
Abstract
Background
Globally, post-menopausal osteoporosis poses a major health challenge, primarily affecting elderly women because of its connection to lowered bone mineral density and increased susceptibility to fractures. This skeletal disorder not only compromises the quality of life but also contributes to a substantial socio-economic and healthcare burden.
Purpose
We examined the efficacy of bavachin, a plant-derived flavonoid estrogen mimic, in mitigating osteoporosis in ovariectomized Wistar rats.
Materials and Methods
Osteoporotic conditions were established through bilateral ovariectomy (OVX), followed by treatment with bavachin. An additional OVX group received alendronate, a standard anti-osteoporotic drug, to serve as a reference for comparative efficacy. Critical molecular markers reflecting bone metabolism, such as osteocalcin, C-terminal telopeptide of type I collagen, alkaline phosphatase, and acid phosphatase, were quantified. Bone microarchitecture was examined using micro-computed tomography, while biomechanical strength was evaluated through a three-point bending test. Serum calcium and phosphorus levels were measured to examine bavachin’s influence on mineral homeostasis. Oxidative stress and inflammatory responses were analyzed by determining antioxidant enzyme activity and pro-inflammatory cytokine concentrations. Furthermore, the expression of bone remodeling regulators, such as osteoprotegerin (OPG), receptor activator of nuclear factor κB ligand (RANKL), osterix (Osx), and runt-related transcription factor 2 (Runx2), was examined in treated and untreated OVX rats.
Results
Bavachin treatment attenuated oxidative stress and inflammation, while improving bone turnover markers and mechanical properties. A decrease in RANKL expression and an upregulation of OPG, Osx, and Runx2 suggest that bavachin effectively modulates bone remodeling pathways and inhibits osteoclast-mediated bone resorption.
Conclusion
Our findings demonstrate that bavachin exhibits significant anti-osteoporotic activity and may serve as a promising and safer alternative to conventional osteoporosis therapies.
Keywords
Introduction
Osteoporosis is a globally prevalent metabolic bone disorder, affecting approximately 19.7% of the population, with pronounced variability across regions and ethnic groups (Sözen et al., 2017; Xiao et al., 2022). It is especially common among post-menopausal women due to a multifaceted interplay of risk factors such as age, sex, hormonal shifts during menopause, and unhealthy lifestyle (Bijelic et al., 2017). Central to its pathogenesis is estrogen deficiency, which disrupts the balance of bone remodeling by decreasing osteoblastic activity and enhancing osteoclastic resorption, thereby accelerating bone loss. Early menarche and premature menopause further amplify vulnerability by prolonging estrogen insufficiency (Mishra et al., 2017; Muñoz et al., 2020). Statistically, women are over twice as likely as men to develop osteoporosis, with risk escalating with age (Alswat, 2017; De Martinis et al., 2021). Clinically, osteoporotic fractures, particularly of the spine, hip, and wrist, are among the most debilitating conditions, leading to heightened morbidity, mortality, and long-term disability (Khan et al., 2024; LeBoff et al., 2022).
Osteoporosis treatment primarily involves the use of anti-resorptive and anabolic drugs to address the imbalance between the catabolic and anabolic phases of bone metabolism (Li et al., 2021). Bisphosphonates remain the most widely used drugs, with newer formulations allowing less frequent dosing (Fuggle et al., 2022). Other anti-resorptive options include selective estrogen receptor modulators and calcitonin. Parathyroid hormone analogs are the main anabolic agents available in the USA and Europe. Emerging therapies include denosumab, a monoclonal antibody inhibitor, and drugs targeting the Wnt/β-catenin pathway (Kim et al., 2021). Despite their efficacy, these medications can have side effects. Close monitoring is essential when using drugs like denosumab and teriparatide due to potential side effects (Hirooka et al., 2020). Bisphosphonates, in particular, may cause severe adverse reactions in some patients, necessitating alternative treatments (Ganesan et al., 2025; Jara et al., 2022).
Phytoestrogens, a group of plant-derived compounds exhibiting estrogen-like activity, have garnered attention as potential therapeutic agents for managing post-menopausal osteoporosis. Structurally analogous to 17β-estradiol, these compounds, particularly isoflavones, lignans, and coumarins, can bind to estrogen receptors and modulate estrogenic signaling pathways (Chavda et al., 2024; Lagari & Levis, 2013; Wang et al., 2020). Among them, genistein, daidzein, and equol demonstrate notable efficacy in promoting osteoblast-mediated bone formation while concurrently inhibiting osteoclast-driven bone resorption (Strong et al., 2014). Dietary sources such as soy and flaxseed are rich in isoflavones and lignans, respectively (Arjmandi, 2001). The bone-protective effects of phytoestrogens are mediated through diverse molecular mechanisms, including modulation of the RANKL/RANK/OPG axis and regulation of apoptosis (Setchell & Lydeking-Olsen, 2003). Such compounds exhibit protective effects against bone loss, contribute to increased bone mineral content, and help reduce the incidence of fractures due to osteoporosis (Kaczmarski et al., 2025). Given their natural origin and favorable safety profile, phytoestrogens present a promising non-hormonal alternative to conventional hormone replacement therapy, particularly for individuals concerned about estrogen-associated malignancies (Arjmandi, 2001).
