
Abstract

Early emergence of eating disorders (EDs) is a risk factor for developmental trajectories marked by excess morbidity and early mortality. 1 While psychiatric morbidity of adult EDs is well-characterized, 2 little is known on psychiatric comorbidity of EDs in childhood. Prior data show that up to half of the children with EDs meet the criteria for a comorbid psychiatric disorder, particularly mood and anxiety disorders 3 –6 However, studies typically include children and adolescents, combine mood and anxiety disorders, focus less on externalizing disorders, and/or do not examine both current and past comorbidity. Further study of psychiatric comorbidity in childhood has the potential to provide new insights regarding factors contributing to ED onset and maintenance. The purpose of the current report was to characterize the past and current psychiatric comorbidities across childhood EDs using nationally representative data.
Method
Participants and Measures
This study used data from the first wave of the Adolescent Brain Cognitive Development (ABCD) study collected from 2016 to 2017. The present analyses represent data from 11,876 U.S. children aged 9 to 10 years and a caregiver. Current and lifetime presence versus the absence of psychiatric disorders was confirmed using the computerized Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) 7 based on the Diagnostic and Statistical Manual of Mental Disorders, fifth edition criteria administered to the child’s caregiver. The K-SADS assessed sub- and full-threshold criteria for anorexia nervosa (AN), bulimia nervosa (BN), and binge-eating disorder (BED); sub- and full-threshold were combined, given lack of meaningful difference between full- and sub-threshold EDs. 8 See Supplemental Table S1 for definitions of subthreshold EDs. The ABCD study received approval from a central Institutional Review Board at the University of California, San Diego, and children’s caregivers provided written informed consent.
Statistical Analyses
Analyses were conducted in Statistical Package for the Social Sciences (SPSS) version 25.0. Those with EDs or binge eating were compared to those without the specified ED/behaviour on demographics using chi-square and t tests. Main analyses were conducted using the complex sampling module within SPSS. Complex sampling allows for the use of propensity weights, which are provided with ABCD data. Propensity weighting corrects for demographic selection bias and adjusts estimates to conform with nationally representative estimates. Logistic regressions, within the complex sampling module, examined associations between EDs and comorbid psychiatric disorders, covarying for sex, age, and race/ethnicity. Current comorbidities included diagnoses coded as present or in partial remission; past comorbidities reflected prior diagnoses that no longer met diagnostic criteria. Odds ratios with 95% confidence intervals that do not overlap with 1 are significant.
Results
One child met criteria for full-threshold AN-restricting subtype, and 1,029 met criteria for subthreshold AN. Six children met the criteria for full-threshold BN, and 15 met the criteria for subthreshold BN. Seventy-four children met the criteria for full-threshold BED, and 60 met the criteria for subthreshold BED. See Supplemental Table S1 for the comparison of EDs on demographic characteristics. There were no differences by sex. There were differences by race/ethnicity. The prevalence of AN was 8.7%, and most children were White (55.5%) or Hispanic (19.2%). Very few children met the criteria for BN (0.7%), but of those who did, a high percentage were Hispanic (69%). The prevalence of BED was 1.1% with White (32.1%) and Hispanic (33.6%) children showing the highest prevalence. Similarly, the prevalence of any binge eating was 5.0% with White (39.7%) and Hispanic (30.3%) children showing the highest prevalence. Asian children showed a relatively low prevalence of EDs.
Table 1 shows associations between EDs and psychiatric diagnoses. Prevalences ranged from 0% to 49% (past) and 0% to 55% (current) for comorbidity. Children with AN showed higher odds of past sleep problems and current attention deficit hyperactivity disorder (ADHD) and post-traumatic stress disorder (PTSD). Children with BN showed higher odds of past major depressive disorder (MDD), panic disorder (PD), obsessive-compulsive disorder (OCD), and PTSD; they also showed higher odds of current PD, generalized anxiety disorder (GAD), OCD, conduct disorder (CD), oppositional defiant disorder (ODD), and ADHD.
Comorbidity between Current Eating Disorders and Behaviour and Current and Past Psychiatric Disorders.
