
Abstract
Background
Parkinson’s disease (PD) is the second most common neurodegenerative disorder with cognitive impairment as a prime non-motor symptom. Biomarkers can assist in detecting cognitive impairment, which normally follows movement dysfunction, and also assist in the differentiation of PD patients with and without cognitive dysfunction, facilitating the early diagnosis and disease management while also allowing for timely therapeutic intervention.
Summary
Here, we have reviewed the biomarkers of Parkinson’s disease from different sources i.e., body fluids (CSF, blood, salivary, urine and tear) and tissues (gut and skin), along with the techniques used for the detection of these biomarkers. We further discuss the importance of biomarker validation and the significance of cohort studies in biomarker discoveries.
Key Message
The chapter is aimed at updating the knowhow of the disease biomarkers that may assist differentiation of these overlapping entities.
Introduction
Amongst the common age-related multifactorial neurodegenerative disorders, Parkinson’s disease (PD) follows Alzheimer’s disease, per their worldwide prevalence. 1 It is primarily characterised by the death of the dopamine synthesising neurons, localised in the substantia nigra pars compacta (SNpc) 2 accompanied by the development of Lewy bodies. 3 Although 16%–36% of the PD cases harbour a risk of heritability, the majority of them are idiopathic. 4 Approximately 5%–15% of patients carry mutations in the glucocerebrosidase A (GBA), 5 thus rendering it an important genetic risk factor for the disease. Other genetic risk factors include the leucine-rich repeat kinase 2 gene (LRRK2), PARK2 (Parkin) and α-synuclein (SNCA). 6
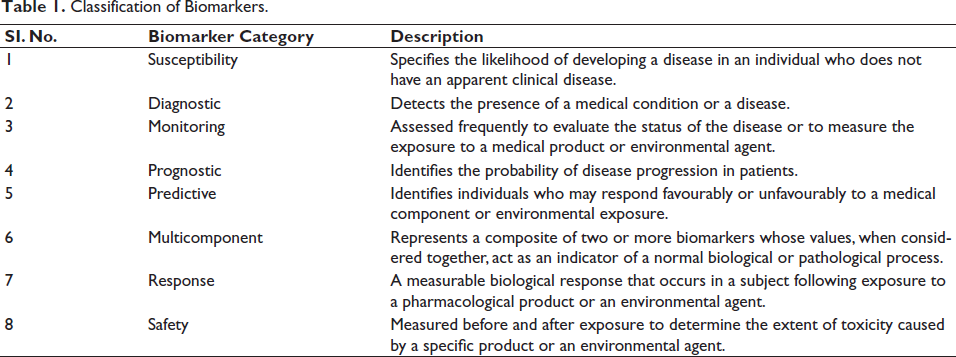
The motor symptoms of this disorder comprise tremor, rigidity, bradykinesia, as well as postural instability, attributable to the death of dopaminergic neurons, while the non-motor manifestations include anxiety or depression, cognitive impairment, sleep disturbances and autonomic dysfunctions 7 ; as the indelible consequences of degeneration on the serotonergic, noradrenergic and cholinergic systems. 8 Several studies have identified cognitive impairment as the most widespread symptom of PD. The severity varies from mild cognitive impairment (MCI) in 25.8% cases to severe dementia (24%–31%).9–11 The prodromal symptoms emerge more than a decade ahead of the motor deficits. Hence, identifying biomarkers would facilitate an early diagnosis and aid disease management while also allowing for timely therapeutic intervention. A biomarker refers to a subset of accurately and reproducibly measurable medical signs. These signs are considered unbiased and reliable indicators of the medical state of the patient Table 1. 12
Classification of Biomarkers.
Sources of Biomarkers