Bavachin, a naturally occurring phytoestrogen derived from Psoralea corylifolia, exhibits a broad spectrum of pharmacological activities, including nephroprotective (Luo et al., 2025), anti-inflammatory (Hung et al., 2019), anti-hepatosteatotic (Wei et al., 2023), and anti-tumor (Yang et al., 2025) effects. Functioning as a partial agonist of estrogen receptors, it binds to and activates both ERα and ERβ, albeit with relatively low potency (Park et al., 2012). Notably, bavachin exerts strong anti-inflammation property by suppressing the IKK/IκBα/NF-κB signaling cascade in chondrocytes, suggesting a protective role against osteoarthritic degeneration (Cheng et al., 2010). Beyond its estrogenic and anti-inflammatory properties, research suggests that bavachin exerts anti-cancer, anti-bacterial, and lipid-lowering effects. Its multifaceted pharmacological profile indicates therapeutic efficacy in the management of numerous complications, including cardiovascular disorders, diabetes mellitus, and neurodegenerative diseases (Patel, 2022). In this study, we analyzed the efficacy of bavachin in mitigating osteoporosis induced by ovariectomy in an animal model.
Materials and Methods
Animals
Twelve-week-old female Wistar rats, weighing approximately 200–250 g, were housed in a controlled environment with a temperature of 20°C ± 2°C, relative humidity of 50%–60%, and a 12-h light/dark cycle. They had unrestricted access to standard chow and water. A 1-week acclimation period was observed before beginning the experimental procedures. All animal experiments and handling procedures received approval from the institutional ethics committee and complied with established standards for the humane treatment and management of laboratory animals.
Osteoporosis Induction
Osteoporosis was induced in the rats via performing ovariectomy following a previously established protocol of Lelovas et al. (2008). Anesthesia was induced in the animals through intraperitoneal administration of pentobarbital sodium at a dosage of 50 mg/kg body weight. A dorsal incision was made to access the ovaries, and the overlying musculature and skin were carefully dissected. The surrounding adipose tissue was excised to expose the ovarian tissue. The junction between the fallopian tube and the uterine horn was ligated, and a small incision was made to excise the ovary. In the sham-operated control (SHAM) group, the same surgical procedure was performed without exposing or removing the ovarian tissue. Throughout the surgical procedure, the vital signs of all rats were continuously monitored to prevent any complications or mortality.
Experimental Design
After a 1-week acclimation period to laboratory conditions, the rats were randomly assigned into different experimental clusters using a computer-generated randomization scheme. Group I served as the SHAM, comprising animals that underwent a mock surgery without ovary removal. Group II included ovariectomized rats, which were kept for 3 weeks prior to undergoing bilateral ovariectomy to induce estrogen deficiency. Group III consisted of OVX rats administered bavachin orally at a dosage of 10 mg/kg body weight per day for a total of 16 weeks. Group IV involved OVX rats treated daily with alendronate at a dose of 2.5 mg/kg body weight over the same 16-week period. At the end of the experimental timeline, all animals were humanely sacrificed, and whole blood was collected via cardiac puncture. The blood samples were left to clot at room temperature for 30 min, and then the serum was separated through centrifugation at 1,500 × g for 10 min. Following blood collection, the femur bones were dissected, fixed in 10% formaldehyde, and preserved at –20°C for further analysis.
Assessment of Biochemical Bone Turnover Marker
To evaluate bavachin’s efficacy on bone remodeling, biochemical indicators of bone turnover were analyzed in the ovariectomized animal model. Serum levels of osteocalcin (OC) and C-terminal telopeptide of type I collagen (β-CTX) were measured using enzyme-linked immunosorbent assay (ELISA) kits obtained from MyBiosource and Novus Biologicals, respectively. Enzymatic activities of alkaline phosphatase (ALP) and acid phosphatase (ACP) were evaluated using colorimetric assay kits provided by Elabscience. All assays were carried out in strict accordance with the protocols recommended by the respective manufacturers.
Assessment of Bone Microarchitecture
Following the treatment period, the rats were euthanized to evaluate the extent of osteoporotic bone loss triggered by ovariectomy and to assess the potential protective effects of bavachin. The right femur from each animal was carefully excised. The distal end of the femur was preserved in neutral buffered methanol, rinsed thoroughly in running water, and subsequently stored in 75% ethanol to maintain tissue integrity. Micro-computed tomography (micro-CT) scans were performed using the following parameters: 70 kV voltage, 114 µA current, with a spatial resolution of 10 µm. Quantitative analysis of the trabecular architecture was conducted within a predefined region of interest, extracting various three-dimensional structural indices, including bone volume fraction (BV/TV), trabecular number (Tb.N), trabecular separation (Tb.Sp), trabecular thickness (Tb.Th), structure model index (SMI), and connectivity density (Conn.Dn). To eliminate bias, the individual conducting the imaging analysis was blinded to the treatment groups throughout the assessment.
