
Abstract
Background:
Previous studies have shown the negative impact of institutional care on children’s physical and mental health. However, in addition to the form of care, the quality of care is an important factor in children’s mental health. This study explored the quality of care and the association between the quality of care and mental health issues among adolescents in Vietnam social support facilities (SSFs).
Methods:
A cross-sectional study was conducted with 273 institutionalized adolescents who lived in SSFs and 273 adolescents cared for by family. Depressive symptoms, anxiety symptoms, sleep problems, behavioral problems, and quality of care were measured. Descriptive statistics were calculated, and multiple linear regression analysis was performed.
Results:
The quality of care was rated as quite high by institutionalized adolescents. However, the mean score for quality of care was significantly lower for institutionalized adolescents than for the comparison group. The quality of physical care did not show a significant relationship with mental health risk, except for anxiety. In contrast, emotional care was negatively associated with all common mental health problems including anxiety (beta = –0.40, P < .001), depression (beta = –0.31, P < .01), conduct behavior (beta = –0.30, P < .01) and sleep problems (beta = –0.30, P < .01). An increase in emotional care was therefore associated with a decrease in mental health problems.
Conclusions:
Emotional care is more important than physical care for adolescents in SSFs. It is necessary to improve the quality of care, particularly emotional care, for adolescents to reduce the risk of mental health problems.
Introduction
The mental health of institutionalized children is a matter of concern. Since the 1960s, studies have shown that anxiety symptoms are more common in institutionalized children than in children in family settings.1,2 Subsequent studies have shown that children who have experienced institutional care have a higher rate of mental health problems than children who have never been placed in an institution.3,4 During adolescence, the risk of mental health problems increases due to age-related psychological characteristics and prolonged time in adverse living environments. The prevalence of common mental health problems, such as depression, anxiety, suicide, sleep problems, and posttraumatic stress disorder, is high,5-12 and behavioral problems such as animal abuse, violence, and substance abuse are common.3,13,14 Deinstitutionalized children who were removed from institutional facilities and fostered in a family setting also exhibited a significant decrease in mental health problems.3,4,14
There are many factors related to mental health problems among institutionalized children. The most common risk factor is experiencing abuse. The majority of children in institutions experience at least one type of trauma or adversity in early childhood, such as being beaten, losing loved ones, being abandoned, witnessing violence, or being victims of sexual abuse.15-20 Even after children are rescued from violence, poverty, or parents with substance abuse issues and subsequent care in institutions, they are still at risk of abuse and violence from caregivers or staff at institutions. Rus et al. investigated 1391 children aged 7–20 years old living in Romanian institutions and found that 39.5% of the children reported that they had been severely beaten by staff, with 80% reporting being severely punished many times. 21 Another study showed that among children who experienced physical abuse, 71% reported that they were abused by their caregivers. 22
The quality of care is also a matter of concern that affects the mental health of children in institutions. Previous studies have focused on the quality of care and its correlation with well-being among institutionalized children. Huynh et al. showed that quality of care (including food security, the quality of shelter, the quality of caregiving, and access to health care services) predicted psychosocial well-being among institutionalized children in low- and middle-income countries. 23 In other words, the better the quality of care, the better children’s mental health is. Improving the quality of institutional care settings by preventing violence, abuse, and neglect of children and providing caregiver training, were considered interventions for children’s emotional, social, and cognitive development. 24
In Vietnam, the social support facilities (SSFs) terminology was first used in Decree No. 103/2017/ND-CP dated September 12, 2017, for the establishment, organizational structure, operation, dissolution and management of SSFs. SSFs are a form of institutional care for children in Vietnam and include social patronage centers, warm shelters and compassionate homes, open homes, specialized schools for children with disabilities, SOS villages, and orphanages. Few studies have focused on children’s mental health among children in SSFs in Vietnam. A survey of institutionalized children aged 6–18 years who were living in two SSFs in Vietnam revealed that approximately 0.9%–8.9% of the children had behavioral problems, the most common of which were delinquent behaviors (8.9%) and the least common of which were somatic complaints (0.9%); furthermore, 5.4% of the children had two or more problems. 25 A previous study indicated that the prevalence of common mental health problems such as anxiety, depression, and suicidal ideation among adolescents (12–18 years old) in SSFs in Vietnam ranged from 21.2% to 25.6%. 26 However, the issue of quality of care and its correlation with mental health problems among Vietnamese adolescents in SSFs has received little attention.
