
Abstract
Congenital hepatic arteriovenous malformations (AVM) are extremely rare, with an incidence of less than 1 in 1 hundred thousand, and the literature is limited to only a few case reports. They are characterised by an abnormal arterial connection to a fistulous venous connection within the liver. This results in high flow, low resistance circulation that causes high output cardiac failure. We report a late-preterm male newborn who presented with respiratory distress and signs of cardiac failure on day 1 of life. The newborn is diagnosed with hepatic AVM as the cause of severe pulmonary arterial hypertension (PAH) and cardiac failure. This case report, along with the literature review, emphasises the need for a high index of suspicion to look for hepatic AVM in a newborn presenting with unexplained PAH and cardiac failure and also discusses different management strategies for hepatic AVM.
Keywords
Abbreviations
AVM: Arteriovenous malformation
PAH: Pulmonary arterial hypertension
CHF: Congestive heart failure
PPHN: Persistent pulmonary hypertension
RDS: Respiratory distress syndrome
CDH: Congenital diaphragmatic hernia
APGAR: Appearance, pulse, grimace, activity, respiration
CPAP: Continuous positive airway pressure
NICU: Neonatal intensive care unit
SVC: Superior vena cava
IVC: Inferior vena cava
Introduction
Pulmonary arterial hypertension (PAH) in the newborn is most often secondary to pulmonary pathology (meconium aspiration syndrome, respiratory distress syndrome (RDS), pneumonia, congenital diaphragmatic hernia (CDH) and congenital lung hypoplasia), sepsis, asphyxia, or congenital cardiac defects; hence, a rare cause like hepatic arteriovenous malformation (AVM) is often undiagnosed, resulting in morbidity and mortality. A large hepatic AVM usually presents as high-output cardiac failure or severe PAH.
Case Report
A late-preterm (36 weeks), 2.7 kg male baby was born by normal vaginal delivery with a normal appearance, pulse, grimace, activity, respiration (APGAR). The baby was referred to our hospital at 8 h of life because of progressive respiratory distress. On examination, the baby had tachypnoea (RR: 68/min) with increased work of breathing and was maintaining preductal saturations of 85% and postductal saturations of 80% in room air with normal heart sounds. The liver was palpable 2 cm below the right costal margin. Chest radiography showed cardiomegaly with normal lung fields. The baby was started on continuous positive airway pressure (CPAP) support with 60% FiO2 and PEEP 6. The complete blood count and sepsis screen came back normal.
Because of cardiomegaly, echocardiography was done, which showed a moderately dilated right atrium and right ventricle with severe PAH, right ventricular systolic pressure (RVSP) (from tricuspid regurgitation (TR) jet) – 60 mmHg), time to peak velocity (TPV) – 50 ms (TPV: right ventricular ejection time (RVET) = 0.2, with a D-shaped left ventricle), and an ejection fraction of 60% with a structurally normal heart.
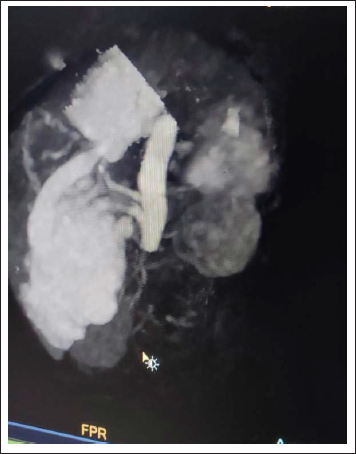
As the lung fields showed optimal recruitment and the sepsis workup came back negative, further investigations were done to find out the cause of the unexplained severe PAH. A neurosonogram was done, and a vein of Galen malformation was ruled out. Bedside ultrasound of the abdomen showed hepatomegaly with multiple vascular-rich cystic masses in the right lobe of the liver with arterial and venous supply. A provisional diagnosis of hepatic AVM, or haemangioendothelioma, was made. At around 30 h of life, the baby had increased work of breathing on CPAP, and because of impending respiratory failure, the baby was electively ventilated. Signs of PAH worsened with an increase in ventilator requirements. The baby was started on intravenous furosemide for flow-related PAH. Arterial blood gas showed an increase in lactate (4.5), with repeat 2Decho showing mild LV dysfunction (FS 25%); hence, milrinone infusion was started at 0.3 µg/kg/min once the baby was haemodynamically stable. Serial functional echocardiography was done for the assessment of ejection fraction and PAH. An MRI of the abdomen and CT angiography were done, which showed a large encapsulated mass lesion involving the posterior segment of the right lobe of the liver with large internal flow voids and arterialised veins and venous channels. Features were in favour of high-flow AVMs with AV fistulas and shunts. Other less likely possibilities were infantile hepatic haemangiomas or vascular neoplasms like haemangioendotheliomas.