Assessment of Biomechanical Strength
The mechanical strength of the right femur was evaluated using a three-point bending test during the procedure. Each femur was carefully placed on a specialized support platform with two fixed points spaced 2.0 cm apart, maintaining the bone’s natural anatomical curvature. A controlled force was applied to the mid-diaphyseal region at a steady rate of 2 mm/min until fracture occurred. From the resulting load-displacement data, key mechanical parameters such as maximum load, stiffness, and energy absorption were determined. Furthermore, material characteristics, including ultimate stress, toughness, and elastic modulus, were calculated from the same curve to thoroughly assess the bone’s structural performance (Zhang et al., 2018).
Estimation of Calcium and Phosphate
Serum levels of calcium and phosphate in both ovariectomized untreated and bavachin-treated rats were quantified utilizing commercially available colorimetric assay kits obtained from Sigma–Aldrich. The procedures were executed following the protocols recommended by the manufacturer.
Assessment of Oxidative Stress
To evaluate the oxidative stress resulting from ovariectomy and the potential protective effects of bavachin, various antioxidant parameters were analyzed in the experimental animals. Catalase (CAT) activity was assessed spectrophoto-metrically by tracking the breakdown of hydrogen peroxide at 240 nm in a reaction mixture comprising tissue supernatant, hydrogen peroxide, and phosphate buffer, following the method of Aebi (1984). Glutathione peroxidase (GPx) activity was determined through a coupled assay measuring nicotinamide adenine dinucleotide phosphate (NADPH) consumption at 340 nm, where the enzymatic reduction of hydrogen peroxide by glutathione (GSH) is linked to NADPH oxidation in the presence of glutathione reductase (GR) (Paglia & Valentine, 1967). GR activity was quantified by monitoring the rate of NADPH oxidation at 340 nm during the conversion of oxidized glutathione (GSSG) back to its reduced form (GSH), based on the protocol by Carlberg and Mannervik (1985). GR levels were estimated using the DTNB method, wherein GSH reacts with DTNB to form a yellow-colored product measured at 412 nm, as described by Anderson (1985).
To assess lipid peroxidation and oxidative damage, the thiobarbituric acid reactive substances (TBARS) assay was employed. In this method, tissue or serum samples were incubated with TBA reagent in a boiling water bath for 15–30 min, followed by cooling and centrifugation. The absorbance of the resulting supernatant was read at 532 nm to determine malondialdehyde (MDA) levels, an indicator of lipid peroxidation (Ohkawa et al., 1979). All biochemical assays were carried out using appropriate standard curves and control samples
Assessment of Inflammatory Cytokines
The concentrations of pro-inflammatory cytokines, including interleukin-1β (IL-1β), Interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α), were quantified in serum samples from ovariectomized untreated and bavachin-treated rats using ELISA kits procured from Abcam. The assays were conducted in accordance with the manufacturer’s standardized protocol, which involved the incubation of samples with cytokine-specific capture antibodies, followed by the addition of enzyme-linked detection antibodies. Colorimetric detection was achieved through substrate conversion, and the absorbance was measured to determine cytokine levels, reflecting the extent of analyte binding.
Assessment of Bone Remodeling Regulators
To evaluate the modulatory effects of Bavachin on bone remodeling in ovariectomized rats, the levels of key regulators, including osteoprotegerin (OPG), receptor activator of nuclear factor κB ligand (RANKL), runt-related transcription factor 2 (Runx2), and osterix (Osx), were quantified using ELISA kits obtained from Elabscience. All assays were conducted as per the guidelines outlined in the kit manuals, strictly adhering to the manufacturer’s instructions.
