
Abstract
Background
Type 2 diabetes mellitus (T2DM) is characterized by insulin resistance and impaired glucose metabolism, leading to hyperglycemia and increased risk of complications like renal fibrosis.
Objectives
This study’s purpose is to examine how berberine hydrochloride (BBR) and metformin (Met) work together to treat T2DM, as well as how these medications affect tissue type metalloproteinase-1 (TIMP-1), glucose, and lipid metabolism levels in the blood and transforming growth factor β1.
Materials and Methods
Using a random number table approach, overall, 100 individuals with T2DM between October 2020 and October 2022 were chosen and classified into two groups: An experimental group and an untreated group, each with 50 patients. The untreated group received Met therapy, whereas the experimental group received BBR based on the untreated group. The two groups were compared regarding efficacy, cholesterol and glucose metabolism, renal function and renal fibrosis indices, and the frequency of adverse responses.
Results
The experimental group’s effective rate was 96.00% higher than that of the untreated group (82.00%). Following treatment, the experimental group had lower levels of glycosylated hemoglobin (HbAlc), insulin resistance index (HOMA-IR), fasting blood glucose (FBG), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), and cholesterol (TC) than the untreated group, while the untreated group had greater levels of high-density lipoprotein cholesterol (HDL-C). Following the course of therapy, the observation group’s levels of cystatin (Cys-C), urinary β2 microglobulin (β2-MG), urine albumin excretion rate (UAER), and urinary microalbumin (ALB) were all lesser compared to the untreated group. Following treatment, the experimental group’s transforming growth factor-β (TGF-β) levels, matrix metalloproteinase-9 (MMP-9), and TIMP-1 were lesser than those of the untreated group.
Conclusion
When Met and BBR are taken together, patients with type 2 diabetes can effectively control their glucose and lipid metabolism, as well as their levels of TGF-β1, MMP-9, and TIMP-1. They can also postpone renal interstitial fibrosis and eventually improve their kidney function, all with a high degree of safety and significant effects.
Introduction
The primary characteristics of type 2 diabetes mellitus (T2DM), a metabolic disease interacting with environmental factors and genetics, are abnormalities in the metabolism of fats and carbohydrates. Its primary pathophysiology involves insulin resistance (IR) and an absolute or relative deficit of islet beta cells. IR affects the body’s glucose and lipid metabolism problems and is linked to the development of related issues brought on by the disease’s continued aggravation (Harrison et al., 2021; Zhang et al., 2020). Because of changes in living conditions and lifestyle, the number of persons with diabetes in our nation has been increasing annually in recent years (Wang et al., 2022).
Early blood glucose management, averting acute and chronic problems, and enhancing the function of insulin receptors and islet β cells can effectively manage the progression of diabetes and enhance patient outcomes (Harrison et al., 2021; Wang et al., 2022). Everyone knows that the most essential and basic treatment for type 2 diabetes patients to maintain stable blood sugar levels is a long-term, sustainable, and healthy lifestyle (Xu et al., 2021). Research has indicated that a nutritious diet, particularly the Mediterranean diet, together with different fasting protocols, a low glycemic index diet, and a balanced diet, can effectively regulate caloric intake, enhance blood sugar and lipid levels, preserve insulin secretion, lessen abdominal obesity, and ultimately improve IR (Xie et al., 2022). However, it can be challenging to break long-standing poor eating habits in the near term, and the hunger in fasting, blood sugar, cholesterol, and other metabolic markers vary, leading to weight regain after retaliatory overeating and significantly decreasing scientific diet compliance (Xie et al., 2022; Xu et al., 2021).
