
Abstract
Background
Brainstem auditory evoked potentials (BAEPs) aid in the diagnosis of probable neurologic disorders of the VIIIth cranial nerve, the associated auditory pathways, and an estimation of hearing sensitivity, for those who are unable to reliably provide information through behavioural hearing evaluations. BAEPs exhibit variabilities due to numerous pathologic and non-pathologic factors. One of the factors that may have a significant impact on typical BAEPs is gender. Although there are numerous studies documenting gender as an influencing factor on auditory evoked potentials in older subjects, there are few comparable studies among subjects who are just entering adulthood.
Objective
The current study aimed to understand the pattern of gender-based differences in BAEPs among emerging adults of Northern India.
Methods
The present study was conducted on 120 normal subjects (70 females, 50 males) who were relatives (second degree) of the patients belonging to Northern India aged between 19 and 25 years old, at the Institute of Medical Sciences. Absolute latencies I, III, V and Inter-peak latencies I–III, I–V, III–V were measured separately for both ears. Statistical analysis was done by using the independent t-test and Mann-Whitney U test based on normality through SPSS version 20.0.
Results
Results revealed a statistically significant difference in absolute latency of Wave I and inter-peak latency (IPL) of I–III, I–V in the right ear and in the left ear. Wave III and IPL III–V were found to be significant. Females showed shorter absolute latencies and IPLs as compared to males.
Conclusion
Significant alterations in BAEPs provide evidence for the potential contribution of gender as an influencing factor in emerging adulthood.
Introduction
In recent years, brainstem auditory evoked potentials (BAEPs), brainstem auditory evoked response (BAER), and auditory brainstem response (ABR), as electrophysiological investigations, have become a useful tool for not only clinically evaluating hearing in children and reluctant patients, but also for noting the degree of hearing abnormalities in patients with dysfunctions in the brainstem. BAEPs have grown to play a significant role in the fields of audiology, neurology, neurosurgery, otolaryngology, and paediatrics, since their initial description in clinical medicine in the 1970s.1–3 BAEPs have a wide range of clinical applications, including the assessment of infants with suspected hearing loss and of individuals with possible retrocochlear lesions. BAEPs are known to have short latency potentials because they appear within the first 10 milliseconds after the presentation of acoustic stimulation. It is thought to represent highly synchronised activation of the cochlea and the midbrain’s primary auditory centres. According to several studies, sedatives and general anaesthetics have no effect on BAEPs. 4
The BAEP consists of seven waves, of which Waves I, III, and V are the most noticeable and have greater clinical significance. While presence of other waves is highly unpredictable and could not even be present in typical cases. The regions that generate these waves are different. Wave I and II originate respectively from the distal and proximal portions of the auditory nerve relative to the brainstem, Wave III goes through the cochlear nucleus, Wave IV originates from the superior olivary complex, Wave V is generated at the lateral lemniscus, Wave VI at inferior colliculus, and finally Wave VII is generated from the medial geniculate body. 5 The analysis of these waves can reveal the brainstem’s abnormal processes. Studies show that neurological development and brainstem functional integrity are generally associated with the BAEPs alterations. The latencies and amplitudes of the waveforms contain the clinically relevant information about BAEPs. Inter-peak latency (IPL) is one of the key BAEP components in diagnostic audiology, and in particular, IPL I–V is crucial because it reflects the central conduction time (CCT) or brain stem conduction time (BCT). CCT demonstrates how well the brain stem is functioning, and its deficiency suggests neurological disorders. 6
Many factors could have an impact on these wave latencies, IPL, and amplitude of BAEPs. These consist of stimulus-related factors such as stimulus intensity, rate, polarity, phase, etc; recording factors like electrode, filter, masking, and reference; subject-related factors or physiological variables as age, gender, body temperature, head size, hormonal status, hearing loss and anthropometric variables, etc. Subject characteristics, particularly ‘age’ and ‘gender’, have significant effects on BAEPs and have received considerable attention from researchers around the nation. Significant gender and age differences in both BAEP latencies and amplitude have been found in a large number of investigations of both normal and hearing-impaired patients. Researchers have found that those over 60 years exhibit greater latencies, although other studies have not identified any statistically significant variations in BAEPs latency with age.7–9