Statistical Analysis
Results are presented as mean values ± standard deviation (SD). Statistical comparisons between groups were conducted using one-way analysis of variance (ANOVA) with SPSS software version 26.0 (USA). Graphs were created using GraphPad Prism version 8 (USA). A p value less than .05 was regarded as indicative of statistical significance
Results
Flavonoid Bavachin Attenuated Bone Turnover Markers in Ovariectomized-rats
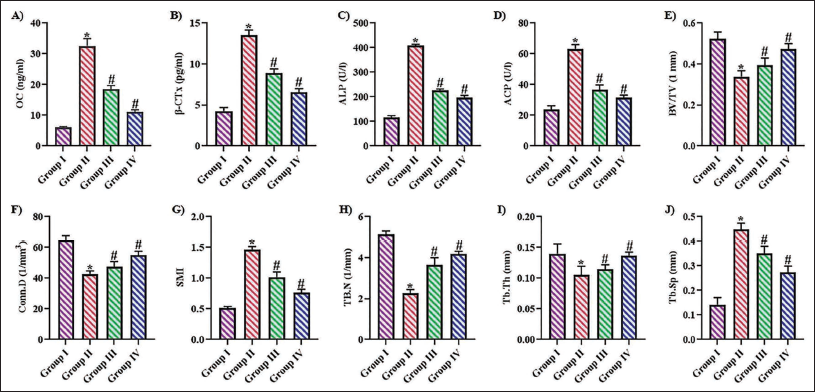
Figure 1A–1D illustrates the levels of biochemical markers of bone turnover in ovariectomized untreated and bavachin-treated animals. Ovariectomy resulted in a significant elevation of OC and β-CTX levels, reaching 28.4 ± 0.0006 ng/mL and 13.5 ± 0.0005 pg/mL, respectively, compared to control rats, which exhibited levels of 6.8 ± 0.0002 ng/mL and 2.7 ± 0.0004 pg/mL. Treatment with bavachin and the anti-osteoporotic agent alendronate significantly (p < .05) attenuated these elevated markers in ovariectomized rats, with bavachin-treated animals showing OC levels of 15.5 ± 0.0001 ng/mL and β-CTX levels of 7.5 ± 0.0008 pg/mL, levels comparable to those observed in the alendronate-treated group (OC: 9.8 ± 0.0004 ng/mL; β-CTX: 4.8 ± 0.0006 pg/mL). Both bavachin and alendronate treatments also significantly (p < .05) reduced serum ALP levels to 195 ± 4.5 U/L and 178 ± 4.5 U/L, respectively, as well as ACP levels to 32 ± 0.007 U/L and 28 ± 0.008 U/L, respectively. The ovariectomized untreated rats exhibited significantly increased levels of ALP (387 ± 7.5 U/L) and ACP (56 ± 0.009 U/L), whereas the control rats exhibited significantly decreased levels of ALP (110 ± 1.5 U/L) and ACP (18 ± 0.006 U/L).
Flavonoid Bavachin Attenuated Bone Turnover Markers and Preserved Bone Microarchitecture in OVX- rats. (A) Osteocalcin, (B) C-terminal Telopeptide of Type I Collagen, (C) Alkaline Phosphatase, (D) Acid Phosphatase, (E) Bone Volume Fraction, (F) Connectivity Density, (G) Structure Model Index, (H) Trabecular Number, (I) Trabecular Thickness, and (J) Trabecular Separation Levels in the SHAM Operated, Ovariectomized Untreated, Ovariectomized Treated with Bavachin, Ovariectomized Treated with Standard Anti-osteoporotic Drug Alendronate. Values are Reported as Mean ± Standard Deviation (SD), with Statistical Significance Set at p < .05.
Flavonoid Bavachin Preserved Bone Microarchitecture in Ovariectomized-rats
The influence of bavachin on the bone microarchitecture of ovariectomized rats was assessed using micro-CT analysis, and the observations were depicted in Figure 1E–1J. Ovariectomy resulted in a significant reduction in Tb.N and trabecular thickness compared to both drug-treated and control groups. Administration of bavachin and alendronate markedly increased these parameters, indicating improved trabecular microstructure. Additionally, ovariectomy led to a substantial decrease in both BV/TV and Conn.Dn, whereas treatment with bavachin and alendronate significantly (p < .05) enhanced these structural indices. Bavachin treatment also reduced Tb.Sp and decreased the SMI, suggesting a shift toward more plate-like and mechanically robust bone architecture. In contrast, untreated ovariectomized rats exhibited significantly elevated SMI and Tb.Sp, indicative of degraded microarchitecture.
Flavonoid Bavachin Enhanced Biomechanical Strength in Ovariectomized-rats
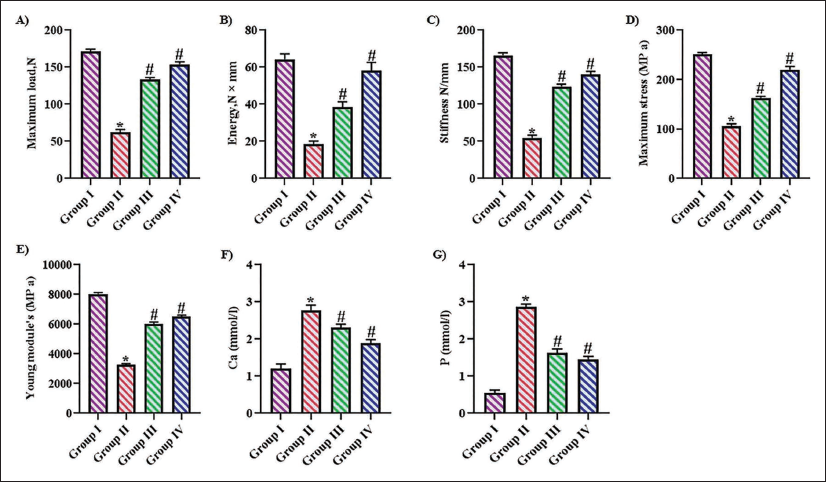
The biomechanical strength of the femurs in bavachin-treated and untreated ovariectomized rats was evaluated using a three-point bending test, with the results shown in Figure 2A–2E. Ovariectomy led to a significant reduction in maximum load and stress-bearing capacity compared to all other experimental groups. Treatment with bavachin and alendronate significantly (p < .05) improved these biomechanical parameters in ovariectomized rats. Additionally, both stiffness and Young’s modulus were markedly decreased in untreated ovariectomized rats. It also increased the energy levels in the ovariectomized animals.
