
Abstract
Introduction:
Adolescent students with vision impairment face additional challenges in attaining optimal mental well-being, which impacts their pursuit of education and quality of life. Their mental health condition is unknown and unaddressed in Nepal. This study aimed to determine the prevalence of depressive symptoms among adolescent students with vision impairment in public integrated schools in Nepal.
Material and Methods:
We conducted a quantitative cross-sectional study among adolescent students with blindness and low vision from four integrated schools in Nepal. Schools were purposively selected, two from Kathmandu Valley, the capital city, and two from western Nepal. Ethical approval was obtained before the study. All adolescents diagnosed with blindness and low vision were invited to participate in the study. Participation was voluntary. They were interviewed using the Depression Self-Rating Scale (DSRS) by trained enumerators. Depressive symptoms were defined to be present if the total DSRS score was greater than 14. Fisher’s exact test and odds ratios were used to assess variables linked to depressive symptoms.
Results:
Among 65 adolescent students with vision impairment, 7 (10.77%) had depressive symptoms. No significant association was found between depressive symptoms and sociodemographic variables such as gender, age, type of vision impairment, and site of the study.
Conclusion:
Adolescents with vision impairment are vulnerable to depressive symptoms in Nepal. A supportive, inclusive environment is recommended to enhance their mental health and well-being.
Introduction
Adolescents develop social and emotional habits during this period, which are important for mental well-being. 1 Nearly 15% of the world’s adolescents grapple with mental health challenges, often unnoticed and untreated. 1 Global estimate of depression is 1.3% in 10-14-year-olds and 3.4% in 15-19-year-olds. 1 An episode of depression during adolescence signifies a chronic or recurrent disorder and predicts an array of psychosocial challenges and poor health outcomes. 2 During adolescence, depression may be misinterpreted as angst or hormone-related moodiness despite its significant ramifications. 3 This is more pronounced among adolescents with vision impairment as they face added challenges and exclusion, consequently experiencing more depression than sighted children.4-6 Factors contributing to mood disorders among such populations include reduced mobility, loneliness, limited social skill opportunities, and greater dependency on help. 7
Nepal has ensured that children with severe vision impairments learn in inclusive settings in integrated schools.8,9 Among their many health issues, mental health conditions are often unknown and unaddressed. Routine screening to identify both those at risk of mental health problems and those requiring treatment has been recommended for children with life-limiting conditions. 10 Hence, this study aimed to determine the prevalence of depressive symptoms among adolescents with vision impairment in Nepal.
Methodology
This quantitative descriptive cross-sectional study was conducted from September to November 2021. We reviewed records from the Center of Education and Human Resource Development, Nepal, to identify four integrated public schools with the highest enrollment of adolescent students with vision impairment. One school was selected from each of Kathmandu and Lalitpur districts in Kathmandu Valley and from Banke and Surkhet districts in western Nepal. Inclusive education promotes social and academic inclusion for all children, including children with blindness and low vision. 11 Students with vision impairment at these schools live in hostel settings.
Detailed ocular examinations were conducted with the help of consultant pediatric ophthalmologists and optometrists to group adolescents with blindness or low vision at their school premises. Adolescents have blindness if their visual acuity in the better eye is less than 3/60 with the best possible correction. 12 They have low vision if their visual acuity is less than 6/18 but equal to or better than 3/60 with the best possible correction. 12
We trained enumerators for uniformity in approaching potential participants and data collection. Male enumerators interviewed boys, and female enumerators interviewed girls. Participation in the study was voluntary, and trained enumerators read the information sheet to adolescents and parents or caretakers before data collection. We obtained written informed consent from parents or caretakers and verbal assent from adolescents. Any adolescent with vision impairment who was absent on the day of data collection, as well as those with known additional disabilities, were excluded from the study. Among 69 adolescents with vision impairment, 65 (94.20%) completed the survey. One student with a physical disability was excluded from data analysis, and three did not assent to participate in the study.