For blood sugar control, medication therapy in conjunction with food modification and exercise therapy remains the most successful approach. Met, the most fundamental first-line medication for T2DM, has been used extensively in clinics for a long time. Because of its shown efficacy and safety, it holds a significant place in both domestic and international guidelines (Habtemariam, 2020). Commonly referred to as “berberine,” berberine hydrochloride (BBR) is an isoquinoline alkaloid extracted from Coptis chinensis. It is an inexpensive medication that is effective in detoxifying, clearing heat, regulating intestinal flora, and having a broad spectrum of antibacterial activity that can either kill or inhibit a variety of gram-positive and gram-negative bacteria as well as fungi. Due to its ability to alleviate the symptoms of diarrhea, it is frequently utilized in clinics (Och et al., 2022). However, several studies conducted recently have demonstrated that BBR also has a significant role in enhancing blood lipids, blood sugar, and immune regulation (Habtemariam, 2020; Och et al., 2022). Using diabetic rats as test subjects, some research has eventually determined that BBR can enhance the phosphatidylinositol 3 kinase (PI3-K)’s glucose transporter 4 (GLUT4) expression and increase GLUT4’s circulation rate in the body, both of which improve IR (Habtemariam, 2020; Liang et al., 2019; Och et al., 2022). Unfortunately, there is a dearth of convincing data from extensive clinical experimental research, and these investigations are mostly based on animal experiments. Based on this, the effort aims to screen for the effects of BBR plus Met on glucose and lipid metabolism, serum TIMP-1, and TGF-β1 in T2DM patients, as well as the efficacy of this combination.
Materials and Methods
General Data
Using the random number table method, a total of 100 T2DM patients between October 2020 and October 2022 were selected, with 50 patients in each group, and divided into experimental and untreated groups. There were 26 females and 24 males in the experimental group. Age range: 41–76 years, mean (61.32 ± 6.42) years; average (7.81 ± 0.73) years of diabetes duration (2–15 years). Overall, 25 males and 25 females were in the untreated group. Age range: 43–79 years, mean (63.05 ± 6.87) years; average (7.21 ± 0.65) years; duration of diabetes: 1–14 years. The general data did not significantly differ among the two groups (p > 0.05).
Inclusion and Exclusion Criteria
Inclusion criteria: (a) Age: Adult patients under 80 years of age, irrespective of gender or ethnicity. Based on the Chinese Guidelines for the Prevention and Treatment of Type 2 Diabetes (2017 edition), a definitive diagnosis of T2DM was established. (b) The patient’s medical records are complete. (c) Give your free will and sign an informed consent form.
Exclusion criteria: (a) Gestational diabetes mellitus, Type 1 diabetes mellitus, or specific type diabetes mellitus. (b) There are serious complications of diabetes, such as severe infection or diabetic ketoacidosis (DKA). (c) Severe hepatic and renal dysfunction: Liver enzyme levels thrice greater compared to the upper limit of normal (specifically ALT or AST), blood creatinine levels above 2.0 mg/dL (176.8 µmol/L), or glomerular filtration rate <45 mL/min. (d) Other diseases that affect glycolipid-related indicators such as hypercortisolism, hyperthyroidism, or hypothyroidism. (e) Severe gastrointestinal discomfort or related diseases. (f) Use of drugs that may affect the study within the first 3 months of enrollment, including any drugs and hormones that affect blood sugar other than Met. (g) Pregnant or lactating women. (h) Follow-up is not expected to be completed under other circumstances.
Methods
Both the groups were given diabetes education, moderate exercise, diet control, and a high-quality low-protein diabetes diet. The untreated group was given Met hypoglycemic treatment with a daily dose of 1,000–2,000 mg. The experimental group was given BBR treatment according to the untreated group: 0.5 g orally three times a day. If gastrointestinal intolerance occurred, the oral dose was adjusted to 0.3 g each time, and the Met dose remained unchanged.
Observational Index
Therapeutic Effect
Obvious effect: The patient’s clinical symptoms have disappeared. The urinary protein quantity of 24 h was <0.5 5 g or more than 2/3, and the blood creatinine was reduced by more than 1/4. (b) Effective: Patients with reduced clinical symptoms, 24 h urinary protein quantity decreased by more than 1/3, patients with renal function improved but not yet reached the obvious effect standard or stable. (c) Ineffective: The patient’s clinical symptoms do not improve or even worsen, and the indicators do not meet the effective standards.