Flavonoid Bavachin Enhanced Biomechanical Strength and Reduced Serum Calcium and Phosphorus Levels in OVX-rats. The Bone Biomechanical Strength and Serum Mineral Contents of Bavachin-treated and Untreated Ovariectomized Rats were Assessed, and the Results were Illustrated in Figure 2. (A) Maximum Load, (B) Maximum Stress, (C) Stiffness, (D) Energy, (E) Young’s Module, (F) Serum Calcium, and (G) Serum Phosphorus Measurements in the SHAM Operated, Ovariectomized Untreated, Ovariectomized Treated with Bavachin, Ovariectomized Treated with Standard Anti-osteoporotic Drug Alendronate. Values are Reported as Mean ± Standard Deviation (SD), with Statistical Significance Set at p < .05.
Flavonoid Bavachin Elevated Serum Calcium and Phosphate Levels in Ovariectomized-rats
Calcium and phosphate levels, which were critical components in bone metabolism, were quantified in bavachin-treated and untreated ovariectomized rats, as depicted in Figure 2F and 2G. Ovariectomy caused a significant decline in serum calcium (2.7 ± 0.0008 mmol/L) and phosphate (2.9 ± 0.00004 mmol/L) levels compared to control rats, which exhibited levels of 1.2 ± 0.0003 mmol/L and 0.4 ± 0.00005 mmol/L, respectively. Treatment with bavachin and alendronate significantly (p < .05) ameliorated these deficits, with calcium levels rising to 1.8 ± 0.0007 mmol/L and 1.5 ± 0.0005 mmol/L, and phosphate levels increasing to 1.6 ± 0.00007 mmol/L and 1.1 ± 0.00003 mmol/L, respectively, in ovariectomized rats.
Flavonoid Bavachin Mitigated Oxidative Stress in Ovariectomized-rats
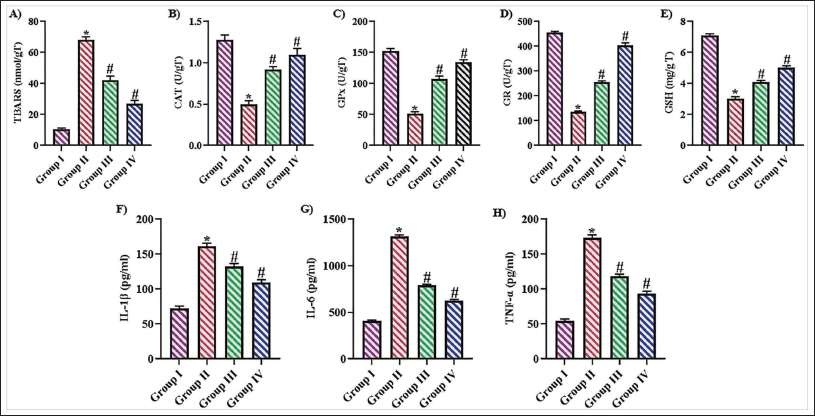
The antioxidative effects of bavachin in ovariectomized rats were evaluated by measuring various antioxidant enzyme activities and oxidative stress markers, as shown in Figure 3A–3E. Ovariectomy markedly induced oxidative stress, as shown by enhanced levels of TBARS and a significant decline in the activities CAT, GPx, and GR. Additionally, levels of reduced GSH were significantly decreased following ovariectomy. Treatment with bavachin and alendronate significantly (p < .05) restored antioxidant enzyme activities, reduced TBARS levels, and elevated GSH levels in ovariectomized rats.
Flavonoid Bavachin Mitigated Oxidative Stress and Inflammation in OVX-rats. (A) Thiobarbituric Acid Reactive Substances, (B) Catalase, (C) Glutathione Peroxidase, (D) Glutathione Reductase, (E) Reduced Glutathione, (F) Interleukin-1 Beta, (G) Interleukin-6, and (H) Tumor Necrosis Factor-alpha Levels in the SHAM Operated, Ovariectomized Untreated, Ovariectomized Treated with Bavachin, Ovariectomized Treated with Standard Anti-osteoporotic Drug Alendronate. Values are Reported as Mean ± Standard Deviation (SD), with Statistical Significance Set at p < .05.