Clinical biomarkers like tremor, rigidity and bradykinesia are common clinical symptoms to identify and monitor the disease; while features like REM sleep behaviour disorder (RBD), constipation, and so on occur in the prodromal stage. 13 PD being a multifactorial syndrome, identifying biomarkers from genetic, structure-based, biochemical and clinical sources promise assistance in enhancing the sensitivity and specificity of disease prediction. Neuroimaging techniques like magnetic resonance imaging (MRI), positron-emission tomography (PET) and so on assist the identification of nigrostriatal neurodegeneration. 14 A considerable number of studies have focused on different tissues or body fluid-resident biomolecules to aid disease prediction as well as monitor the progression. 15 Genetic markers are reliable tools to predict the onset of familial or early onset of PD. 6
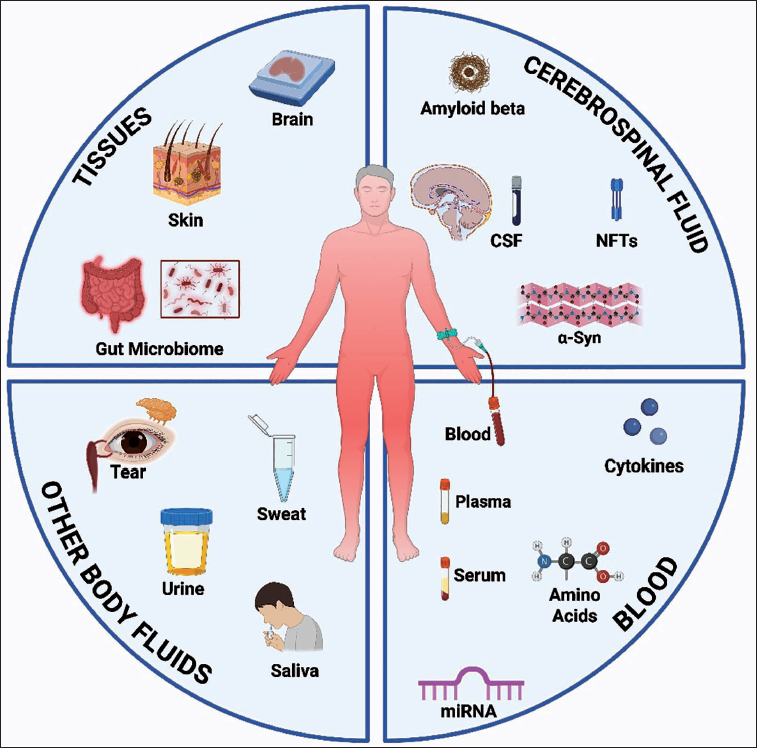
Body Fluid-based Biomarkers (Figure 1)
Cerebrospinal Fluid-based Biomarkers
Although tapping cerebrospinal fluid (CSF) is an invasive procedure, it is an undisputable source for biomarker discovery, by virtue of being in immediate and persistent contact with all the cells in the CNS. The alterations in amyloid-β, Tau, α-synuclein, neurofilament light chain (NfL) and vascular endothelial growth factor (VEGF) are widely studied in PD with dementia, in view of their close association with Alzheimer’s disease, a cognition-centric syndrome. The following section deals with various aspects of biomarker research. Deletions or missense mutations within the gene DJ-1, known as the PD protein 7 (PARK7), are possible candidates for familial onset of the disease. 16
Amyloid β, T-tau, p-tau and α-Synuclein
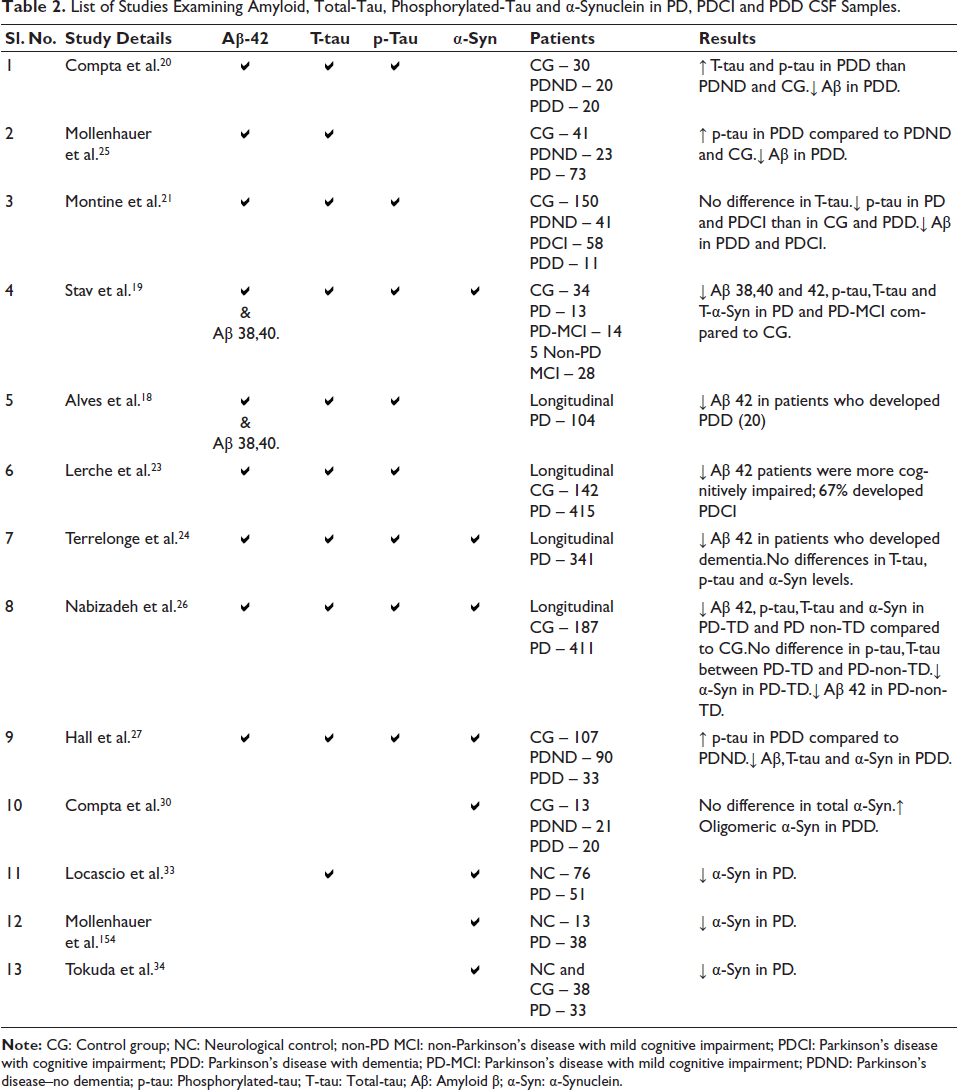
In the PD patients, symptoms manifesting MCI as well as those progressing to dementia (PDD) are often correlated with the occurrence of amyloid-β plaques, Lewy bodies and neurofibrillary tangles in the limbic and neocortical structures.17–19 This led to quantitative investigations on total tau, phosphorylated tau, amyloid-β, as well as α-synuclein in the CSF of PD patients (Table 2). Lower levels of CSF amyloid-β in PD and PD with cognitive impairment vis-à-vis the healthy controls are common notations.19–21 Lower CSF amyloid-β levels indicate the presence of amyloid plaques and are associated with defective verbal learning, poor response inhibition and delayed verbal recall in PD patients. 19 Besides, a correlation exists between CSF Aβ-42:40 levels and reduced inter-hippocampal connectivity in cognitively impaired PD patients, as seen via fMRI studies. 22 While lower CSF-Aβ endorsed a risk of developing cognitive impairment18, 23, 24 p-tau, T-tau levels were less consistent.21, 24–27 Higher CSF T-Tau concentration in parallel with higher CSF lactate levels were correlated with the disease progression 28 via metabolite accumulation due to mitochondrial impairment. 29
List of Studies Examining Amyloid, Total-Tau, Phosphorylated-Tau and α-Synuclein in PD, PDCI and PDD CSF Samples.