We conducted face-to-face interviews using the Nepali version of the Depression Self-Rating Scale (DSRS) to determine depressive symptoms.13,14 DSRS has demonstrated good psychometric properties and has been effectively used with adolescents in non-clinical settings. 15 DSRS consists of 18 questionnaires assessing feelings over the past week with response options of mostly, sometimes, or never, scored as 2, 1, and 0, respectively, with overall scores ranging from 0 to 36. Depressive symptoms were defined to be present if the total DSRS score was greater than 14. The trained enumerators read the questions and the response options aloud to participants during data collection.
Data were entered and cleaned in Microsoft Excel 2019 and analyzed using IBM SPSS 26.0. Fisher’s exact test and odds ratios at 95% confidence intervals were computed to identify factors associated with depressive symptoms. Statistical significance was determined at a P-value less than .05.
Results
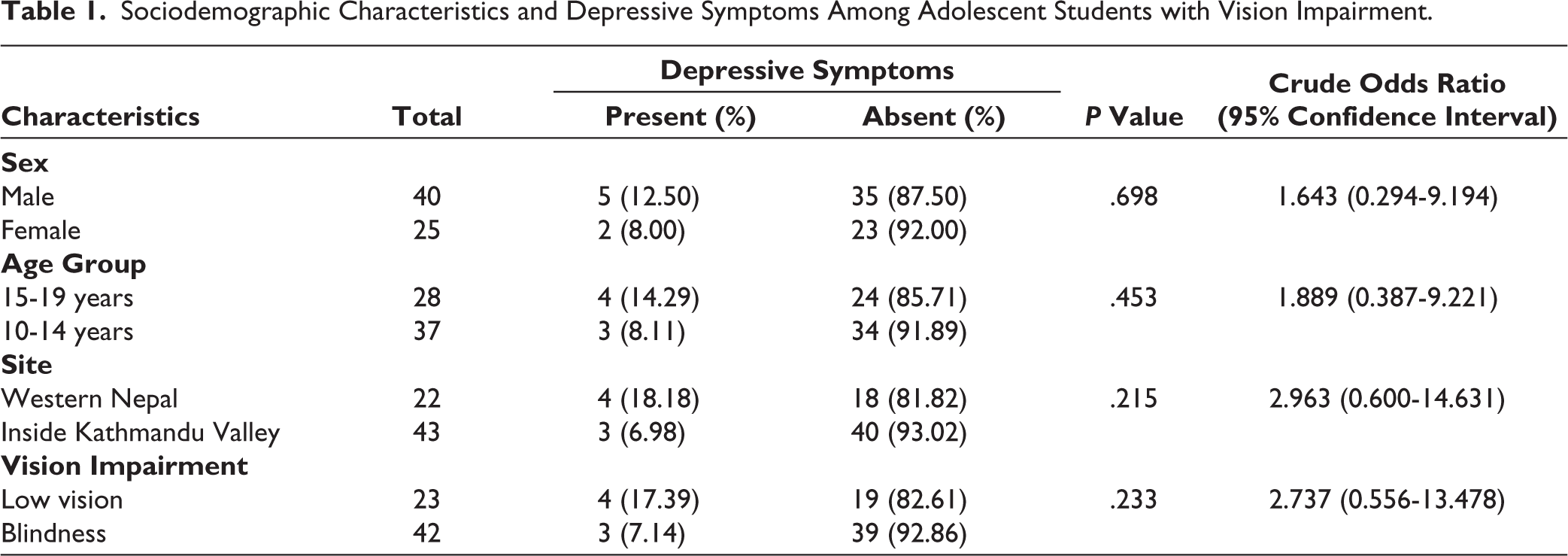
Among 65 adolescents with vision impairment, 7 (10.77%) had depressive symptoms. The mean age of the study participants was 13.97 ± 2.14 years. Table 1 shows there was no significant association between variables of interest, such as age, gender, location, and type of vision impairment, and depressive symptoms.
Sociodemographic Characteristics and Depressive Symptoms Among Adolescent Students with Vision Impairment.