Flavonoid Bavachin Suppressed Pro-inflammatory Cytokine Levels in Ovariectomized-rats
Figures 3F–H illustrate pro-inflammatory cytokine levels in bavachin-treated and untreated ovariectomized rats. Ovariectomy triggered a decline in IL-1β and IL-6, with respective concentrations of 154.0 ± 0.09 pg/mL and 1340 ± 8.5 pg/mL. Treatment with bavachin and alendronate markedly (p < .05) reduced these cytokine levels to 126.0 ± 0.04 pg/mL and 98.0 ± 0.03 pg/mL for IL-1β, and 755 ± 1.5 pg/mL and 615 ± 2.8 pg/mL for IL-6, respectively. Moreover, TNF-α levels decreased from 165.0 ± 1.5 pg/mL in ovariectomized untreated rats to 132.0 ± 0.5 pg/mL and 74.0 ± 0.5 pg/mL following bavachin and alendronate treatment. Control rats exhibited significantly lower cytokine levels, with IL-1β at 60.0 ± 0.04 pg/mL, IL-6 at 320.0 ± 3.5 pg/mL, and TNF-α at 48.0 ± 0.7 pg/mL.
Flavonoid Bavachin Modulated Bone Remodeling Markers in Ovariectomized-rats
Figure 4 illustrates the impact of bavachin and alendronate on bone metabolism markers in OVX animals. Ovariectomy significantly reduced OPG, a decoy receptor that prevents RANKL-mediated osteoclast activation, and markedly elevated RANKL levels (260 ± 8 pg/mL and 85 ± 0.0007 pg/mL, respectively). Treatment with bavachin and alendronate reversed these effects, increasing OPG levels (920 ± 11 pg/mL and 1010 ± 8 pg/mL, respectively) and decreasing RANKL (65 ± 0.0005 pg/mL and 45 ± 0.0004 pg/mL, respectively). Furthermore, both compounds enhanced osteogenic transcription factors Runx2 and Osx, essential for osteoblast differentiation; Runx2 levels rose to 8.5 ± 0.0003 pg/mL and 12 ± 0.0009 pg/mL, and Osx to 8.5 ± 0.0003 pg/mL and 12 ± 0.0009 pg/mL with bavachin and alendronate, respectively. Compared to all experimental groups, control rats exhibited the most favorable bone profile, with significantly higher OPG (1,350 ± 10 pg/mL), Runx2 (18 ± 0.0007 pg/mL), and Osx (13.8 ± 0.0009 pg/mL) levels, along with lower RANKL expression (22 ± 0.0003 pg/mL).
Flavonoid Bavachin Modulated Bone Remodeling Markers in OVX-rats. (A) Osteoprotegerin, (B) Receptor Activator of Nuclear Factor κB Ligand, (C) Runt-related Transcription Factor 2, (D) Osterix Levels in the SHAM Operated, Ovariectomized Untreated, Ovariectomized Treated with Bavachin, Ovariectomized Treated with Standard Anti-osteoporotic Drug Alendronate. Values are Reported as Mean ± Standard Deviation (SD), with Statistical Significance Set at p < .05.

Discussion
The onset of post-menopausal osteoporosis is mainly attributed to a decline in estrogen levels, which affects bone remodeling through multiple mechanisms. Estrogen deficiency leads to accelerated bone loss, particularly in cancellous bone, and causes continuous bone turnover in both women and men (Armas & Recker, 2012; Riggs et al., 1998). Both natural and surgical menopause result in comparable decreases in bone mineral density after 3 years (Ohta et al., 1994). Surgically induced menopause may lead to more intense metabolic alterations, favoring the earlier onset of osteoporosis (Pavel et al., 2016). It directly impacts bone cell activity and mediates osteoimmunity, involving various immune cells such as T cells, B cells, and macrophages (Yao et al., 2025). Estrogen deficiency increases IL-7 production, activating T-cells and promoting osteoclastogenesis through increased RANKL and TNF production (Cenci et al., 2000). In rheumatoid arthritis, estrogen deficiency exacerbates bone loss by causing immune dysregulation, particularly in ACPA-positive patients. This leads to an increase in pro-inflammatory cytokines such as TNFα and IL-17, which enhance bone resorption while suppressing bone formation (Xu et al., 2022). The present study investigated the impact of the phytoestrogen bavachin on osteoporosis induced by ovariectomy.
Bone turnover markers are increasingly utilized to assess bone remodeling activity and track treatment outcomes in osteoporosis. They offer dynamic insights into bone health, either independently or alongside BMD measurements (Kim et al., 2006; Vasikaran et al., 2011). Evidence suggests that elevated bone resorption markers combined with low femoral BMD are more predictive of fractures than low BMD alone (Vasikaran, 2008). Additionally, recent research indicates that higher BTM levels are linked to a greater risk of osteoporotic fractures, regardless of BMD status (Hlaing & Compston, 2014). Therefore, we quantified the bone turnover markers, osteocalcin, β-CTX, ALP, and ACP in the experimental animals to evaluate the therapeutic efficacy of bavachin in OVX rats.
