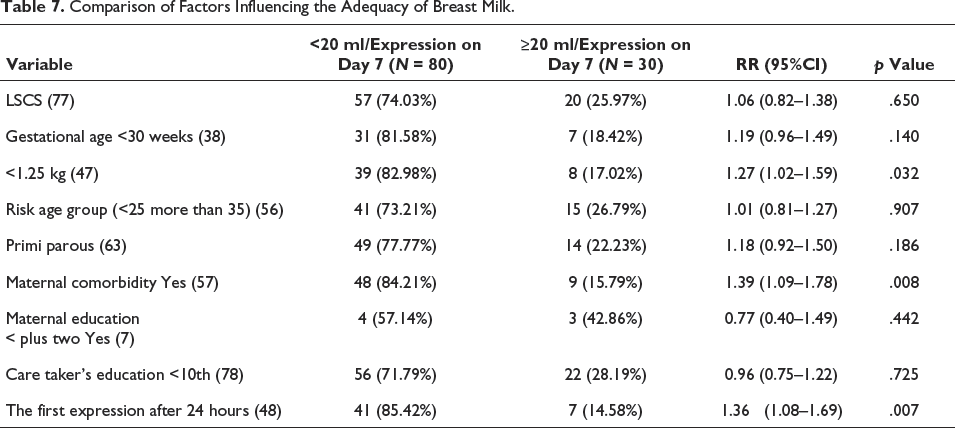
Other major outcomes in the two groups were as shown in Table 5. The full intervention group had a statistically significant increase in the proportion of babies having adequate milk per session on day 7. Also, there was a statistically significant increase in the proportion of babies discharged on exclusive breast milk in the full intervention group. However, there was no increase in the proportion of babies having at least 2 ml of milk at 48 hours of life. The milk expression practices of mothers in the two groups were as in Table 6. Mothers who received the full intervention had a 1.86 times higher chance of getting milk expressed in the first 24 hours. Analysis of other factors affecting the adequacy of breast milk is given in Table 7. Birth weight <1.25 kg (RR: 1.27, CI: 1.02–1.59), maternal comorbidities (RR: 1.39, CI: 1.09–1.78), and time of first milk expression after 24 hours (RR: 1.36, CI: 1.08–1.69) were having significant associations for inadequate milk availability.
Major Outcome Differences Between the Two Groups.
Comparison of Expression Practices of Mothers in the Two Groups.
Comparison of Factors Influencing the Adequacy of Breast Milk.
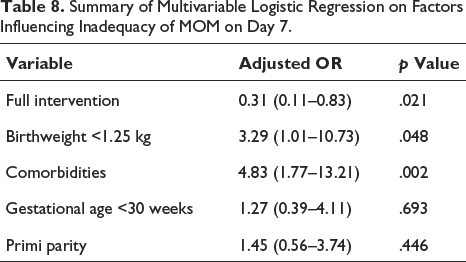
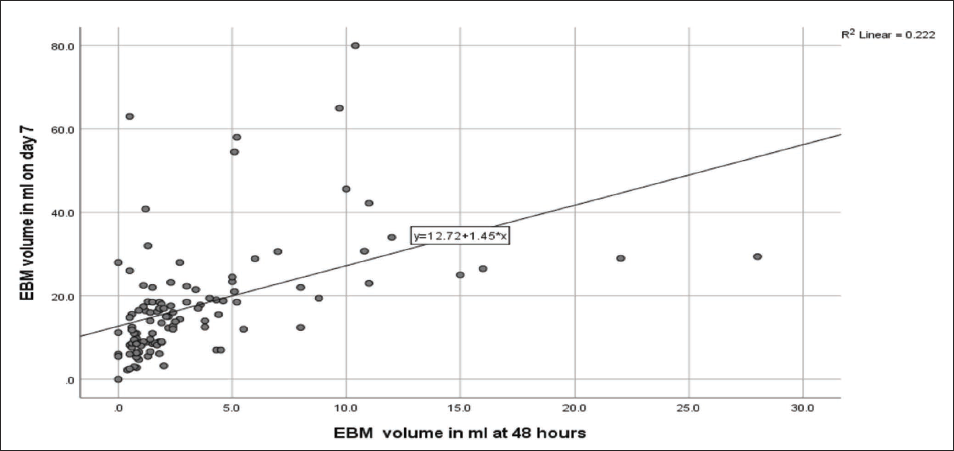
For adjusting the confounding factors associated with inadequate milk volume on day 7, logistic regression was done by the Enter method. We chose the factors based on scientific literature and our univariate analysis (p value < .2) for putting into the logistic regression. The timing of the first expression was not taken as it was influenced by our intervention. The benefit of antenatal BMC bundles on the availability of adequate milk volume on day 7 persisted even after multivariable binary logistic regression (Table 8) (adj. OR for inadequate milk 0.31, CI: 0.11–0.83, p value: .021). Birth weight <1.25 kg (adj. OR: 3.29, CI: 1.01–10.73) and maternal comorbidities (adj. OR: 4.83, CI: 1.77–13.21) were the other significant factors relating to the inadequate availability of milk. On multiple linear regression, it was found that antenatal intervention alone increased an average of 6.28 ml of MOM per session on day 7. However, there was only a moderate correlation between milk volume at 48 hours and the volume of milk on day 7 as shown in Figure 4 (Spearman’s rho 0.603).
Summary of Multivariable Logistic Regression on Factors Influencing Inadequacy of MOM on Day 7.
Scatter Diagram Showing the Correlation of MOM Volume at 48 Hours and MOM per Session on Day 7.