Materials and Methods
Participants and Procedure
The data are from the Vietnamese Institutionalized Adolescent Mental Health Study, which was conducted in nine of the 63 provinces/cities in Vietnam. Details of the sampling and procedures have been described in our previous publication. 26 Briefly, 11 institutions were selected from nine provinces/cities, including three municipalities, three delta provinces, and three mountainous provinces. A total of 546 participants aged 12–18 (Mage = 14.9, 41% boys) were equally divided into two groups: 273 institutionalized adolescents living in SSFs, called the IA group, and 273 adolescents living in family settings, called the NIAs. The NIA group was sampled from two junior high schools and two senior high schools to match the gender, grade and age distributions of the IA group. The inclusion criteria for the participants were age 12–18; having previously lived in an SSF for at least 6 months (for the IA group); consent to participate provided by a legal guardian, and assent to participate from the adolescents. Participants were excluded if they had a history of or active chronic psychosis, physical disabilities, intellectual disabilities, or reading difficulty. All relevant information sheets and forms, such as research purposes, questionnaires and consent forms for parents, other legal guardians or a legally authorized official (heads of the institutions or school administrators), were submitted and consent was obtained for minors’ participation. Assent was also obtained from all participants before the study was initiated. The participants were informed about the right to withdraw from the study without repercussions. The research design and ethical considerations were reviewed and approved by Hue University (Project No. DHH2023-01-207) and the target facilities and schools.
Measures
Sociodemographics
A self-report survey was designed to collect information about adolescents’ sociodemographic characteristics such as age, gender, biological parent status, onset of being institutional care, and length of institutional care. The details of the sampling and data collection were described in our previous publication. 26
Quality of Care Questionnaire
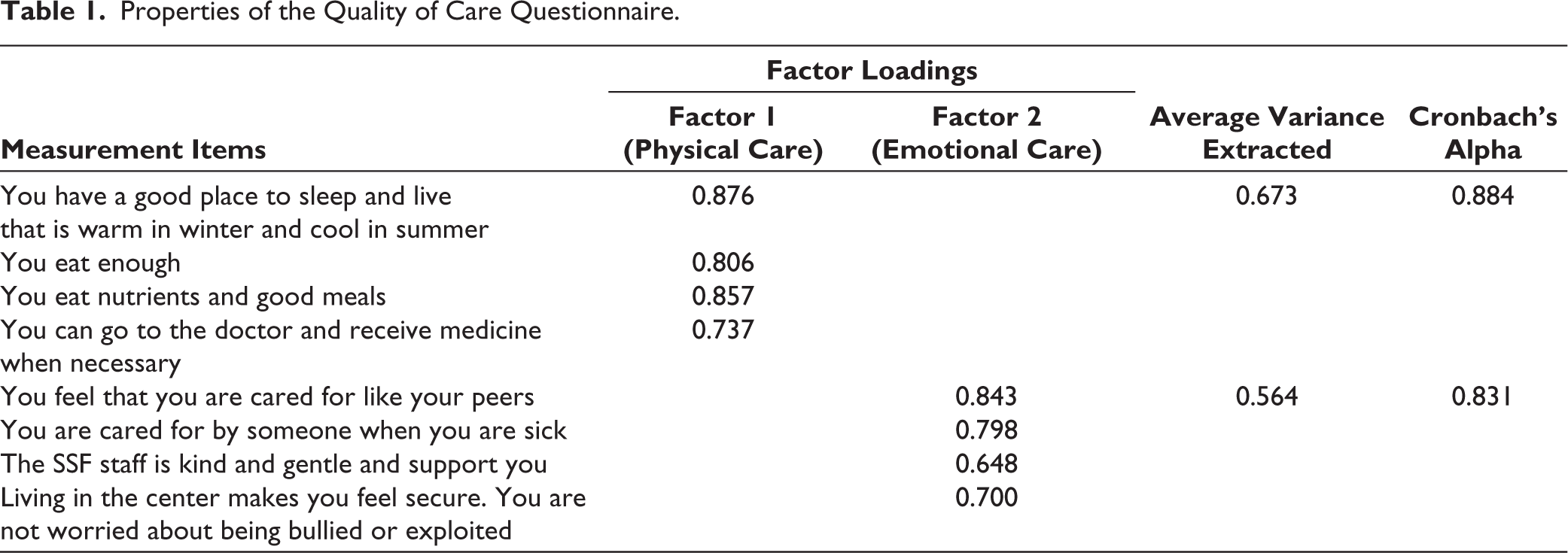
A questionnaire was developed to measure the quality of child care based on the Child Status Index. 