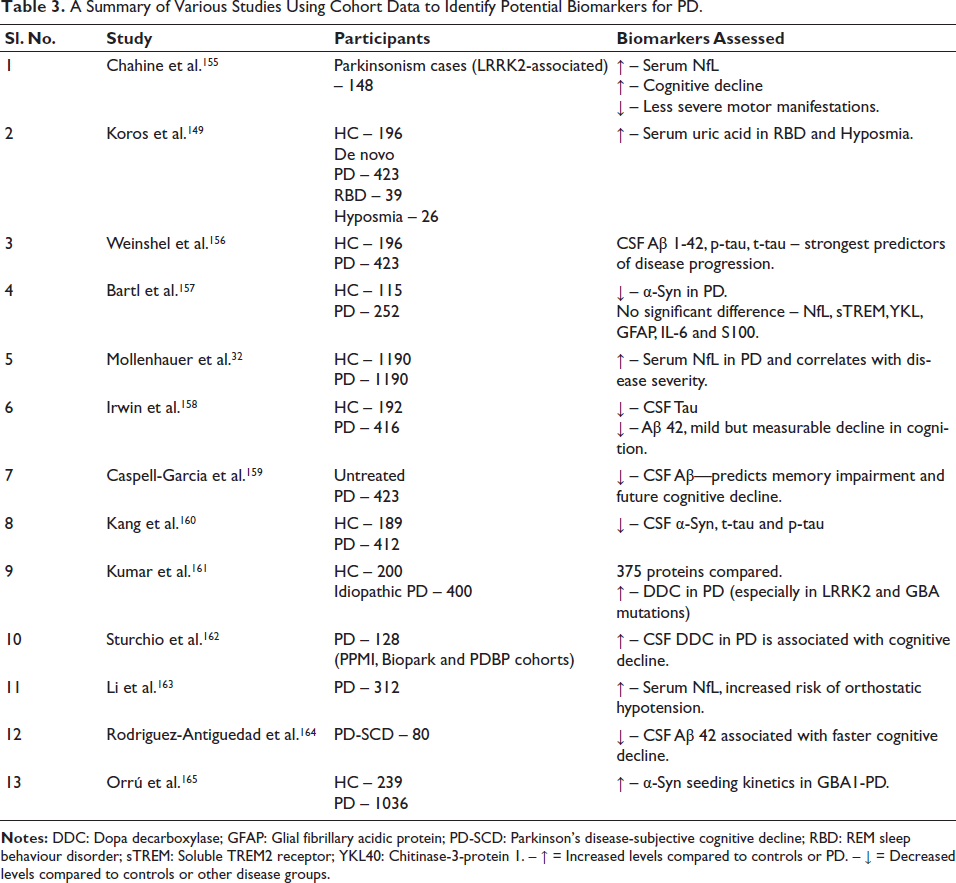
A Summary of Various Studies Using Cohort Data to Identify Potential Biomarkers for PD.
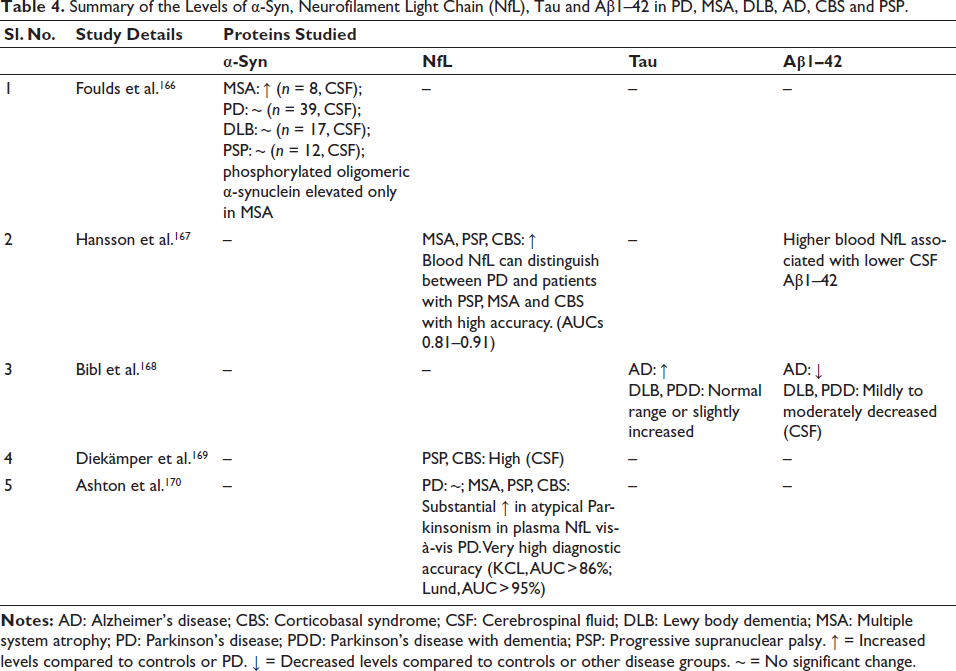
Summary of the Levels of α-Syn, Neurofilament Light Chain (NfL), Tau and Aβ1–42 in PD, MSA, DLB, AD, CBS and PSP.
