
Abstract
Pediatric acute-onset neuropsychiatric syndrome (PANS) is defined by abrupt emergence of obsessive–compulsive behaviours and/or food restriction with concurrent cognitive and behavioural symptoms. Symptoms of obsessive–compulsive disorder and eating disorder frequently overlap in such cases, clouding diagnostic certainty and hypothesized etiologic factors. This case illustrates an atypical eating disorder presentation, resulting from PANS wherein a meticulous ruling out of organic causes andtimely institution of specific serotonin reuptake inhibitor facilitated remission. Through this case report the authors highlight the need of awareness of other medical practitioners regarding the symptomatology and presentation of PANS so as to facilitate early intervention in a collaborative approach.
Introduction
Pediatric Acute Onset Neuropsychiatric Syndrome (PANS) is defined by abrupt onset of obsessive-compulsive disorder (OCD) or severely restricted food intake, associated with other fluctuating neuropsychiatric symptoms such as anxiety, emotional lability and/or depression, irritability, aggression, and/or severe oppositional behaviors, developmental regression, deterioration in school performance, sensory or motor abnormalities, and somatic symptoms. 1 About 10% to 20% of pediatric onset OCD and 50% of pediatric onset anorexia are linked with PANS.2,3 To date, studies in the area of PANS, including pediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS) and pediatric infection-triggered neuropsychiatric disorder (PITAND), have been relatively small and hence unable to comprehensively address questions of heterogeneity in clinical presentation. This case demonstrates a complex presentation of overlapping restrictive eating behavior and affective, psychomotor, and behavioural alterations following PANS posing a diagnostic dilemma and treatment challenge.
Case Details
A 13-year-old female child presented with a severe loss of appetite for the past 6 months, preceded by a bout of common cold, sore throat, and infrequent rise in body temperature lasting 5 to 7 days. Two weeks after the febrile illness, she started skipping meals citing reasons of reduced appetite, refusing protein-rich foods, and complaining of early satiety. Soon after, she was observed to have repetitive spitting, almost 20 to 30 times a day with no apparent reason. She also appeared socially withdrawn, confining herself to her room, unlike her usual self. Her interest in studies and scholastic performances dwindled. Her mood remained irritable and her defiance increased. However, there was no expression of any depressive cognition. By now, her restricted eating behavior had led to a weight loss of 10 kgs.