Discussion
Out of the 110 babies who were available for analysis 53 babies belonged to mothers who had received both antenatal and postnatal BMC bundles whereas 57 babies belonged to mothers who received only postnatal BMC bundles. From a recent review, daily pumped milk volume in the first week is a predictor of continuing exclusive breastfeeding at discharge. 6 In this study, there was a median increase of 5 ml of milk per session on day 7 in the group of mothers who received the full intervention, which will come to an extra milk volume of 50–60 ml per day. By linear regression also it was shown that antenatal BMC bundles alone increased 6.8 ml of MOM per session on day 7. In this study, there was a median increase of 0.7 ml of milk at 48 hours of life in the full intervention group. This difference was statistically significant. The clinical impact may not be significant in babies with higher birth weights but surely can support an ELBW baby.
In studies by Dong et al. and X Ru et al., the volume cut-off per session for the onset of lactogenesis II was 20 ml.3, 4 Logically this is reasonable on day 7 because, if a 1.25 kg baby achieves full feeds on day 7, 18–20 ml per session will be enough for feeding at a rate of 150–200 ml/kg/day. So, when taking a cut-off of 20 ml per session on day 7, those who have received antenatal BMC bundles had a 1.32 times higher chance of getting adequate milk volume on day 7 (RR: 1.32, CI: 1.04–1.69, p value .023) compared to the other group and this protective effect was persisting even after adjusting for the other factors as shown in the logistic regression. In a study by Bagga et al., antenatal interventions did not make an impact on the expression or quantity of milk on days 1, 3, and 7 and there are not many studies in the published literature on the influence of milk volume on day 7 by antenatal interventions. 5
In this study, when compared to other studies in this area, the antenatal BMC bundle had an additional factor of early identification of a female caretaker. She was counselled regarding the need for early and frequent expressions for establishing feeding in a preterm baby and was also asked to stay with the mother after delivery. This might have made a positive result in making milk available at the bedside in a government setting.
In this study, a birth weight <1.25 kg was associated with inadequate milk volume on day 7 (RR: 1.27, CI: 1.02–1.59) and the association persisted after adjusting for the confounders (adj. OR: 3.29, CI: 1.01–10.73). Any one of the comorbid conditions (PIH, GDM, hypothyroidism, acute fatty liver of pregnancy, SLE) in the mother was associated with a higher risk for the inadequate volume of milk on day 7 (RR: 1.39, CI: 1.09–1.78) and it was also persisting even after adjusting for the possible confounders (adj. OR: 4.83, CI: 1.77–13.21). So special attention to counselling regarding breastmilk should be given to this high-risk group. Other factors like maternal age, type of delivery, parity, and education of parents or bystanders did not affect the available volume of milk on day 7.
On analyzing the breastmilk-promoting practices in this cohort, there was a significant increase in the expression rate within the first 24 hours in the full intervention group (69.81%) compared to mothers who received only partial intervention (43.86%). Overall, 56.4% of mothers expressed breast milk within 24 hours, and only three mothers (2.7%) expressed it within six hours of birth. Even among mothers who were antenatally counseled, 30% did not express it in the first 24 hours. This might be due to various logistic issues in a government hospital. Delays in shifting mothers from the delivery room and operation theatres due to maternal complications, the absence of dedicated staff to help mothers in expression, non-availability of lactation counsellors round the clock, caretakers not being allowed inside the delivery room, long distances between maternal wards and NICU, etc., might have caused this delay in expression. In this study, though antenatal BMC bundles had an effect on early expression rates it had no effect on breast pump use, number of expressions per day, and night expressions.
In the whole study cohort, 78.18% of the babies were discharged on MOM which was higher when compared to other studies.7, 8 There was a statistically significant increase in the rate of exclusive breastfeeding at discharge in those who received antenatal BMC bundles (89% vs. 70%).
This was a prospective study and could meet the sample size adequately. We have included only those mothers who received full components of the bundles to avoid bias in the comparison of performance and both groups were comparable. However, we could not include BMI, socioeconomic status, and diet of the mother in our study. We tried to find out the availability of breastmilk at the bedside in the NICU by our interventions but could not differentiate whether non-availability was due to inadequate breastmilk in the mother or logistic issues in bringing the milk to the NICU.
Conclusion
A breast milk care bundle beginning from the antenatal period could significantly increase the availability of adequate breast milk on day 7, exclusive breastfeeding rates at discharge, and rates of milk expression in the first 24 hours compared to a postnatal breast milk care bundle alone. Hence, antenatal breast milk care bundles including the identification of a dedicated female caretaker should be a routine from 24 weeks of gestation. Maternal comorbidities and birth weight less than 1250 grams were the other significant risk factors reducing the adequacy of feed volume on day 7. But even with antenatal care bundles, only 37.74% of babies received adequate feed volume on day 7, only 70% of mothers expressed milk within the first 24 hours, and only 50% received at least 2 ml of milk at 48 hours. These areas need further attention.
Footnotes
Acknowledgment
We sincerely thank the senior residents in neonatology Dr. Anupama S Pillai and Dr. Shabin J for their whole hearted support for our study.
Contributions by Each Author
All five authors have contributed to the concept and design of the work, analysis, and interpretation of data, drafting of the article, and approval of the version to be published. The first author has done the acquisition of the data. Each author has participated sufficiently in the work to the public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration of Patient Consent
We authors certify that we have obtained all appropriate patient consent forms. The parents understood that their baby’s name will not be published and due efforts will be made to conceal their identity.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Human Ethics Committee, Medical College, Thiruvananthapuram.
Permission Number: HEC. No.01/14/2021/MCT dated 15 January 2021.
Supplemental material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.