27 The questionnaire consisted of eight questions that focused on two aspects: physical care conditions including food security, nutrition, shelter and medical care (four questions) and emotional care conditions including love and protection (four questions). Confirmatory factor analysis was performed, and the average variance extracted and Cronbach’s alpha coefficient were calculated to evaluate the validity and reliability. The results showed that the factor loading of all the items was greater than 6 and the average variance extracted for physical care and emotional care conditions was 0.673 and 0.564, respectively (>0.5), indicating that the scale had good convergent validity. 28 The Cronbach’s alpha coefficient was 0.884 and 0.831, respectively (see Table 1).
Properties of the Quality of Care Questionnaire.
Depression Scale
The current study used the Vietnamese version of the Center for Epidemiologic Studies Depression Scale (CES-D) developed by Radloff. 29 The scale consists of 20 items with a total score ranging from 0 to 60 points that measure depressive symptoms during the previous week. A higher score indicates more severe depressive symptoms. The corresponding items have four answer options, namely “less than 1 day,” “1–2 days,” “3–4 days,” and “5–7 days” with scores ranging from 0 to 3 points. The Vietnamese version of the CES-D has shown good validity and reliability among middle and high school students. 30 In the current study, the Cronbach’s alpha coefficient of the scale was 0.87.
Anxiety Scale
A questionnaire developed by Nguyen, Le, and Dunne to assess anxiety in Vietnamese adolescents was administered. 30 This scale consists of 13 items, each of which is answered on a 3-point Likert scale ranging from 1 (never) to 3 (often). The total score ranges from 13 to 39. A higher score indicates more severe anxiety symptoms. The questionnaire demonstrated good validity and reliability among Vietnamese adolescents. The Cronbach’s alpha coefficient of the questionnaire was 0.79.
Sleep Problems
Sleep problems were assessed with regard to three aspects: insomnia, nightmares, and self-assessment of sleep quality. Insomnia symptoms and nightmares questions were developed based on diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) and the Pittsburgh Sleep Quality Index (PSQI) to measure insomnia symptoms. These questions included the following: “During the past month, have you been unable to get to sleep within 30 minutes?”; “Have you woken up in the middle of the night and then taken a long time to get back to sleep?”; “Have you woken up early in the morning and unable to return to sleep?”; and “Have you had nightmares?” The items were rated on a five-point scale: “never = 0,” “less than once a week” = 1, “once or twice a week” = 2, “three to five times a week = 3” and “almost every day = 4.” In addition, a self-assessment question asked about sleep quality, which was scored on a scale of 0 (very good) to 4 (very bad). The Cronbach’s alpha coefficient of the questionnaire was 0.74.