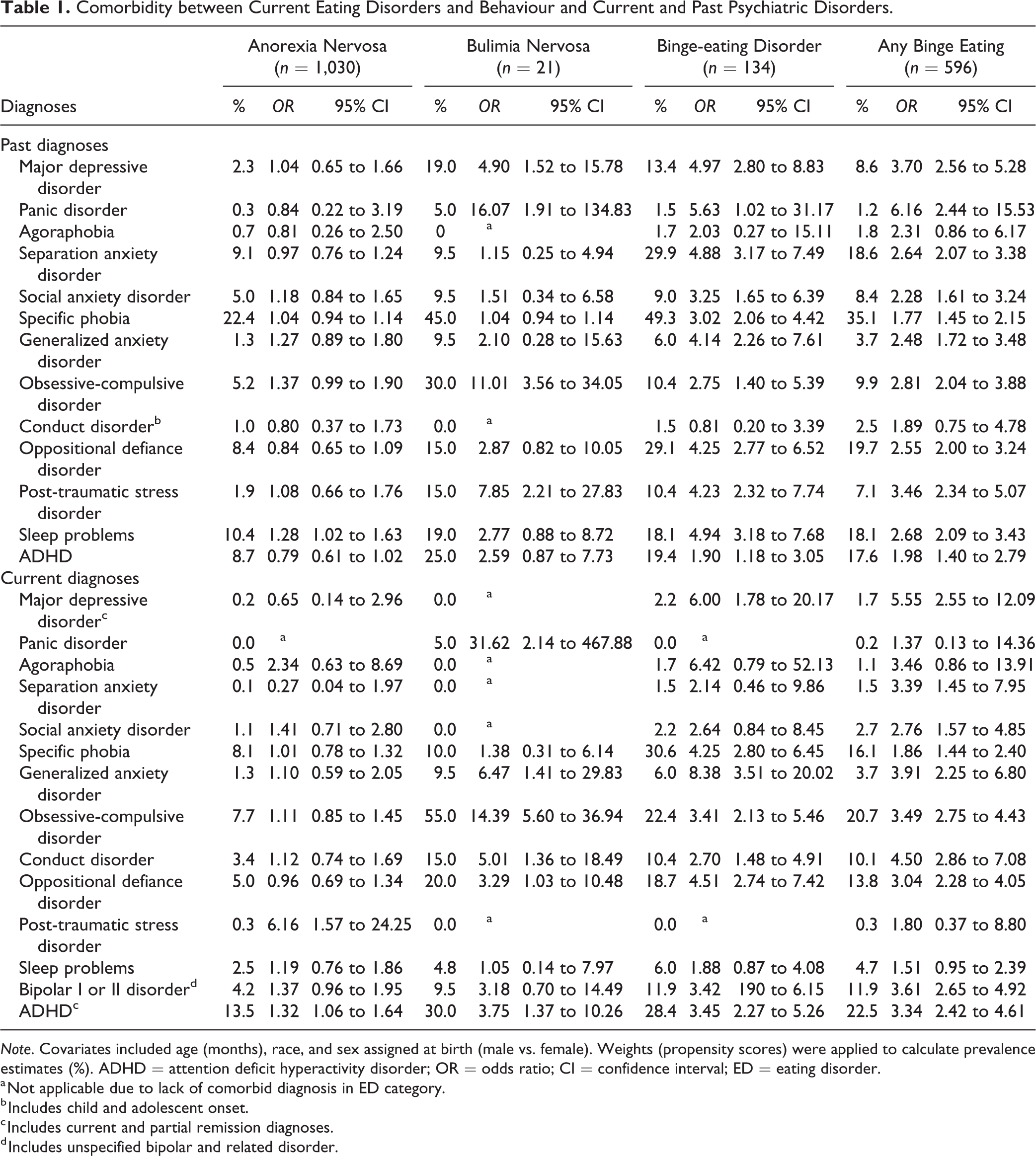
Note. Covariates included age (months), race, and sex assigned at birth (male vs. female). Weights (propensity scores) were applied to calculate prevalence estimates (%). ADHD = attention deficit hyperactivity disorder; OR = odds ratio; CI = confidence interval; ED = eating disorder.
a Not applicable due to lack of comorbid diagnosis in ED category.
b Includes child and adolescent onset.
c Includes current and partial remission diagnoses.
d Includes unspecified bipolar and related disorder.
Children with BED showed higher odds of past MDD, PD, separation anxiety disorder, social anxiety disorder, specific phobia, GAD, OCD, PTSD, ADHD, and sleep problems. They also showed higher odds of current MDD, GAD, specific phobia, OCD, CD, ODD, bipolar disorder, and ADHD.
Children with any binge eating showed higher odds of past MDD, PD, separation anxiety disorder, social anxiety disorder, specific phobia, GAD, OCD, PTSD, bipolar disorder, ADHD, and sleep problems as well as current MDD, separation anxiety disorder, social anxiety disorder, specific phobia, GAD, OCD, CD, ODD, bipolar disorder, and ADHD.
Discussion
Results suggest associations between EDs and psychiatric morbidity, particularly BED and any binge eating. AN was generally associated with less comorbidity, with lower comorbidities than prior data in adolescents. 6 Given that 99.9% of children met subthreshold AN criteria, it is possible that psychiatric morbidity increases as AN progresses or across development. Consistent with previous research, BN, BED, and binge eating were associated with elevated psychiatric comorbidity. 6 Few children met full-/subthreshold BN criteria, which limited the ability to find associations; however, BN was highly associated with current/past PD and OCD and past PTSD. BED and any binge eating were associated with a wide range of current/past psychiatric disorders. Aligned with prior nationally representative data in adolescents, 9 there were associations between current ADHD and higher odds of all EDs.
While this study furthers research on psychiatric comorbidity of childhood EDs across internalizing and externalizing disorders as well as current and past diagnoses, there are several limitations. Limitations include cross-sectional assessment of current and past psychiatric disorders, self-report of diagnoses by parents only, reduced ability to generalize findings to international samples, and not assessing avoidant restrictive food intake disorder. Findings mostly converge with the adult and child literature by finding elevated psychiatric comorbidity in EDs, particularly in EDs characterized by binge eating 2,6 and strengthen the argument for a developmental perspective on psychiatric disorders. Comorbid psychopathology represents a key factor to consider in future studies of early EDs. Future research should examine causal mechanisms of EDs and psychiatric disorders in preadolescent children.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_07067437211026485 - Psychiatric Comorbidity Associated with Eating Disorders in 9- to 10-year-old Children
Supplemental Material, sj-docx-1-cpa-10.1177_07067437211026485 for Psychiatric Comorbidity Associated with Eating Disorders in 9- to 10-year-old Children by Tyler B. Mason and Kathryn E. Smith in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Author Contributions
Dr. Mason and Dr. Smith conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants K01DK124435 from the National Institutes of Health (National Institute of Diabetes and Digestive and Kidney Diseases).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.