Blood Index
3 mL peripheral venous blood and 5 mL urine samples were taken before and after treatment. (a) Glucose and lipid metabolism: HbA1c, fasting blood glucose (FPG), fasting insulin (Fins), and insulin resistance index (HOMA-IR) levels = Fins/22.5 × FBG were measured. Serum triglyceride (TG), cholesterol (TC), high-density, and low-density lipoprotein cholesterol (HDL-C, LDL-C) levels were measured. (b) Renal function: The levels of serum cystatin (Cys-C), urinary microalbumin (ALB), urinary β2 microglobulin (β2-mg), and urinary albumin excretion rate (UAER) were detected. (c) The kidney fiber index: By enzyme-linked immunosorbent assay to detect matrix metalloproteinase 9 (MMP-9), transforming growth factor beta (TGF-beta), matrix metalloproteinases inhibitor-1 (TIMP-1) level.
Adverse Drug Reaction (ADR)
Compare the prevalence of ADR during treatment among the two groups.
Statistical Analysis
The statistical program SPSS 23.0 was employed for data analysis. The measured data were provided as mean ± standard deviation (x ± s), the t-test was employed to compare the two groups, the χ2 test was employed to show the adoption rate of the measured data, and p < 0.05 represented that the variation was statistically significant.
Results
A Comparison of the Two Groups’ Clinical Efficacy
Table 1 illustrates that the experimental group’s treatment effective rate was 96.00% greater than the untreated group’s (p < 0.05).
Clinical Efficacy Comparison Between the Two Groups.

Comparison of the Two Groups’ Lipid and Glucose Metabolism
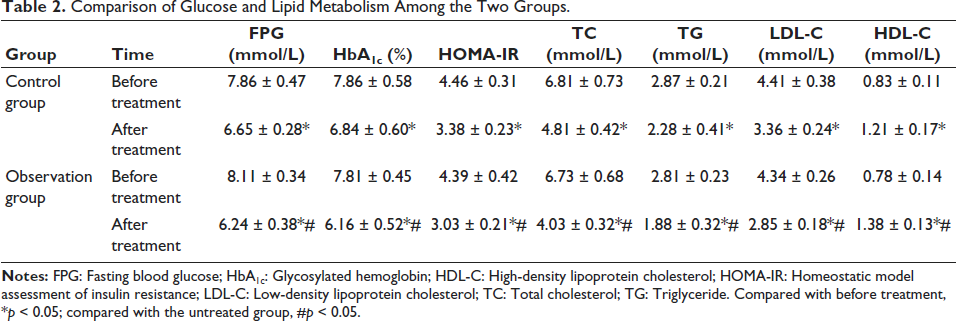
Before therapy, there was a lack of discernible variation among the two groups’ lipid and glucose metabolism (p > 0.05). Following treatment, both groups’ blood levels of FPG, HbAlc, and HOMA-IR were lower than pretreatment (p < 0.05), and the experimental group’s levels were lower than those of the untreated group. Following the intervention, both groups’ serum levels of TC, TG, and LDL-C were lower than they were prior to treatment; additionally, the experimental group’s levels were lesser compared to those of the untreated group, and the experimental group’s levels of HDL-C were higher than those of the untreated group (p < 0.05) (Table 2).
Comparison of Glucose and Lipid Metabolism Among the Two Groups.