Lower CSF α-synuclein in PD19,27,30–34 was linked to decreased scores in the composite cognitive domain, executive attention domain and memory and visuospatial domains. 35 Further, the presence of a direct link between testosterone and CSF total α-synuclein in male PD patients, 36 suggests its contribution to central synucleinopathy, while oestrogen may inhibit its pathological aggregation. 37 Thus, hormones may influence male preponderance.
Neurofilament Light Chain
NfL acts as a marker for axonal neurodegeneration, as it is released into the CSF and blood upon neuronal damage. 38 Higher levels in PD were associated with motor and cognitive impairments.39, 40 A longitudinal study 41 further demonstrated a link between higher baseline CSF–NfL levels and enhanced anxiety-related risk during disease progression.
Angiogenic Biomarkers
Angiogenesis is governed by several proteins, including proteins of the VEGF family and their receptors and also placental growth factor (PlGF), Angiopoietin (Ang) family and proinflammatory cytokines such as interleukins. Higher proximity between the melanin-containing neurons and the blood vessels in the SNpc in PD patients was apparently related to glial infiltration, leading to failed neuronal firing and functional degradation. 42
In PD and PD with cognitive impairment, higher levels of CSF-VEGF and PIGF were contrasted by low Ang2. 43 Additionally, the CSF/plasma ratio in PD patients tipped that of controls,43, 44 suggesting a blood-brain barrier breach. 45
Inflammatory Biomarkers
Neuroinflammation is characterised by microglial activation, lymphocyte infiltration and astrogliosis, 46 which is supported by enhancements in levels of interleukins such as interleukin-6 (IL-6), interleukin-1 beta (IL-1β) and interleukin-8 (IL-8)47, 48 in the substantia nigra of PD patients. Higher levels of complement factor H in the CSF of PD patients with cognitive impairment vis-à-vis the controls and PD patients 49 may reflect a compensatory process to downplay the overactivation of the alternate immune pathway. 50
The acute-phase plasma protein, that is, C-reactive protein (CRP), regulates inflammation. 51 Its levels are significantly elevated in the CSF of patients with PD52, 53 and more so in PD patients with dementia. 54 CCL28, a predominant component of the mucosal tissue than the neural cells, bridges the adaptive and innate immune responses by driving the homing of T and B lymphocytes. Its downregulation was classically linked to neuronal loss in PD. 55 Contrarily, in another study, elevated levels in PD-CSF were related to a probable release from the degenerating neurons. 56 Glycoprotein non-metastatic melanoma protein B (GPNMB) induces tissue damage, inflammation, mitochondrial dysfunction and activates the endo-lysosomal pathway.57, 58 Autopsied midbrains of PD patients evidenced a link between activated microglia and elevated levels of GPNMB.58, 59 CSF analysis also showed significantly higher levels with ageing, explaining a compounding effect on motor and cognitive function. 60 Fibrinogen, a glycoprotein predominantly produced by the liver, is converted into fibrin by thrombin to form a blood clot. In aged men, high blood fibrinogen levels were associated with a higher propensity to PD. 61 CSF-fibrinogen was notably elevated in PD patients with cognitive impairment. 48 Animal studies have shown that intraperitoneal injections of fibrinogen can induce Parkinsonian-like features. 62
The proinflammatory proteins interleukin 12B, osteoprotegerin (OPG) and C-X-C motif chemokine ligand 11 (CXCL11) that are linked with T-cell response are decreased in PD. 63 In contrast, the levels of colony-stimulating factor 1, which assists microglial proliferation, were increased.63, 64 Further, the levels of proinflammatory cytokines like tumour necrosis factor alpha (TNF-α), IL-1β, IL-2, IL-4, IL-6 and interferon-γ were significantly higher in the serum of Parkinson’s disease patients.65, 66 Some of these were correlated to pathology in mouse models. 67
Lysosomal Proteins
Functional impairment of the lysosome is a prominent feature in the substantia nigra of PD patients. 68 Deregulated lysosomal autophagy pathway directs abnormal deposition of α-Syn, in vivo. Glucocerebrosidase (GCase) enzyme, encoded by the gene GBA, is down-regulated in several lysosomal storage disorders. GBA also enhances susceptibility to PD. 6 Reduced GBA enzyme activity in Parkinson’s patients, independent of gene mutation, established its association with age. 69 . A corresponding decline in the activities of CSF β-hexaminidase and CSF β-galactosidase in both GBA-PD and sporadic PD patients raises remarkable possibilities. 70
Dihydroxyphenylalanine-decarboxylase
DDC (aromatic
Sleep Biomarkers
Sleep disturbances are the commonest non-motor symptoms of PD, affecting nearly 98% of patients. 74 Longitudinal studies 75 report an association of RBD with rapid declines in global cognition and across multiple cognitive domains (visuospatial ability, verbal episodic memory, language, executive functioning/attention and working memory/processing speed). Excessive daytime sleepiness (EDS) leads to a decline in executive functioning/working memory, verbal episodic memory and attention/processing speed, while insomnia induces greater declines in global cognition and verbal episodic memory.