Conducting Behavior
The current study used the conduct behavior subscale of Goodman’s Strengths and Difficulties Questionnaire (SDQ). The Vietnamese version of the SDQ demonstrated good reliability according to Dang et al. 31 and is widely used in Vietnam. In our study, the Cronbach’s alpha coefficient of the subscale was 0.73.
Statistical Analyses
First, to detect the possible impact of common method variance, we used Harman’s single-factor test. The analysis showed that the total variance explained by one factor was 10.71%, which was less than 50%.32,33 This finding showed that there was no serious common method bias in the research data.
Next, we calculated descriptive values such as the mean and standard deviation (std).
Finally, to explore how the care conditions were associated with mental health problems, we performed four different multiple linear regression models while controlling age, gender, BMI, parent status, length of institutional care, and onset of institutional care. Mental health problems (i.e., depression, anxiety, conduct problems, and sleep problems) were considered dependent variables, while physical care conditions and emotional care conditions were known as independent variables.
All analyses were performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 22.0.
Results
Results of the Assessment of Quality of Care at the SSFs
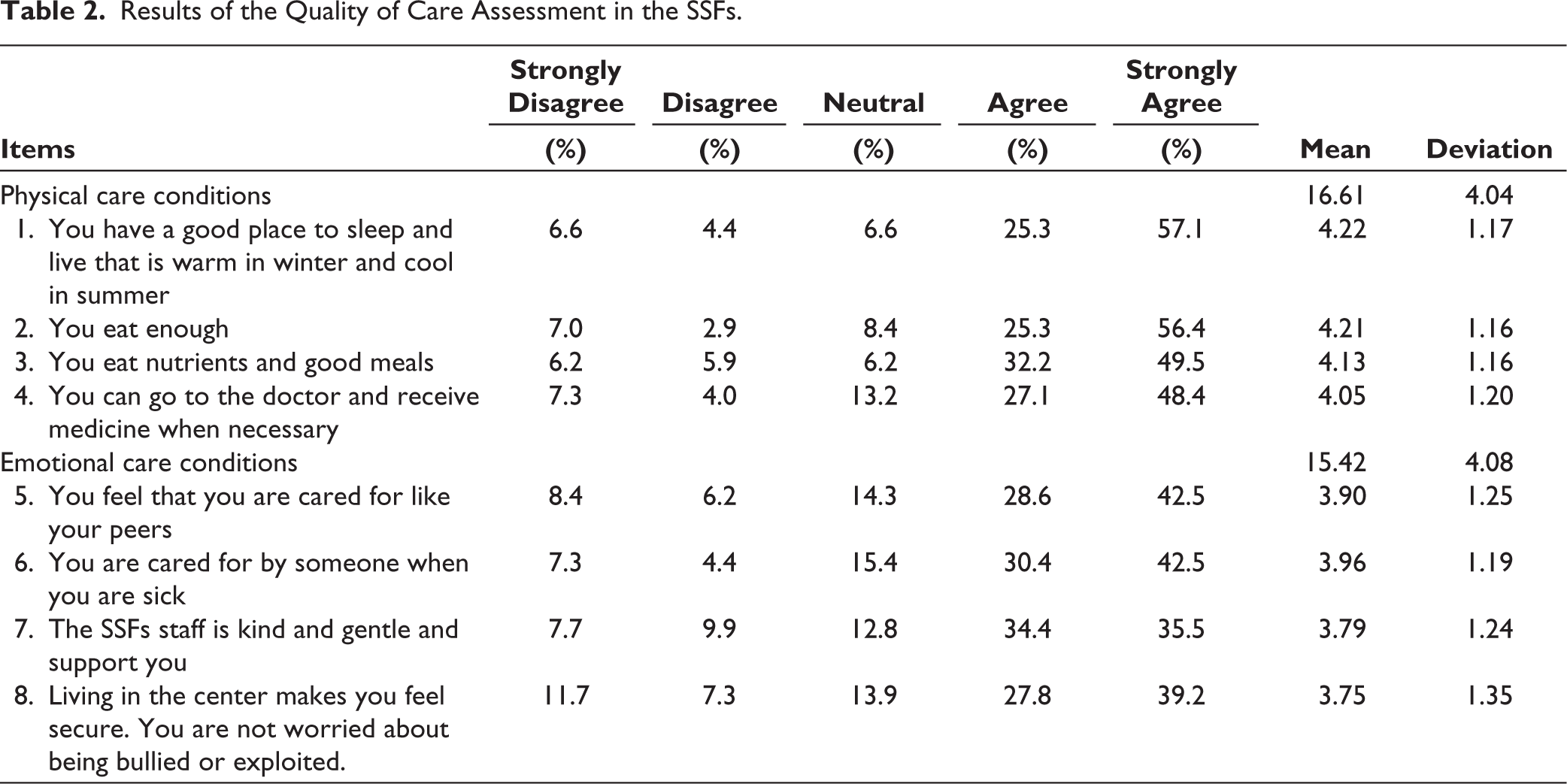