OC plays a twin role by reflecting bone generation and correlating with skeletal muscle mass and fall risk in post-menopausal women. Its responsiveness to estrogen levels and nutritional interventions further highlights its utility as both a biomarker and a therapeutic indicator (Kuo & Chen, 2017; Lee et al., 2007; Vitale et al., 2021). Conversely, β-CTX, a degradation product of type I collagen, act as a reliable marker for bone catabolism, which is linked to decreased bone mass and muscle function, as well as increased Tb.Sp, especially in menopausal populations (Chubb & Vasikaran, 2017). β-CTX also serves a key function in assessing the efficacy of anti-resorptive therapies, establishing it as a benchmark for clinical follow-up (Jiang et al., 2023). ALP, while commonly used to assess liver and bone health, demonstrates strong associations with bone mineral content and treatment outcomes in osteoporosis. Notably, reductions in ALP levels have been observed in response to bisphosphonate therapy, reinforcing its clinical relevance (Fink et al., 2016; Kyd et al., 1998). Tartrate-resistant ACP serves as a specific indicator of osteoclastic activity and is elevated in conditions like post-menopausal osteoporosis and Paget’s disease (Bull et al., 2002; Hannon et al., 2004). Bavachin-treated rats exhibited decreased bone turnover markers compared to the untreated OVX rats, indicating its potent inhibitory effect on estrogen deficiency-induced bone resorption. The reduction in serum calcium and phosphate levels in bavachin-treated OVX rats aligns with the observed decrease in bone turnover activity.
Oxidative stress, driven by estrogen deficiency and ageing, is a critical factor in post-menopausal osteoporosis (Giorgio et al., 2007; Mohamad et al., 2020). Estrogen loss impairs mitochondrial β-oxidation of fatty acids, elevating reactive oxygen species (ROS) such as H2O2, particularly in hepatic mitochondria and peroxisomes, while concurrently reducing antioxidant enzyme activities (Oliveira et al., 2018). Excess ROS promotes osteoclast-mediated bone resorption through regulated free radical production, whereas osteoblasts counteract oxidative stress via antioxidants like GPx (Sontakke & Tare, 2002; Zhou et al., 2016). GSH contributes substantially to redox homeostasis by donating electrons to neutralize ROS, facilitating osteogenic differentiation through upregulation of collagen I, OC, and ALP (Wang et al., 2022). GSH deficiency impairs GPx4 function, enhancing lipid peroxidation and ferroptosis via Fe²+-catalyzed reactions (Gaschler et al., 2018). Meta-analytical data confirm elevated oxidative biomarkers and diminished antioxidant defenses in osteoporotic post-menopausal women. Natural antioxidants exhibit therapeutic potential by inhibiting osteoclastogenesis and promoting osteoblast activity and bone matrix synthesis (Austermann et al., 2019; Domazetovic et al., 2020; Marcucci et al., 2023). Given the critical role of antioxidant defense in counteracting estrogen deficiency-induced oxidative damage, we examined the bavachin effect on oxidative stress in ovariectomized (OVX) rats. Bavachin treatment significantly enhanced antioxidant enzyme activities and effectively attenuated oxidative stress, indicating its potential in restoring redox balance and mitigating osteoporosis-associated bone deterioration.
The immune system significantly contributes to the development of post-menopausal osteoporosis, primarily through estrogen deficiency-induced inflammation (Iantomasi et al., 2023; Saxena et al., 2021). The decline in estrogen levels fosters a persistent low-grade inflammatory state, elevating proinflammatory cytokines and chemokines that disrupt bone cell activity (Inada & Miyaura, 2010). Estrogen normally modulates immune cell behavior, and its absence leads to heightened levels of inflammatory stimulators (Cohen-Solal et al., 1993; Zheng et al., 1997). These cytokines have been detected in both peripheral circulation and the bone microenvironment of post-menopausal women, correlating with increased bone resorption (Romas & Martin, 1997). Notably, IL-1 elevation has been shown to be reversible with estrogen therapy (Pacifici et al., 1989; Rogers & Eastell, 1998). In our study, Bavachin treatment not only scavenged oxidative stress but also significantly suppressed the synthesis of inflammatory-stimulating cytokines in the OVX rats.