Several investigations have demonstrated that male subjects exhibit larger latency measurements (primarily in Wave V) and IPL (particularly in the I–V IPL) compared to female subjects. McClelland and McCrea did not discover a gender difference in latency until the age of 14, which suggests a connection to puberty’s bodily changes. It has been extensively examined how ageing affects the typical click-elicited ABR. It is well known fact that getting older causes a reduction in ABR amplitude; however, this is not always in a consistent pattern. Slight variations in latency and inter-peak intervals (IPIs) have also been seen.10, 11 Consequently, both age and sex are highlighted as factors that could affect BAEP recordings; nevertheless, the extent of their impact is still debatable, necessitating further research into these problems. The literature does not provide a clear explanation for the origin of these gender differences. The majority of researchers have hypothesised that lower latencies in females were caused by the brainstem’s smaller size, which led to reduced neural transmission times. Studies showing the gender difference to be caused by head size were absent until recently. Trune et al. examined the relative impact of head size, gender, and age on the ABR and showed that both men’s and women’s ABRs were sensitive to changes in head size. The women, however, continued to have shorter latencies when they were compared to men with smaller heads. 12
In the study on the effects of age, gender, and sensorineural hearing loss (SNHL) on ABR latencies, Jerger and Johnson discovered that younger women with SNHL had lower ABR Wave V latency than older women with a similar SNHL. There was no statistically significant difference between the ABR Wave V latency of younger and older males with comparable SNHL. Jerger and Johnson came to the conclusion that there must be other characteristics that distinguish younger women other than older women in order to explain the latency difference and suggest a possible hormonal influence. 13 Body temperature also has an impact on ABR amplitudes and latencies as well. Several studies have demonstrated that ABR Waves I–V latency can increase with a reduction in body temperature in humans. 14
A new notion of development termed ‘emerging adulthood’ is put forth, with a focus on the ages of 18–25, for the time period from late adolescence to early adulthood. Arnett suggested emerging adulthood as a stage of life with distinct demographic, social, subjective, physiological and psychological characteristics that occurs between adolescence and full-fledged adulthood. 15 It is generally known that age affects the BAEP waveform. The impact of gender on BAEP patterns, however, continues to be a topic of discussion. Although quite a few researches have looked into gender-based variations in BAEP waveform patterns among children, adolescence and elderly, there has not been a study done on the emerging adults specifically.
Methods
The present cross-sectional study was conducted at BERA LAB in the Physiology Department of the Institute. The study protocol was approved by the Research Ethical Committee of the Institute. All of the registered subjects were given a written consent form after being given information about the study in their own language. Without their consent, there would be no exposure of their identities.
Inclusion Criteria
After Institutional ethical committee approval, 120 subjects between the ages of 19 and 25 (50 male and 70 female) with normal audiometric hearing were chosen. They were chosen at random from among the relatives of patients (second-degree relatives) belonging to the region of Northern India who visited the hospital’s outpatient department and appeared to be in good health. Physical examinations were done. Body weight was measured by having the subject stand firmly on level ground against a strong wall, slide a flat object up to the head, and record their height using a measuring scale attached to the wall. A computerised gadget was used to weigh the subject. By dividing the weight in kilos by the square of the height in metres, one can determine their body mass index. The breathing rate was recorded. The radial arteries in both hands were used to determine pulse rate, and all data were recorded. With a sphygmomanometer, blood pressure was measured. To rule out any secondary causes of neurological deficiency, a comprehensive history and clinical examination were conducted.
Exclusion Criteria
Subjects were excluded if they had a history of head or ear trauma, significant occupational noise exposure, intake of known ototoxic drugs (such as aminoglycosides), or any other medication that might affect the normal functioning of the nervous system (such as antidepressants, antipsychotics, etc.). They were also excluded if they had a family history of deafness or any systemic illness that might affect the nervous system (such as uraemia, diabetes mellitus, stroke, hepatic encephalopathy, multiple sclerosis, thyroid disorders, anaemia, meningitis, etc.), a history of chewing tobacco, chronic alcoholism, or cigarette smoking, or who had undergone surgery, radiotherapy, or chemotherapy within the previous year were all excluded from the study.