We assessed the quality of care based on descriptive statistics including the percentage, mean and std (Table 2). The results indicated that the children were well assured of both physical and emotional care. Most of the children selected “agree” or “strongly agree” for all items, with an average score of 3.75–4.22. In addition, the results showed that the average score for physical care conditions (mean = 16.61) was greater than that for emotional care (mean = 15.42).
Results of the Quality of Care Assessment in the SSFs.
Comparison of Quality of Care and Mental Health Problems Between the Two Groups of Subjects
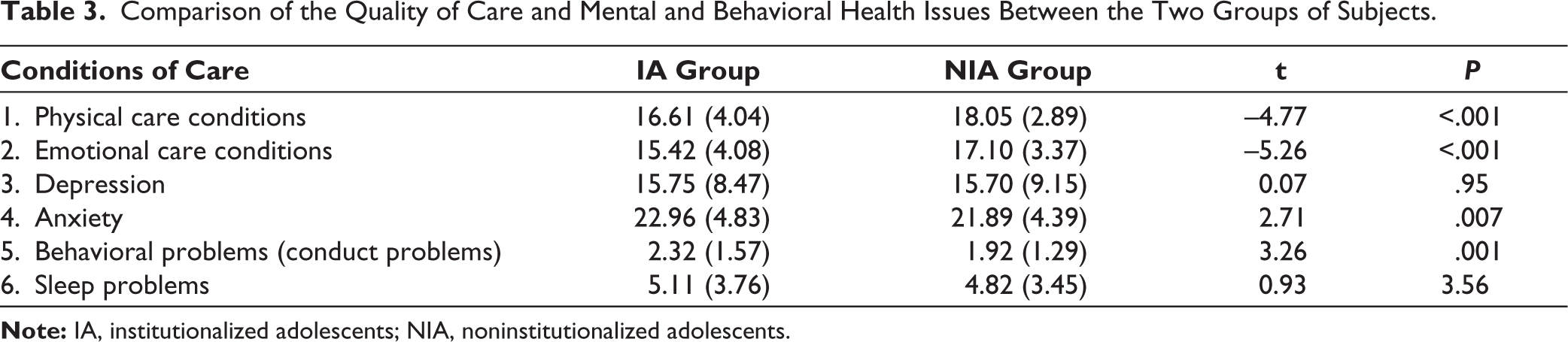
In this research, we compared the quality of care and mental health problems between children who lived in institutions and those who did not. We conducted a t-test for two independent variables. The results of the analysis are shown in Table 3.
In the current study, the mean score for quality of care was significantly lower in the IA group than in the NIA group. In particular, this was shown in terms of both physical care and emotional care (t = –4.77 and t = –5.26, respectively; P < .001). In terms of mental health, the symptoms of depression and sleep problems did not differ significantly between the two groups (t = 0.07 and t = 0.93, respectively; P > .05). Notably, however, adolescents in the institutional care setting had a greater risk of anxiety and behavioral problems than those in the family care setting (t = 2.71 and t = 3.26, respectively; P < .01).