CSF reflect the direct status of the CNS and hence is considered the most important biofluid for biomarker detection, making the data more credible. However, the CSF-based biomarker research has still not reached its peak potential, due to the possibilities of trauma and contamination related to lumbar puncture.
Other Body Fluids and Biomarker Discovery
Blood-based Biomarkers
Blood-based biomarkers are considered ‘promising for monitoring and management of disease progression’ due to their easy accessibility, time and cost efficiency and simpler processing protocols. Nevertheless, amongst the most promising molecules, that is, α-Syn failed to present consistent findings, with some studies reporting increased total plasma levels, 76 while others suggest a decrease 77 or absence of any differences78–80 between patients and controls. Besides, a cluster of four proteins prominently present in plasma, that is, osteomodulin (OMD) and bone sialoprotein (BSP), was enhanced in PD patient samples, while growth hormone receptor (GHR) and aminoacylase-1 (ACY1) were notably depleted. 81 Blood plasma levels of miRNA-331-5p were significantly upregulated in PD. 82 The gene targets associated with miR-331-5p are the ATM kinase signalling pathway, which regulates PINK1 and Parkin genes. 83 In addition, levels of miR-153, miR-223, miR-15b, miR-185, miR-221 and miR-181a were significantly decreased, while the levels of miR-195, miR-19b-3p were upregulated in blood.82, 84, 85 Discrepancies between expression levels of the miRNA across different studies may be due to the source, that is, serum or plasma.
Lower levels of serum tyrosine and phenylalanine have also been observed in patients with PD. 86 Phenylalanine, an essential amino acid, is hydroxylated by the enzyme phenylalanine hydroxylase to tyrosine, which is subsequently hydroxylated by tyrosine hydroxylase to DOPA, the precursor of dopamine, norepinephrine and epinephrine. Homocysteine (Hcy), a sulphur-containing amino acid, causes neural toxicity and cell death. 87 Elevated levels in the plasma of PD patients,88, 89 more specifically in those with dementia, 90 correlated well with the disease progression. 91 Thus, several proteins implicated in PD pathogenesis are dysregulated in the patient’s blood, raising expectations towards their utility in disease monitoring.
Salivary Biomarkers
Hyper-salivation with diminished clearance resulting in drooling, as well as inadequate and irregular swallowing, are pertinent symptoms of PD. 92 Logical reasoning reckons that collecting saliva samples is a much simpler and non-invasive procedure. Saliva is also more stable than CSF in terms of degradation. The concentrations of α-Syn are similar in saliva and CSF. However, certain difficulties are posited, wherein the production is affected in the early stages of the disease. 93 The ratio of total/oligomeric α-Syn was higher in PD patients, and the total salivary α-Syn was negatively associated with the clinical features. 94 However, another cohort study reported the absence of any differences in the concentrations or any correlation with the motor symptoms of the patients. 80
DJ-1 levels were considerably high in saliva in the advanced stages.95, 96 Further, a mild age-dependent increase was noted in the levels in male patients vis-à-vis the females and the unaffected individuals. 97 The alterations in the sputum of Parkinson’s patients with dysphagia as a comorbidity were in correlation with the UPDRS scores.98–101 Salivary α-amylase, a marker for stress response in humans, is also reduced in PD compared to other neurodegenerative diseases. 102 Amongst two distinct exosomal proteins, L1 cell adhesion molecule (L1CAM) was significantly increased in the saliva of PD patients, accompanied by phospho-α-Synuclein. Its abundance suggests flooding of neuron-derived exosomes in the saliva, indicating the underlying pathological process, since misfolded α-Syn aggregates are often found in saliva-derived exosomes. 103
Microtubule-associated protein light chain 3 beta (MAP-LC3β) is involved in autophagic clearance of aggregated proteins. The higher levels in PD may be a compensatory mechanism, which is validated by a positive correlation between phosphorylated-tau and MAP-LC3β alongside an inverse correlation with TNFα. MAP-LC3β levels correlate inversely with the severity of non-motor symptoms, hinting that impaired autophagy contributes to prodromal signs. 104
Urine-based Biomarkers
A significant decline in urinary filamentous α-Syn has been reported in patients with PD. 105 In addition, the filamentous α-Syn/T-α-Syn ratio was also elevated in the patients. 106 The decrease of salivary DJ-1 is contrasted with an enhancement in the levels in the urine of male patients in an age-dependent manner. 107
Tear Fluid-based Biomarkers
Tears contain proteins secreted by the lacrimal glands. They are modulated by the autonomic nervous system that is majorly affected in PD. 7 Tears are produced in two discrete ways: basal tears, to keep the eye moist and reflex tears in response to irritation and emotions. Most research focuses on reflex tears as they are not significantly affected by aging. The collection is again non-invasive and simple, unlike drawing blood or accessing CSF by lumbar puncture. Significantly higher levels of CCL2 and lactoferrin were demonstrated in the reflex tears of male patients compared to female patients. 108 A few studies have shown significantly higher levels of α-Syn and Nfl in PD patients.109–111 However, the levels of total α-Syn and DJ-1 were not promising. In an interesting turn out, the levels of TNF-α and α-2-Macroglobulin are elevated in patients with PD.111, 112
Autonomic dysfunction may give rise to blepharitis, a manifestation where eyelid glands get clogged and lead to the symptoms of ‘dry eye’. The overall manifestation appears as inflammation of the ocular surface. The blood vessel density in the retina was quantitatively lower in patients at the middle stage (H-Y stage II and III) of the disease compared to those in the early stages (H-Y stage I). 113 They also exhibited lower blink rate and reduced tear production.111, 112 Thus, eyes and tears may offer economical and objective windows for biomarker discoveries.