BAEPs Recording
The BAEP procedure was carried out in a silent environment with a constant room temperature of 30°C. An appropriate BAEPs device called the NeuroStim-NS 2 (Medicaid Systems) was used to record the BAEPs under standard conditions. The apparatus is often referred to as a Brainstem Evoked Response Audiometer (BERA). It is a safe and non-invasive technique. Anthropometric measurements were performed after obtaining written consent and explaining the process to the subjects. In order to reduce muscular activity and prevent interference with the BAEP recording, readings were taken when the subject was lying down. To maintain their potential to obstruct the process, all metallic objects, jewellery, and other radiating objects were kept out of the subject’s contact. In order to identify any hearing impairments that might affect the recordings, analyses, and interpretation of the ABR, and other tasks, tuning fork tests (Rinne test, Weber test) were conducted prior to the recording sessions. The international 10/20 system of electrode placement with a single channel setting was used for electrode application. The forehead skin, as well as both mastoid processes, were then thoroughly cleaned to remove any oil. The active electrode, which was positioned onto the vertex (Cz) to maintain its location throughout the recording, was one of many electrodes spread out throughout the scalp. Moreover, the reference electrode was positioned in the area of the mastoid prominence, and the ground electrode was positioned over the forehead (Fz). Low filter was set at 100 Hertz, high filter at 10 kiloHertz, and the headphones were in the proper position. The wave patterns were recorded using brief click monoaural stimuli at 70 decibels with 2000 repetitions (11/second). All the manifested waves were recorded in the rarefaction setting as well as in a soundproof room. The waveform from each ear was measured up to twice to ensure reproducibility. We measured the IPL I–III, I–V, and III–V as well as the absolute latencies of Waves I through V.
Statistical Analysis
The data was evaluated using Statistical Package for Social Sciences System version 20.0 (SPSS 20.0). The Shapiro-Wilk test and the visual approach were used for normality testing. Data were presented using Mean ± SD and Median ± QD. Independent t-test and Mann-Whitney U test based on normality were used to compare the studied parameters. p < .05 was considered statistically significant.
Results
Age-matched healthy adult male and female subjects were selected in the current investigation to examine and compare the gender differences in BAEP latencies. 120 subjects were chosen from the relatives of patients who visited the hospital’s outpatient department and seemed to be in good health. SPSS 20.0 was used for analysing data. Before proceeding, BERA recording tuning fork tests (Rinne test and Weber test) were performed to identify any type of hearing loss. It helps in determining whether subjects may have any conductive or SNHL. Both tests were positive and central, respectively. 240 ears were evaluated using a rarefaction click stimulus at a rate of 11 clicks per second. The sound pressure level (SPL) was 70 decibels, which was above the subjective hearing threshold. Ipsilateral stimulation was used for recording BAEPs. The absolute and IPL of all waves were calculated and analysed. According to normality of data independent t-test and a Mann-Whitney U test were done to compare BAEPs latencies between the two sexes.
Comparison of BERA Wave Latencies (in Milliseconds) in Right and Left Ear of Both Genders.
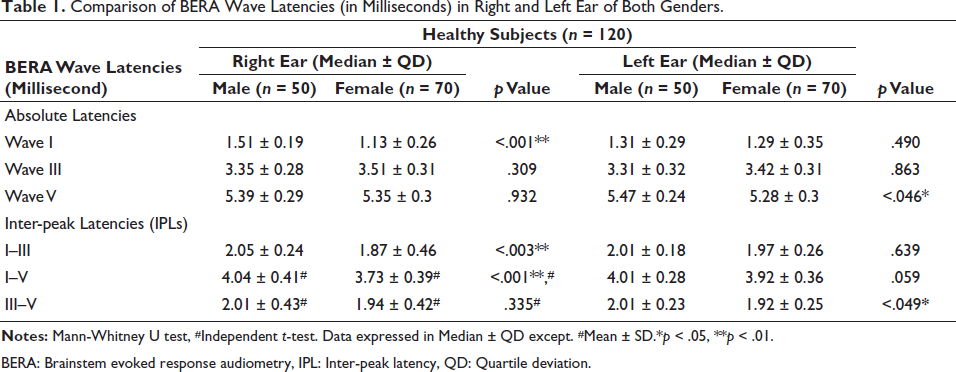
BERA: Brainstem evoked response audiometry, IPL: Inter-peak latency, QD: Quartile deviation.
Figure 1 represents a statistically significant difference in right ear BERA wave latencies in both genders. Female shows shorter latencies as compared to males in Wave I, IPL I–III and I–V in the right ear.
Shows Differences in Right Ear Wave Latencies in Both Genders.
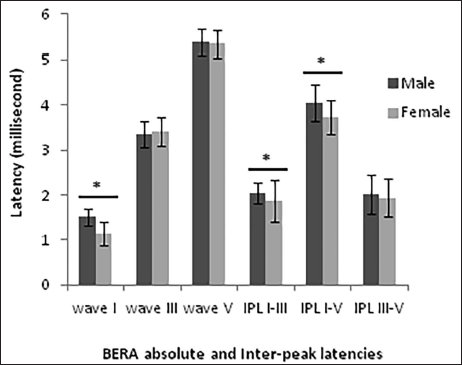
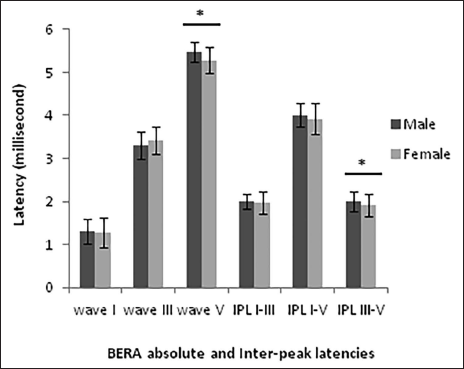
Figure 2 shows that females have significantly shorter Wave V and IPL III–V latency in the left ear. Whereas some wave shows a slight difference in latencies of BAEPs when compared with males, although it is not statistically significant.