Comparison of the Quality of Care and Mental and Behavioral Health Issues Between the Two Groups of Subjects.
The Relationship Between Quality of Care and the Prevalence of Mental Health Problems Among Adolescents in SSFs
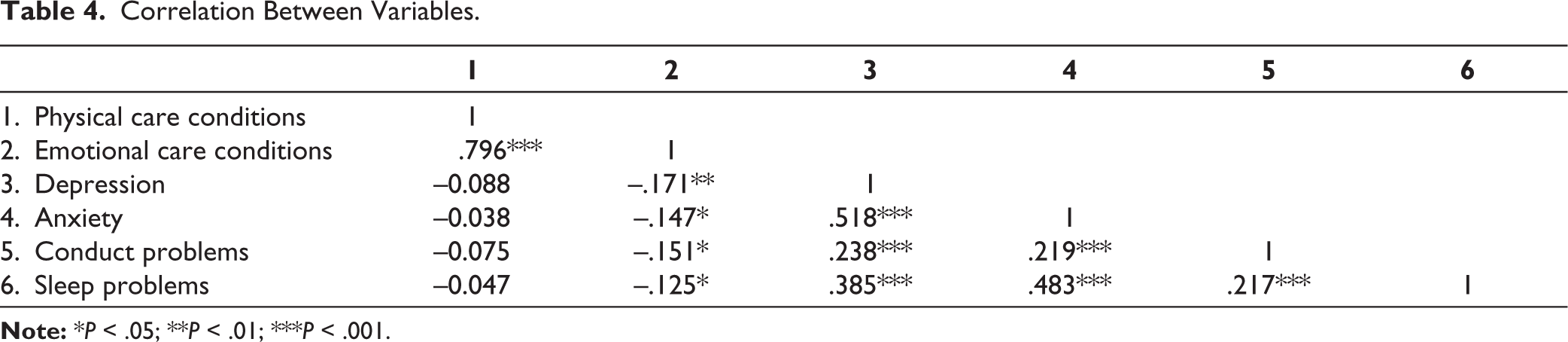
In all multiple linear regression models, the linear correlation between each pair of variables was checked. The correlation coefficients between variables were below 0.80 (see Table 4). VIF values (see Table 5) less than five indicated that multicollinearity was not problematic. 34 It implies that the variables considered are moderately correlated. Residuals of the model were normal distributed, which was checked by histogram charts, normal P-P plots, and scatterplots. All of this indicates that assumptions for models are satisfied.
Correlation Between Variables.
The results of multiple linear regression analysis for the IA group are presented in Table 5. In the current sample, the association between quality of physical care and symptoms of mental health was not significant, except for anxiety (β = 0.28, P < .01). However, emotional care was significantly associated with all common mental health problems including anxiety (β = –0.40, P < .001), depression (β = –0.31, P < .01), conduct problems (β = –0.30, P < .01) and sleep problems (β = –0.30, P < .01). Negative standardized coefficients (β) indicates that an increase in emotional care is linked to a decrease in mental health problems.
Associations Between Mental and Behavioral Problems and Quality of Care Among Institutionalized Adolescents.