Renal Function Index Comparison Between the Two Groups
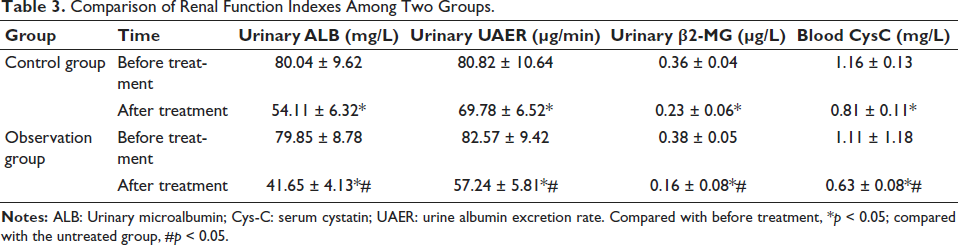
Before therapy, there was a lack of discernible variation in the renal function indices among the two groups (p > 0.05). Following therapy, there was a decrease in blood CysC, urine ALB, UAER, and β2-MG levels in both groups compared to pretreatment values, with a remarkable variation between the experimental and untreated groups (p < 0.05) (Table 3).
Comparison of Renal Function Indexes Among Two Groups.
Renal Fibrosis Index Comparison Between the Two Groups
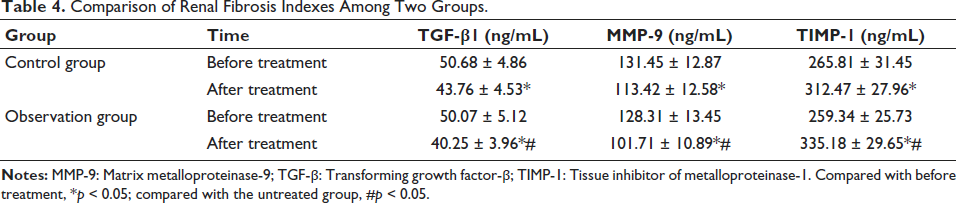
Prior to treatment, there was no discernible difference in TGF-β1, MMP-9, or TIMP-1 levels between the two groups (p > 0.05). Following therapy, both groups’ blood levels of MMP-9 and TGF-β1 were lower than they were prior to treatment, with the experiment group having lower levels than the untreated group. TIMP-1 levels were higher than they were prior to treatment, with the experiment group having higher levels than the untreated group (p < 0.05) (Table 4).
Comparison of Renal Fibrosis Indexes Among Two Groups.
Comparison of the Two Groups’ Adverse Reactions
Patients in the experimental and untreated groups underwent pre- and posttreatment testing for three routine tests during the clinical treatment: an electrocardiogram, liver function, and renal function. No obvious abnormalities, drug toxicity, or side effects were discovered.
Discussion
With the change in unhealthy lifestyles, such as sitting down, staying up late, and eating a high-fat diet, metabolic diseases such as T2DM have skyrocketed in developing countries. Based on the International Diabetes Federation Diabetes Atlas, approximately 400 million people worldwide have T2DM, and 10 million people are diagnosed with diabetes yearly (Liang et al., 2019; Och et al., 2022). With the prolonged course of T2DM, insulin secretion function decreases and IR persists, resulting in hyperglycemia toxicity, which can lead to fatal and disabling diabetic chronic complications such as diabetic retinopathy, kidney disease, cardiovascular and cerebrovascular diseases, which is not good for the patient’s physical and mental health, seriously decreases the life’s quality, and enhances the economic burden of patients and their families as well as society (Liang et al., 2019; Zhang et al., 2019).
Metformin (Met) was introduced into the clinic 60 years ago, and its discovery dates back to the 17th century when it was used to relieve the intense urination of medieval diabetes. At present, Met plays a significant part in many diabetes guidelines at home and abroad (Zhang et al., 2019). Many guidelines recommend that Met be recommended for patients with obesity or normal BMI and no obvious abnormalities in renal function. If combination drugs are required, one of them should include Met (Chen et al., 2023). Recently, more studies have proved that Met can be applied to other diseases, such as obesity, hyperlipidemia, and tumors (Chen et al., 2023; Zhang et al., 2022). BBR is an isoquinoline alkaloid commonly isolated from plants and was originally used to treat diarrhea and dysentery. So far, BBR has not only been used to treat diarrhea but also has been used as an OTC drug in the clinic to treat stomatitis and hepatitis (Cortez-Navarrete et al., 2023; Zhang et al., 2022). In recent years, many studies have confirmed that BBR is effective in the treatment of hyperglycemia, hypertension, and hyperlipidemia, and can also assist in cardiovascular diseases, hyperuricemia treatment, and other clinical effects (Araj-Khodaei et al., 2023; Cortez-Navarrete et al., 2023; Zhang et al., 2022). Although much research has shown that the hypoglycemic effect of BBR is similar to that of Met, it has not been widely used in diabetes treatment.