The reason for seeking psychiatry consultation was the recent onset of repetitive hand washing and prolonged time spent in bathing. At presentation, she had a BMI of 17 kg/m2 with extreme psychomotor retardation. Hemogram, renal function test, liver function test, and thyroid function tests were within normal limits. CT scan of the brain also showed normal findings and detailed CNS examination ruled out any meningeal signs or focal deficits. With a provisional diagnosis of PANS, she was started on Fluoxetine 20 mg, to which she responded well. In a follow-up visit after 2 months, she was playful, with reactive affect, improved appetite, and weight gain of 2.5 kgs with no repetitive behaviors.
Discussion
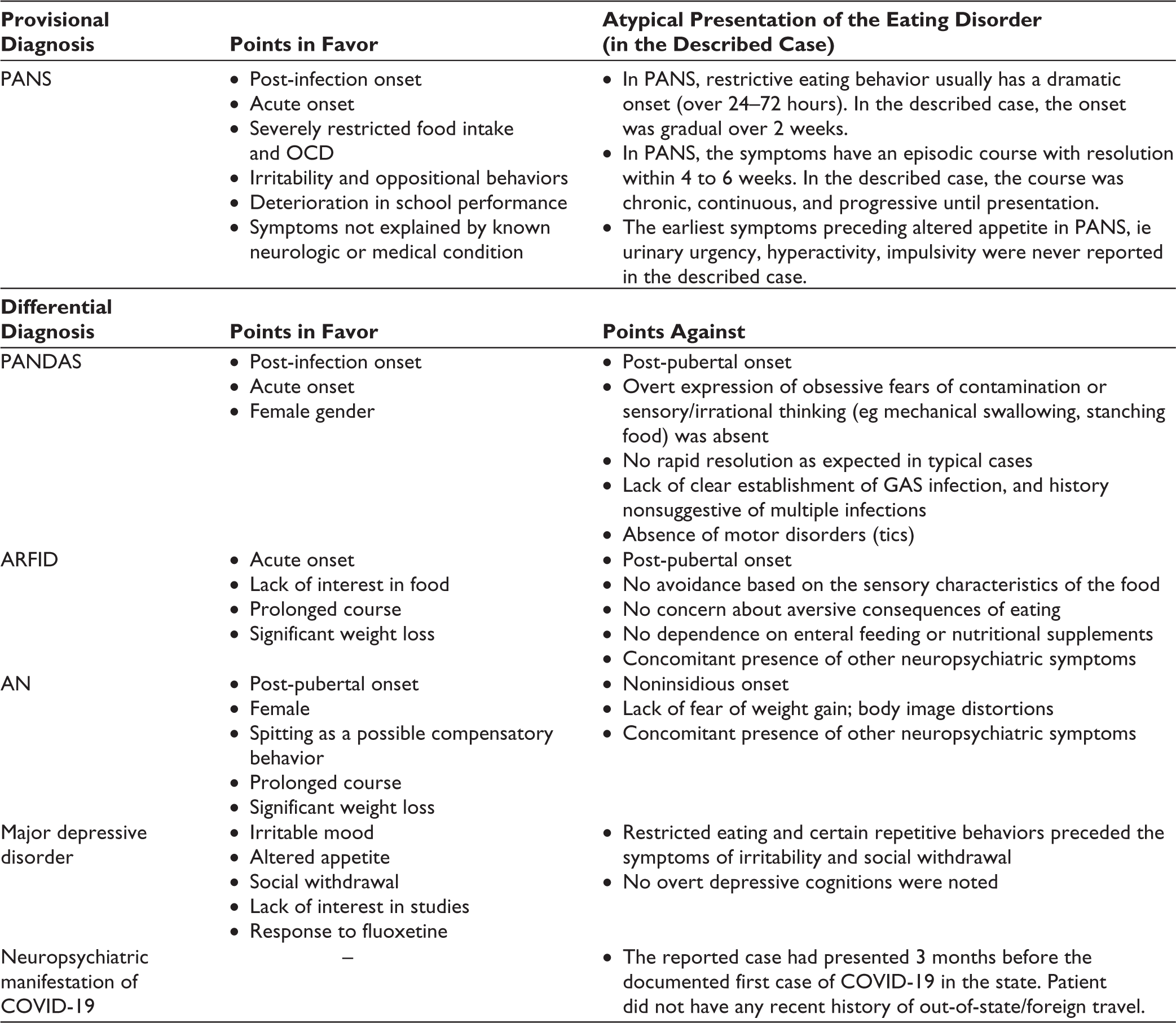
In our case, the post-infection onset of severe eating restriction, followed by changes in behavior and mood, and recent development of compulsive hand-washing favored a diagnosis of PANS. Other close differentials like PANDAS, Avoidant Restrictive Food Intake Disorder and Anorexia Nervosa were meticulously ruled out after consideration of the clinical pointers against them (Table 1). At the same time, few deviations from that of a classical PANS could be acknowledged such as gradual onset and continuous progressive course, as seen only in 8% of PANS cases. 2 A typical episode of PANS presents with initial symptoms of urinary urgency, hyperactivity, impulsivity, separation anxiety, and declining scholastic performance followed by gradual development of attention deficits, mood swings, and defiant behaviors. 4 Though certain repetitive behaviors like spitting and washing were observed, the associated cognition of body image disturbance, fear of weight gain, or contamination was absent. Altered appetite and obsessive-compulsive symptoms with psychomotor retardation have also been described in depressive disorders, 5 but other features of affective disorder were absent. No pointers towards psychosis were reported. Moreover, the patient responded to a trial of fluoxetine substantiating our diagnosis.
The causal mechanism is hypothesized to be multiple triggers initiating a neuroimmune process converging on a common pathway resulting in the varied clinical presentation. 6 Research is underway regarding potential treatments of PANS, but is currently limited. Empirical studies and case reports suggest that treatment should consist mostly of therapies that target immune and infectious causes. 1 We chose fluoxetine, because of its proven efficacy in treating selective neuropsychiatric symptoms of PANS.
Further studies are needed to understand the long-term course of PANS, the varying neuropsychiatric manifestations, and their management.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Informed consent was received before initiating the study. Anonymity of the patient was maintained throughout.