Solid Tissue Biomarkers
α-Syn gets deposited in a variety of peripheral tissues, that includes skin, colon and olfactory mucosa of patients with PD.112, 114–116 Hence, identification of these deposits could aid the diagnosis of patients living with the disease. Examinations of the gut and skin have provided interesting findings, as discussed in the following section.
Gut Biomarkers
Gut dysfunction is a leading prodromal non-motor symptom of PD. 7 Vagal motor axons in the gut are positive for α-Syn, and these different project to α-Syn immunoreactive neurons present in the myenteric plexus of the gut. 112 This forms the basis for the hypothesis of the disease beginning in the ENS following an infection, and breach in the intestinal mucosa, that subsequently spreads to the CNS via vagal innervations. Evidently, co-occurrence of α-Syn and Lewy bodies in the gastric mucosa ensues during the prodromal stage of the disease.117, 118
It is posited that gut microbiota and their metabolic products may initiate the process of Lewy body formation in the enteric nervous system. PD patients have significantly low levels of enterococci and lactic acid-producing bacteria, with higher levels of Bifidobacterium and Enterobacteriaceae species.119, 120 Additionally, a reduction in short-chain fatty acids (SCFAs) is also reported in early stages of the disease. 119 Increased intestinal permeability in patients with PD 121 coincides with reduced expression of the tight-junction protein—occluding, 122 and elevated expression of proinflammatory cytokines. 123
Skin Biomarkers
Aggregates of α-Syn have been reported in skin and other peripheral tissues as well. Thus, it serves as an accessible peripheral target for biomarker detection. In addition, the phosphorylation index of α-Syn is higher in the patient skin biopsies.115, 124 The gradual age-related increase in α-Syn aggregates in the brain is rated at 9.3% and 12.8%, respectively, in the seventh and eighth decades of life, 125 which supports the age-dependent onset of the disease. Higher p-α-syn deposits in the skin were correlated with lower densities of intraepidermal nerve fibres and higher UPDRS (score III). 126
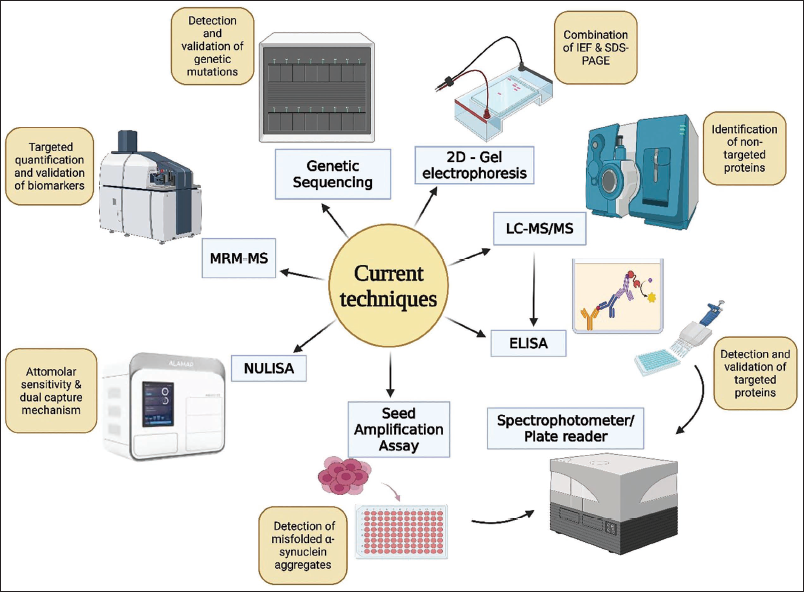
Detection Methods
The search for biomarkers plays a critical role in most areas of biomedical research. With the increasing need to identify biomarkers, several modalities have been developed for reliable and reproducible detection of biomarkers.
2-Dimensional Gel Electrophoresis (Figure 2)
This is one of the oldest and most commonly used techniques for the detection and identification of biomarkers from clinical samples. It combines the principles of isoelectric focusing (IEF) and sodium dodecyl sulphate-polyacrylamide gel electrophoresis. It is thus capable of detecting several proteins from the same gel image. 127 This technique is now restricted to experimental models.