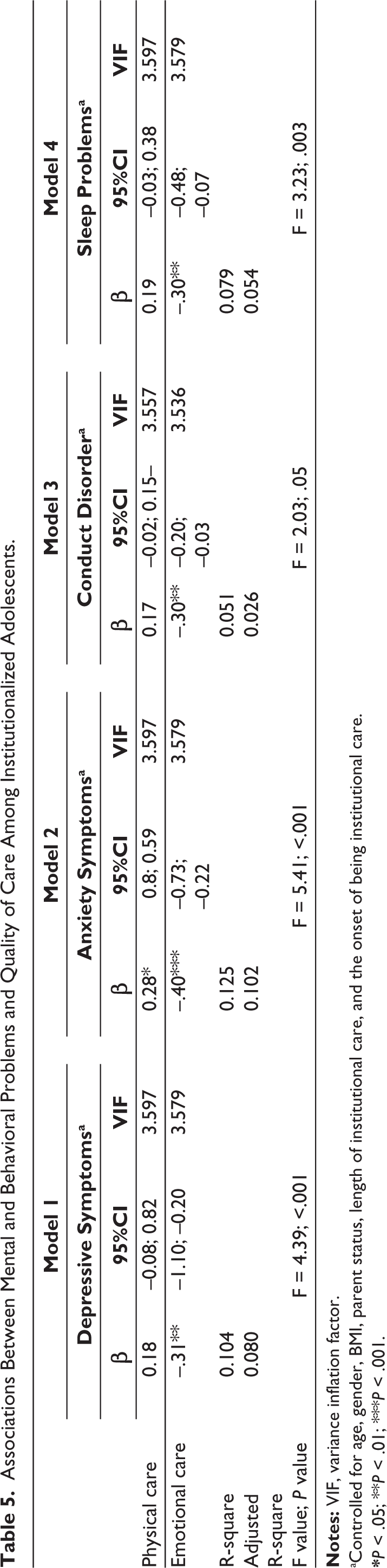
aControlled for age, gender, BMI, parent status, length of institutional care, and the onset of being institutional care.
*P < .05; **P <.01; ***P < .001.
Discussion
Recently, studies related to orphanages and abandoned children have been controversial with regard to the importance of the form or quality of care. To the best of our knowledge, this study is the first to focus on the relationships between the quality of care and mental health and behavioral problems among institutionalized adolescents in Vietnam. This study provides important evidence for improving the quality of care and enhancing mental health care for institutionalized children in Vietnam.
The results showed that most IAs give high evaluations of the quality of care at the SSFs, where they are provided with basic needs such as food, shelter, medical check-ups, attention, encouragement, and protection. Remarkably, they have ensured enough accommodation and enough nutritious meals. According to the Vietnamese Government of Decree 20/2021/ND-CP, children in SFFs receive monthly social allowances ranging from 1,440,000 to 1,800,000 Vietnamese dong (equivalent to 60 USD to 77 USD) depending on their age. This amount is mainly used to provide meals for children. The children also receive additional support, such as household items, stationery, books, etc. In addition, many SSFs have attempted to mobilize financial resources via donations or charity to improve meals for children. This is likely the main reason why the majority of participants reported high satisfaction with the quality of care. Another possible explanation for this result is the early childhood experiences of the IA group. With the exception of some children who were abandoned by their parents after birth, numerous children in the IA group have spent their childhood in many different environments. Many of them live in families with poverty, violence, alcoholic parents, or even live on street, begging or working as vendors or laborers. 35 Consequently, IAs may tend to be satisfied and appreciate their current quality of life even though it may not be ideal.
Unlike physical care, emotional care conditions face more challenges. According to Circular No. 33/2017/TT-BLĐTBXH dated December 29, 2017, each caregiver can take care of a maximum of 10 healthy children and four disabled children. However, the reality is different from this standard. In fact, caregivers in SSFs must take care of many children despite limited knowledge and skills, high work pressure, an overwhelming workload, and limited income. 35 This is a major challenge, not only in Vietnam but also in other low- and middle-income countries, where many orphaned and abandoned children are in need of care while resources are still limited. 24 This may be the main factor that influences the care, love, and concern of caregivers toward the children.