Hence, a diagnosis of high-flow hepatic AVM was made, and definite treatment for the same was considered. Oral propranolol and steroids were considered as possible underlying haemangioendothelioma of the liver. By day 3 of life, a repeat sepsis screen showed elevated procalcitonin and a positive CRP. Hence, steroids were not started. Oral propranolol was started at 1 mg/kg/day, along with IV antibiotics. Investigations showed no evidence of haemolytic anaemia, consumptive coagulopathy, or hypo- or hyperthyroidism. By day 4 of life, the baby’s condition improved, and he was completely off the ventilator by day 7 of life. But because of persistent oxygen requirements and mild respiratory distress, definitive treatment options of radiological intervention (coiling or embolisation of feeding vessels) or surgical ligation of the feeding vessels were explained to parents. But unfortunately, because of financial constraints, the parents decided to withdraw the treatment, and we lost the baby to follow-up.
Discussion
AVMs in newborns are very rare anomalies. The incidence of congenital hepatic AVMs is less than 1 in 1 hundred thousand live births. 1 They are associated with significant morbidity and mortality (50%–90%). 2 AVM that produces symptoms in the first 6 months of life occurs primarily in the CNS, lung, and liver. Among AVMs, hepatic AVMs are much rarer. There are only a few case reports of congenital hepatic AVM in the literature. Cerebral AVM (Vein of Galen Malformation) is known to present as persistent pulmonary hypertension (PPHN) 3 and cardiac failure. There are only a few case reports of hepatic AVM presenting as PPHN. In our case, the baby had congenital hepatic AVM, which was the cause of severe PAH and right heart failure.
Congenital AVM usually presents as high-output cardiac failure (58%), with a median age of presentation of 2.2 months. 4 Other presenting features of hepatic AVM are hepatomegaly, PPHN, microangiopathic haemolytic anaemia, consumption coagulopathy, portal hypertension and hydrops fetalis. 1 Hepatic AVM is a direct arterial-to-venous connection that bypasses the normal tissue perfusion capillaries that occur in the liver. Usually, single or multiple arterial feeder vessels drain into the AVM. 1 As systolic blood pressure is higher on the arterial side, there is progressive shunting of blood into the venous side.1–3 As more blood is shunted through this low-resistance circulation, cardiac output rises, resulting in high-output cardiac failure. PPHN is associated with conditions resulting in either increased pulmonary vascular resistance or decreased pulmonary blood flow. 3 Most cases of PPHN are almost always due to elevated pulmonary vascular resistance. Only a few conditions of PPHN are due to increased pulmonary blood flow. AVM is one such condition where PPHN is caused by increased pulmonary blood flow. Other conditions causing increased pulmonary blood flow and leading to PPHN are neonatal hyperthyroidism. 3 A combination of clinical signs of heart failure and echocardiographic findings of accentuated blood flow within the superior vena cava (SVC) or inferior vena cava (IVC) in the presence of a structurally normal heart should alert one to look for an AVM in the neonate. Treatment of PPHN finally depends on the underlying pathophysiology. Pulmonary vasodilators are useful in the treatment of PPHN, which occurs because of increased pulmonary vascular resistance. The use of pulmonary vasodilators will worsen the symptoms of PPHN because of increased pulmonary blood flow. In the case of PPHN caused by AVM, treatment is medical management of cardiac failure and definitive treatment of AVM. In our case, the baby was initially stabilised with furosemide and milrinone infusions. 5