Genetic Testing
Approximately 36% of PD cases are reported to have a genetic origin. 4 The high-risk genetic factors include mutations in GBA, SNCA, LRRK2, PARK7, PINK and PARK2 (PRKN).6, 16 Duplication of the SNCA genes is pathogenic, leading to elevated expression of α-Syn 128 and is associated with the earlier age at onset of the disease and cognitive impairment. Mutations in PARK7, PARK2 and PINK affect the mitochondrial and mitophagy functions, while LRRK2 and GBA affect the lysosomal trafficking pathways. 129 The genetic association of the disease has been extensively covered elsewhere. 4
Targeted and Non-targeted Proteomics
While genomics determines susceptibility-associated genes, proteomics determines the gene products, including the proteins, which are further influenced by the translational control or regulation by post-translational modifications.
Most biomarker-discovery studies are based on the non-targeted approach. The protocol involves non-targeted proteomics, followed by their analytical validation and quantification by targeted proteomics or ELISA. 130 ‘Non-targeted proteomics’ aims to identify/quantify as many proteins present in a sample in a relative manner, which limits the accuracy and precision. Liquid chromatography–mass spectrometry (LC–MS) is a well-established technique for small molecule analysis and forms a crucial component of much of the proteomics-related research. Here, protein mixtures in cell lysates or biofluids are digested by proteases (e.g., trypsin), separated by capillary ‘liquid chromatography’ and then analysed by mass spectrometry. 131 However, LC–MS is favoured for biomarker discovery, while subsequent validation is achieved by high-throughput platforms like MRM-MS/SRM-MS and ELISA. 132
Targeted proteomics is suitable for biomarker verification. Protocols of multiple reaction monitoring MS (MRM-MS) and selected reaction monitoring MS (SRM-MS) offer extensive multiplexing capabilities as well as sensitivity and precision for the quantitation of biomolecules. 133 MRM and SRM analyses are based on rapid fragmentation of peptides, followed by monitoring three to five pre-selected ions. Monitoring a small group of pre-selected ions allows highly sensitive detection of up to nanogram concentrations in a millilitre of a sample. 134 In contrast to MS-based analysis, protein microarrays imprint specific antigens or antibodies on a slide or a membrane to facilitate multiple protein detection by antigen-antibody reaction. 135
Enzyme-linked Immunosorbent Assay
Enzyme-linked immunosorbent assay (ELISA) is based on the principle of antigen-antibody reaction and is a widely used method for targeted protein quantification, yielding good sensitivity. Sensitivity refers to the test’s potential to rightly determine individuals with the disease, while specificity refers to the potential to rightly identify individuals without the disease. 136 Direct ELISA tends to be less sensitive compared to indirect and sandwich ELISA. 137 Despite these advantages, the limitations include a paucity of highly specific antibodies required for the validation of novel proteins. 135
Seed Amplification Assays (Real-time Quaking-induced Conversion)
α-Syn seed amplification assays (SAAs) are being developed as a reliable biomarker diagnostic tool for PD. It is based on the principle of amplification of misfolded protein after repeated sonication. 136 The techniques involve a pre-treatment including shaking and sonication of α-Syn derived from patients to generate α-Syn monomers (seeds), followed by incubation at physiological temperature to promote its aggregation. Fluorescent dyes like Thioflavin T, which bind to amyloid fibrils, are used to detect the quantum of amplification over time. 136 Exceeding a threshold value of 1,000 (Fluorescence units) 137 seed amplification is essential for the ‘test positivity’. SAA shows high sensitivity for PD, and the ‘seed’ can be derived from several sources, including CSF, skin biopsies and blood. 138 The assay was also said to identify the prodromal stage of the disease with 96.2% sensitivity. 139
The potential applications of SAA to accurately distinguish α-synucleinopathies have been widening. α-Syn-SAA can discriminate PD from healthy individuals (70.8% specificity, p < .0001) and tauopathies [CBD (71% specificity) as well as PSP (75% specificity), p < .0001]. 140 Advanced machine learning-based algorithms may assist diagnosis in the future. 141
Nucleic Acid Linked Immuno-sandwich Assay
This technique improves the sensitivity of traditional ligation assays by ~10,000-fold to attomolar concentrations. It suppresses the background via a dual capture and release mechanism by conjugating the oligonucleotide to antibodies. Fully automated nucleic acid-linked immuno-sandwich assay (NULISA) makes broad and in-depth proteomics easily accessible for research and diagnostics. 142
Validation
An increase in protein levels may be due to a compensatory attempt or may be pathogenic in nature, which can be ascertained using experimental models. Validation of the identified biomarkers using animal models is critical, and analysis relies on the assessment of animal behaviour and the histopathological examinations in the related areas like the SNpc, striatum, hippocampal-subicular formation, amygdala and so on. 143 Examples of behavioural assessments include open field studies to assess locomotory behaviour, novel object recognition test for cognition and memory, cylinder test to identify asymmetry, heating pad for nociceptive threshold, gait analysis, rotarod and pole test to assess motor coordination and balance and so on. 49
Clinical Validation of Biomarkers
Following demonstration of the possible utility of the biomarker(s) in detecting and monitoring the disease, implementation at the bedside requires clinical validation. 144 Furthermore, following biomarker discovery, an independent cohort is used to validate the selected biomarkers, and the results are crucial in determining their therapeutic utility. Retrospective or prospective analysis may be performed on a cohort. 145