In this work, the effective rate of treatment in the experimental group was greater compared to that in the untreated group, representing that BBR combined with Met can further enhance the clinical symptoms of patients and improve clinical efficacy. In addition, in the pretreatment of this study, the FPG, HbAlc, and HOMA-IR levels in the untreated group were lesser compared to before treatment, which may be related to the hypoglycemic mechanism of Met. In the BBR combined with the Met treatment group, the above indexes decreased significantly, and the degree of decline was better than that of Met monotherapy, suggesting that BBR has a definite hypoglycemic effect. Previous studies have confirmed that BBR has the same or better effect than Met in reducing FBG in diabetic rats (Pei et al., 2019). The mechanism of BBR hypoglycemia may have the following aspects: (a) It can activate glucagon-like peptide 1 (GLP-1) receptor in pancreatic beta cells, increase insulin receptor expression, further activate AMPK and PI-3K pathway, and increase glucose transport and utilization in peripheral tissues (Araj-Khodaei et al., 2023; Cortez-Navarrete et al., 2023). (b) The expression of insulin receptor mRNA can be increased through upregulation of protein kinase C (PKC) (Araj-Khodaei et al., 2023). (c) BBR can activate GLUT1-mediated glucose uptake by 3T3-L1 adipocytes via EPK and AMPK pathways (Pei et al., 2019). (d) Suppression of multiple transcription factors leads to inhibition of gluconeogenesis of two rate-limiting enzymes, glucose-6-phosphatase and phosphoenolpyruvate carboxykinase (Di et al., 2021). BBR reduces blood sugar levels by reducing glucose production and increasing glucose uptake, transport, and utilization. BBR monotherapy in treating T2DM still has limitations, and its efficacy and safety lack a large sample of randomized controlled clinical studies. The combination of BBR and Met is an economical and effective alternative hypoglycemic program, worthy of clinical promotion (Di et al., 2021; Pei et al., 2019; Wang et al., 2021).
Abdominal obesity and excessive visceral fat, as the soil and core of IR, increase the risk of T2DM and play a significant role in the pathogenesis of T2DM (Nematollahi et al., 2022). This research showed that BBR combined with Met could enhance the TC, TG, LDL-C, and HDL-C levels in patients in addition to improving IR and hypoglycemia. In terms of lipid-lowering mechanism, BBR varies from statins in that it can upregulate LDLR expression by stabilizing LDLR message ribonucleic acid (mRNA) and suppressing the transcription of pre-protein converting enzyme (PCSK-9) (Nematollahi et al., 2022; Wu et al., 2021; Xu et al., 2020). Meanwhile, BBR can also activate the AMPK-SIRT1-PPARα pathway. Inhibition of macrophage expression of lectin-like oxidized low-density lipoprotein receptor-1 (Lox-1) reduces the formation of foam cells (Wu et al., 2021; Xu et al., 2020). In addition, BBR can also reduce TG by activating AMPK and blocking the MAPK/ERK pathway, which can decrease the translocation of the nucleus and the binding activity of the NF-κB pathway activated by LPS (Xu et al., 2020). Presently, preliminary animal and human trials have shown that BBR can improve the lipid profile. A large study pointed out that BBR can reduce LDL, TC, and TG in patients with dyslipidemia, which is compatible with the results (Khater et al., 2023; Senesi et al., 2021).