Our results revealed that the quality of care is lower for adolescents living in institutional care settings than for those living in family settings. This finding is consistent with several previous studies in different countries with different cultural backgrounds, such as Japan, Norway, and Turkey.36-38 This is understandable and may explain why deinstitutionalization has become a trend. Deinstitutionalization requires the preparation of essential conditions such as the establishment of a system of alternative services, a proper child protection system, the development of a strong social work system and increased awareness of children’s rights and child development. 39 In the immediate future, the childcare system in Vietnam has not met these conditions. Therefore, the immediate work that must be done is to improve the quality of care, both physically and emotionally, to ensure the safety and well-being of children in institutions.
An important finding of the current study is the correlation between the quality of care and mental and behavioral health issues. Notably, correlations between physical care conditions (housing, food, health care, etc.) and mental health and behavioral issues were not found. In contrast, emotional care conditions were negatively correlated with depression, anxiety, sleep problems, and conduct problems. Multiple linear regressions showed that an increase in emotional care conditions was linked to a decrease in mental health problems. These results are inconsistent with those of previous studies in five low-income countries. A study of low- and middle-income countries revealed that all components of quality of care including food security, shelter and health care services, significantly predict the well-being of orphan and separated children. 23 This result may be related to the quality of childcare at the SSFs in Vietnam. A previous study showed that more than 80% of adolescents living in Vietnamese SFFs have experienced some form of physical, emotional, and/or sexual abuse and neglect. 26 Other studies have shown that institutionalized children suffer from caregiver punishment.21,22 These experiences of neglect and abuse experiences have been found to be related to mental health problems among many IAs in Vietnam. 26
These findings indicate that in addition to ensuring physical care condition, it is necessary to improve the quality of care in terms of emotional aspects, such as increasing the care, love, tenderness, and gentleness of caregivers. It would be an important solution to decrease mental health problems for adolescents who are living in SSF in Vietnam. Specific solutions should focus on improving the knowledge and skills of caregivers. A similar strategy has been effective in Tanzania. The results of an intervention showed that after caregivers received support to improve their knowledge and skills, the incidence of child abuse tended to significantly decrease,40,41 and the prevalence of depression among institutionalized children also decreased. Another approach is to minimize violence, abuse, and neglect in institutional as much as possible. 24 The combination of caregiver training and efforts to control violence would be appropriate in Vietnam.
Limitations
This study has several strengths including a representative research sample, a focus on vulnerable adolescents and a comparison between two groups of adolescents receiving care in different settings. However, this study also has several limitations. First, self-reported data were collected, which can influence to the measurement, particularly the quality of care rating. In addition, the participants were living in institutions, which may have led to biased self-reports. Second, the quality of care questionnaire was answered only by adolescents, not by caregivers or other relevant adults. Third, because this was a cross-sectional study, it could identify associations but not causal relationships between quality of care and mental health problems. Fourth, as mentioned above, many children in the IA group lived in dysfunctional families before being institutionalized, which might have different effects on children’s mental health and behavioral problems as well as how they evaluate the current quality of care. Unfortunately, the present study did not explore the specific reasons why each child was institutionalized. Further studies should focus on this sociodemographic variable.
Conclusion and Implications
According to the recommendations of UNICEF, provisions of the Vietnamese Law on Children (Law No. 102/2016/QH13) and regulations on alternative care for children in Vietnam, long-term care of children in SSFs is the last choice after all other solutions have failed. Moreover, the current study found negative correlations between the quality of emotional care and common mental and behavioral health problems. This implies that, in addition to accelerating the process of deinstitutionalization to give orphaned and separated children the opportunity to develop their full potential, it is necessary to improve the quality of care for children in the SSFs, particularly to improve their emotional care conditions.
Footnotes
Acknowledgements
The authors wish to thank all of participants, parents, the head of the institutions, and principal of the school in Vietnam who kindly approved and allowed the participation of adolescents.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The participants were informed about the research purposes, information privacy policy and right to withdraw from the study without repercussions. Informed consent/assent was also obtained from all participants before the study was initiated.
The research design and ethical considerations were reviewed and approved by Hue University (Project No.: DHH2023-01-207) and the target facilities and schools.