Estrogen exerts its effects on bone largely through modulation of the OPG/RANKL/RANK pathway, which is central to osteoclast regulation (Almeida et al., 2013; Lacey et al., 1998). RANKL, a cytokine vital for osteoclast formation and function, is secreted by stromal cells, activated T cells, and B cells (Simonet et al., 1997). It binds to RANK receptors on osteoclasts and their precursors, promoting bone resorption (Li et al., 2000). OPG, a soluble receptor, competes with RANK for RANKL binding, thereby inhibiting osteoclastogenesis (Kong et al., 1999). These three molecules RANKL, RANK, and OPG are indispensable for osteoclast biology, as evidenced by animal studies; the absence of RANK or RANKL results in osteopetrosis, while the lack of OPG leads to severe bone loss (Streicher et al., 2017). Sex hormones, particularly estrogen, directly enhance OPG expression and indirectly influence RANKL levels, as demonstrated in vitro and in animal models where removal of gonads increases RANKL expression in bone (Bord et al., 2003; Saika et al., 2001). Therapeutically, blocking RANKL with denosumab, a monoclonal antibody, effectively reduces bone resorption and is widely used in managing osteoporosis (Fukumoto & Matsumoto, 2017; Kawai et al., 2011). More recently, romosozumab, targeting sclerostin, a Wnt pathway inhibitor that also stimulates RANKL, has been introduced, promoting bone formation and reducing resorption by inhibiting sclerostin activity (Mullard, 2019; Wijenayaka et al., 2011). Bavachin treatment significantly decreased the RANKL expression and increased the OPG levels, thereby promoting osteoblastogenesis in OVX rats.
Bavachin treatment also enhanced the key osteogenic transcription factors, Runx2 and Osx, both essential for bone matrix formation. Runx2 initiates osteoblast lineage commitment, while Osx, acting downstream, is critical for osteoblast maturation (Komori, 2006; Nakashima et al., 2002). Estrogen loss induces oxidative stress and inflammation, which suppresses the expression of Runx2/Osx and reduces bone formation (Almeida et al., 2007). While RANKL signaling primarily promotes osteoclastogenesis, it indirectly affects osteoblasts by increasing pro-inflammatory cytokines, which can inhibit Runx2 transcriptional activity (Boyle et al., 2003; Weitzmann & Pacifici, 2006). Natural antioxidants have shown the ability to counteract these effects by restoring Runx2/Osx expression and supporting osteoblast function under oxidative stress (Bai et al., 2005; Domazetovic et al., 2020). In our study, bavachin treatment significantly attenuated RANKL and increased the expression of Runx2/Osx.
The anti-osteoporotic efficacy of bavachin in OVX rats was confirmed with our micro-CT analysis and three-point bending test. Our micro-CT analysis and three-point bending test revealed significant deterioration in trabecular bone architecture following ovariectomy. Treatment with bavachin effectively reversed these structural impairments, restoring trabecular microarchitecture to near-normal levels via inhibiting OPG/RANKL signaling pathway. This suggests that bavachin enhances trabecular connectivity and promotes a biomechanically superior, plate-like trabecular structure, which correlated with our other biochemical results. In addition, our study has several limitations that should be acknowledged. One major limitation is the species difference between rats and humans, which may affect the translatability of our findings. Additionally, the treatment duration was relatively short, and the long-term effects of bavachin on bone health remain unknown. Furthermore, our study lacked long-term follow-up, which is essential for assessing the sustainability of bavachin’s osteoprotective effects. These limitations highlight the need for further studies to be conducted in the future. In our future studies, we plan to address these limitations by conducting experiments with longer treatment durations and follow-up periods, as well as exploring the efficacy of bavachin in other species, including humans. By addressing these limitations, we aim to provide a more comprehensive understanding of bavachin’s therapeutic potential for osteoporosis. In terms of translational relevance, bavachin’s development as a dietary supplement or pharmacological agent holds promise, but several challenges need to be addressed. These include formulation challenges, such as optimizing bioavailability and stability, as well as regulatory hurdles. Additionally, further studies are needed to confirm bavachin’s efficacy and safety in humans. Future research should also investigate optimal dosing regimens and potential interactions with other medications. By addressing these challenges and uncertainties, we can further explore bavachin’s therapeutic potential for osteoporosis.
Conclusion
Overall, the findings of this study suggest compelling evidence that bavachin, a flavonoid-based phytoestrogen, exerts notable osteoprotective effects in an ovariectomy-induced model of post-menopausal osteoporosis. Bavachin significantly improved bone microarchitecture, enhanced biomechanical strength, and favorably modulated biochemical markers of bone turnover. Its ability to attenuate oxidative stress and inflammatory responses, alongside the regulation of key bone remodeling genes, namely, downregulation of RANKL and upregulation of OPG, Osx, and Runx2, underscores its dual anti-resorptive and anabolic potential. These findings prove that bavachin may be a viable, naturally derived therapeutic candidate for treating post-menopausal osteoporosis, warranting further investigation in clinical settings to validate its efficacy and safety profile.
Abbreviations
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This work was approved by the Institutional Ethical Committee of Huanggang Central Hospital of Yangtze University, Huanggang, Hubei, China.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
NA.