The kidney is the nature of congenital, and the main essence, the main water, and the main gas, T2DM patients with kidney disease dysfunction, blood stasis, phlegm turbidness, water, and other pathological products formation, kidney deficiency caused by kidney essence loss in storage, proteinuria, and a series of symptoms, if early detection and timely treatment of patients with renal damage can effectively enhance the prognosis of patients (Ai et al., 2021; He et al., 2022; Senesi et al., 2021). Serum CysC can reflect the state of ultra-early renal function with high sensitivity and specificity. In addition, urine β2-MG, UAER, and ALB are markers of renal function injury (Noh et al., 2022; Shinjyo et al., 2020). The study found that BBR can enhance the level of kidney function in T2DM patients with kidney disease (Noh et al., 2022). In this study, urinary ALB, UAER, β2-MG, and blood CysC levels in the posttreatment experimental group were lesser compared to those in the untreated group, indicating that BBR can effectively reduce ALB and improve renal function in patients, which is consistent with the above findings. Further comparison of renal fibrosis indexes among the two groups pre- and posttreatment showed that among many MMP family members, MMP-9 could degrade renal basement membrane collagen and other cellular matrix, which was most correlated with the occurrence of T2DM complicated kidney disease (Mi et al., 2019; Shrivastava et al., 2023). TIMP is a natural specific inhibitor of MMPs, which can interact with the active site of MMPs and prevent the interaction between MMPs and substrate. Among them, TIMP-l can inhibit the degradation of MMP-9, decrease the expression of MMP-9, or increase the TIMP-1 expression (Mi et al., 2019; Xuan et al., 2020). Both can cause MMP-9/TIMP-1 dysregulation and accelerate glomerular sclerosis (Xuan et al., 2020). TGF-β1 in renal tissue is secreted by glomerular and tubular epithelial cells. In the occurrence and development of T2DM with renal disease, a variety of factors promote the abnormal increase of TGF-β1 expression and stimulate the synthesis of collagen and other cell matrix components (Yao et al., 2020; Zhao et al., 2021). In this study, serum levels of MMP-9 and TGF-β1 decreased and TIMP-l increased in the two groups after treatment, and the effect of the experimental group was better compared to that of the untreated group, indicating that BBR combined with Met can further prevent glomerular sclerosis, delay renal interstitial fibrosis, and improve renal function by regulating the cellular matrix metabolic system. In the course of treatment, no serious ADR occurred in the two groups, indicating that BBR combined with Met treatment is safe.
Conclusion
BBR combined with Met can effectively regulate the glucose and lipid metabolism of type 2 diabetes patients, regulate the TGF-β1, MMP-9, and TIMP-1 levels, delay renal interstitial fibrosis, and enhance kidney function, with significant effects and high safety.
Abbreviations
ALB: Urinary microalbumin; β2-MG: Urinary β2 microglobulin; BBR: Berberine hydrochloride; Cys-C: Cystatin C; FBG: Fasting blood glucose; GLUT4: Glucose transporter 4; HbA1c: Glycosylated hemoglobin; HDL-C: High-density lipoprotein cholesterol; HOMA-IR: Homeostatic model assessment of insulin resistance; IR: Insulin resistance; LDL-C: Low-density lipoprotein cholesterol; Met: Metformin; MMP-9: Matrix metalloproteinase-9; T2DM: Type 2 diabetes mellitus; TC: Total cholesterol; TG: Triglyceride; TGF-β: Transforming growth factor-β; TIMP-1: Tissue inhibitor of metalloproteinase-1; UAER: Urine albumin excretion rate.
Footnotes
Acknowledgments
The authors thank the anonymous reviewers and editors who helped improve the article.
Authors Contributions
Weichen Yan designed the study. Yun Jie and Yongwei Zhang wrote the original draft. Weichen Yan supervised the study. All authors read and approved the final version of the manuscript.
Availability of Data and Materials
The data could be obtained by contacting the corresponding author.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study protocol was approved by the Ethics Committee of the Fifth People’s Hospital of Hainan Province (No. 20190712HN). Informed consent was obtained from all patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.