Discussion
Our study showed 10.77% of adolescents with vision impairment had depressive symptoms. In India, 13.8% had depression among school adolescents with blindness. 16 The prevalence falls within the 9%-20% range reported in a meta-analysis of children with blindness and adolescents. 17 The prevalence of depressive symptoms among adolescents with vision impairment in our study is higher than the global estimate of depression for all adolescents, which is 1.3% for 10-14 year olds and 3.4% for 15-19 year olds. 1 Studies have also shown that depression is more prevalent in adolescents with blindness than in those with low vision or their sighted peers.18,19 However, in our study, adolescents with low vision were more likely to experience depressive symptoms than those with blindness, but the association was not statistically significant. This finding is similar to a study in Nepal, where children aged 7-17 years with blindness had better psychosocial functioning than those with low vision. 20 Lack of low vision rehabilitation among those with residual vision may hinder their adaptation, limit their independence, and increase the risk of developing depressive symptoms. Providing tailored care based on their vision impairment and emphasizing gradual adaptation and coping strategies may enhance their overall quality of life.
The male adolescent students with vision impairment had higher odds of having depressive symptoms than female adolescents in our study, but the difference was not statistically significant. A review also showed no significant difference in depressive symptoms between female and male adolescents with vision impairment. 17 In contrast, female children with vision impairment in the USA were more likely to have depression than males. 21 Among public school adolescents in Nepal, females were more likely to have depression than males.22,23 The discrepancy in findings between our study and those studies may be due to the small sample size, and further research is needed to explore the relationship between vision impairment, depression, and gender in adolescents. The social context of gender and inclusion is important to consider. 24 Social exclusion among students with vision impairment in schools has been linked to an increased risk of depression. 25 Future studies should consider qualitative research to explore the social contexts and gender norms influencing depressive symptoms.
In our study, older adolescents with vision impairment were likely to exhibit depressive symptoms than younger adolescents, but the difference was not statistically significant. Similar results have been reported among adolescents in childcare homes in Nepal, where older adolescents had higher odds of depressive symptoms than younger ones. 26 Older adolescents may have greater awareness of future educational and economic challenges posed by vision impairment, exacerbating their depressive symptoms. Students with vision impairment face unique challenges in academic learning and achievement. 17 Improving access to adaptive modern technologies designed to meet their needs can help them in academic learning.
In our study, adolescents with vision impairment attending schools in western Nepal showed higher odds of depressive symptoms compared with those from Kathmandu Valley, though this difference did not reach statistical significance. A study among schoolchildren aged 6-16 years in Nepal found small differences in emotional and behavioral problems between geographic regions and rural and urban living areas. 27 Students in Kathmandu Valley come from both within the Valley and different districts of Nepal. Their families often reside and work within the Valley, enabling regular family interactions and emotional support. In contrast, students of western Nepal come from local and surrounding districts, and families rarely reside near them. Parents in western Nepal often face challenging geographic terrain and limited transportation, leading to fewer visits and reduced emotional support. This disparity in family proximity and support might have contributed to the observed differences in depressive symptoms. Transforming and equipping existing public schools into integrated schools with inclusive education in different districts of Nepal could help address these challenges.
The study was limited to adolescent students with vision impairment and did not include out-of-school adolescents with vision impairment, who might face even greater mental health challenges. The use of enumerator-administered DSRS may have introduced social desirability or response biases, as opposed to self-rated assessments. The small sample size and non-probability sampling limit generalizability and may skew findings. The study lacked comparison with sighted peers, limiting causal inference. Despite these limitations, this research can inform policymakers, educators, and healthcare providers about the mental health needs of adolescents with vision impairment in Nepal.
Conclusion
Our study shows that adolescents with vision impairment in schools are suffering from depressive symptoms. We recommend exploring the causes and creating a supportive environment tailored to address their challenges. This approach should promote their mental health and overall well-being through targeted interventions, implementing inclusive practices, and fostering a culture of understanding and acceptance.
Footnotes
Acknowledgements
We extend our heartfelt thanks to the resource teachers and caretakers of all four integrated schools in this study. We are also immensely grateful to the enumerators and study participants for their cooperation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the USAID Child Blindness Program (GR2-CBP015). The funder had no role in the study design, data collection, management, analysis, interpretation, writing of the report, or the decision to submit for publication.
Statement of Informed Consent and Ethical Approval
Ethical approval for the study was obtained from the Ethical Review Board of the Nepal Health Research Council, Kathmandu, Nepal (protocol No. 268/2021 P).