A large number of independent cohorts have been established for longitudinal studies; however, global cohorts established by the Parkinson’s progression marker initiative (PPMI) and the JPND neurodegenerative disease research BioLoC-PD group are of prime importance as they act as a source for well-characterised samples, for worldwide collaborative research. This is critical, since PD has a highly heterogeneous and multifactorial progression, including the development of severe dementia over time (Table 3). 146
Parkinson’s Progression Marker Initiative Cohort Studies
PPMI is a multicentric, longitudinal and observational study aimed at evaluating the progression of the clinical features through imaging outcomes, biological and genetic markers at all stages of PD across geopolitical boundaries. The overarching aim is to identify progression biomarkers to enhance the treatments available for the disease by bringing together researchers, funders and study participants. The cohort has banked longitudinal data from over 4,000 participants, enrolled at roughly 50 sites across the globe. 147
Cognition-based Studies in Parkinson’s Disease-Parkinson’s Progression Marker Initiative
Siderowf et al. validated the diagnostic performance of SAAs to identify PD using cross-sectional assessment of the participants in the PPMI cohort. Assessments on 1,123 participants (7 July 2010–4 July 2019) exhibited a positive correlation between prodromal and genetic carriers of the disease. 148 It was further evidenced that SAAs classified patients with PD with greater specificity and sensitivity. 5-years long systematic evaluation of serum uric acid in 423 de novo PD patients and 196 controls from the PPMI database showed higher levels in patients with prodromal REM behavioural disorder compared to those without. 149
Assessment of autonomic dysfunction with ‘Scales for Outcomes in PD—SCOPA-AUT’ correlated with disease progression. 150 Essentially, the symptom frequency and the mean scores were obtained from the PPMI database. While comparing a 7-year-long follow-up data of patients and 5-year follow-up data for healthy controls, autonomic dysfunctions, for example, gastrointestinal, urinary, thermoregulatory and sexual dysfunction, appeared to be common during the prodromal stages and worsened with the disease progression (Table 4).
Atypical Parkinsonian Syndromes
In contrast to PD, the atypical Parkinsonian syndrome refers to a more diverse collection of neurodegenerative disorders. 151 Among them, corticobasal syndrome (CBS), Lewy body dementia (LBD), frontotemporal dementia with Parkinsonism (FTD-P), multiple system atrophy (MSA), progressive supranuclear palsy (PSP) and normal pressure hydrocephalus (NPH) are the most prominent subtypes. They account for 5%–10% of the PD population, and in the early stages, patients with APS are frequently misdiagnosed as PD. 152
In our centre, an ongoing longitudinal study aims at the recruitment of approximately 400 de novo patients of MSA, PSP and CBS, in order to understand the mechanisms underlying the pathological protein aggregation and the progression of the disease in the Indian context. 153 Clinical evaluation of motor and non-motor symptoms will be supplemented by assessment of sleep dynamics through polysomnography (PSG) recordings. The leads from non-targeted proteomic analysis of CSF would be followed up by ELISA to validate the proteins in a larger cohort of Asian-Indians, which forms a sizeable part of the world population.
Summary
At present, CSF analysis provides to be the stable source of biomarker studies. Other biofluids requiring less invasive collection procedures, like peripheral blood, tears, saliva, sweat and urine, also need rigorous and widespread validation. A reverse and double blind clinical validation of biomarkers from these sources would pave the way necessary for translational applications and disease management. Since PD is multifactorial, the discovery of more specific biomarkers will help differentiate different subtypes, that is, PD with motor dysfunctions and PD with cognitive and motor dysfunctions, and thus facilitate timely intervention of appropriate therapeutics. Crucial amongst the vitals is the need to identify population-specific biomarkers and if possible individual-centric answers. The heterogeneity observed in PD may be difficult to address in the absence of such concerted efforts.
Footnotes
Acknowledgements
This study was supported by DBT-TATA Innovation Fellowship under grant (number HRD-16012/6/2020-AFS-DBT; 2022-23) and ICMR under grant (number EM/Dev/IG/32/0165/2023) to PAA. RR is a NIMHANS fellow (MsNs202406), and SC is an ICMR Fellow (2021-15115/Proteomics-BMS).
Author’s Contribution
Ragini R.: Conception as well as interpretation of the published research articles to collate and write the 1st draft of the manuscript. Approved the final version of the submitted manuscript and is accountable for all aspects of the article. Shatabdi Choudhury: Conception as well as interpretation of the published research articles and preparation of the 1st draft, including figures using BioRender software. Krithika N.C.: Conception, interpretation of the published research articles and critical revision of the 1st and 2nd drafts of the article. M.M. Srinivas Bharath: Developing the concept and critically revising the 2nd draft of the manuscript for intellectual content. B.L. Sujatha Rathod: Conception and design, as well as critical reviews of the 2nd and final drafts for intellectual content. Ravi Yadav: Developing the concept and critically revising the 2nd draft of the manuscript for intellectual content. Phalguni Anand Alladi: Conception and design of the manuscript and figures. Critically revised the 1st, 2nd and final draft of the article for intellectual content and approved the final version for submission.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not applicable.
Statement of Ethics
An ethical statement is not required.