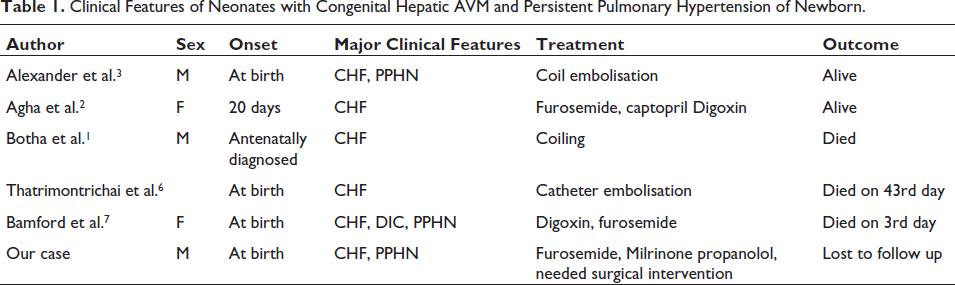
As per the literature review, to the best of our knowledge, there are published case reports of five newborns who presented with cardiac failure with features of PAH and were diagnosed to have congenital hepatic AVM. Out of the five newborns, two babies (40%) had a favourable outcome. Out of the two babies who survived, one (50%) recovered with medical management. Alexander et al. 3 reported a case of a newborn who was treated successfully with coil embolisation. Agha et al. 2 reported the case of a 20-day-old newborn who presented with cardiac failure and was treated conservatively with anti-failure medications. Botha et al. 1 reported another baby who was antenatally diagnosed and treated with coiling. Thatrimontrichai et al. 6 reported a neonate who was diagnosed at birth and was treated with catheter embolisation, but the baby succumbed to illness. Bamford et al. 7 reported a case of a newborn who was treated conservatively with anti-failure medications, but the baby succumbed to illness on day 3 of life (Table 1 and Figures 1 and 2).
Clinical Features of Neonates with Congenital Hepatic AVM and Persistent Pulmonary Hypertension of Newborn.
Chest X-Ray Showing Cardiomegaly.

CT Angiogram Showing Hepatic AVM.
The standard treatment options for congenital hepatic AVM are conservative management with anti-cardiac failure medications (furosemide, digoxin, captopril, and enalapril) in haemodynamically stable babies who do not require neonatal intensive care unit (NICU) admission. There is a case report suggesting the same. Other treatment options for hepatic AVM include surgical and radiological interventions. Surgical options are ligation or resection of the feeding vessel, partial hepatic resection or orthotopic liver transplantation.3, 4, 7 Radiological interventions available include transcatheter embolisation of the feeding vessels. But the chances of recanalisation are high if there are multiple feeding vessels. 1 Surgical resection is associated with significant risk in sick infants and babies with multiple collateral vessels. As per the available case reports, embolisation is successful and effective in AVM with a single feeding vessel.
Conclusion
Cerebral AVM (Vein of Galen malformation) is known to present as PAH and cardiac failure in newborns. There are only a few case reports of hepatic AVM presenting as PAH. In a few case reports, hepatic AVM is diagnosed incidentally in babies while being managed for PPHN. The high mortality rate (50%–90%) associated with hepatic AVM emphasises the need for a high index of suspicion for early diagnosis and definite treatment. Medical management with drugs can be tried on babies who do not require hospital admission and are haemodynamically stable. Radiological intervention with percutaneous transcatheter embolisation is less expensive, safer, and as effective as the surgical approach. However, coil embolisation appears to be most effective in treating AVMs with a single feeder arterial vessel. Finally, this case report emphasises the fact that, while evaluating a baby for severe PAH, echocardiography is incomplete without examination of the liver and brain.
Footnotes
Declaration of Conflicting Interest
The authors declare that they have no conflict of interest. This manuscript has been read and approved by all the authors.
Ethical Approval
Not Applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent is obtained from the newborn’s mother.