Shows Differences in Left Ear Wave Latencies in Both Genders.
Discussion
The present study explored to determine how gender affected the BAEP latencies in emerging adult individuals of either sex. In response to an auditory input, the brain produces very small electrical voltage potentials called BAEPs, which are recorded from the scalp. As a result, BAEPs involve activity along the entire auditory pathway, from the cochlear hair cells to the cerebral cortex. BAEPs can be categorised based on latency, which is the amount of time between the presentation of a sound stimulus and the peak of the wave. As electrical activity in the auditory nerve and brainstem responds to an acoustic input, the auditory nerve and the brainstem produce far-field reflections known as BAERs or BAEPs, which can be recovered from the electroencephalogram by filtering and averaging.
Results of the present study revealed that females had shorter absolute latencies and IPLs compared to the males as in agreement with previous studies.16, 17 However, these differences were found statistically significant for Wave I and IPL I–III, I–V in the right ear and in the left ear, the differences were found in Wave V and IPL III–V. This difference directly suggests that BAEPs are affected by gender in emerging adulthood. According to Tandon and Mishra’s research, gender differences in BAEP latencies begin around the age of 16. 18 Jerger et al. (1980) reported that ABR was impacted by gender. At all age groups, female individuals consistently displayed shorter latencies and higher amplitudes in both normal and hearing-impaired subjects. Wave V amplitude was around 25% greater, and Wave V delay was roughly 0.2 ms shorter in female subjects. 13
There is mounting evidence that gender is one of the key factors which affect BAEPs. The findings from this study showed a significant difference between the sexes in the Wave V latency time and the III–V IPI; males had longer latencies in left ear and also in Wave I and IPL I–III, I–V in right ear. This finding is consistent with other published findings indicating an increase in Wave V and the I–V IPI in males.8, 19
The latency of Waves I values in our study is significantly higher in males than in females in the right ear, which is consistent with studies done by Dass et al., Trune et al. and Manjuran & Arora.12, 20, 21 In the present study, females exhibited significantly shorter Waves V latency than males, which corroborated with findings of other studies.22, 23, 12 Research conducted outside of India has revealed significant differences in absolute Wave I, III, V, and IPL I–III, I–V, and III–V latencies regarding genders, which are frequently reported by researchers and complement the findings of our study.9, 24, 25
Stockard et al. (1978) hypothesised that the anatomical distance of the auditory pathway in females may be shorter than that in males because the generators of the ABR components are considerably adjacent to one another. The mean IPL value for I–III, I–V in the right ear was prolonged in males than in females; on the other hand, on the left side, it was found statistically significant in IPL III–V. Moreover, Stokard et al. also noted that the IPLs of men were longer than those of women. 26 Furthermore, in diabetics, particularly in those with peripheral neuropathy, Goldsher et al. reported bilateral symmetrical prolongation of all peak latencies as well as prolongation of I–III, I–V, and III–V IPL differences. 27 Sharma et al. also observed that diabetics had longer Wave I, III, and V latencies as well as longer I–III and I–V IPL. 28
Conduction from the VIII nerve across the subarachnoid space is measured by IPL I–III. The IPL values do not increase with age, according to Oku and Hasegewa, and Costa et al., in particular, I–III IPL decreases.11, 29 Fallah TM and Maria Khatoon et al., reported that I–III IPL is shown to be prolonged as age increases from younger to older.7, 30
III–V IPL measures conductivity from the lower pons to the midbrain. The present study found a statistically significant difference in III–V IPL regarding gender, whereas in other studies, no changes were found. The III–V IPL was discovered to be prolonged as people aged from younger to older by Uziel A et al. 31
One indicator of conduction from the proximal VIII nerve via the pons to the midbrain is the I–V IPL. A statistically significant change was observed in left ear I–V IPL. Roshenhall U et al. noted no significant change in their study. The majority of researchers have hypothesised that lower latencies in females were caused by the brainstem’s smaller size, which led to reduced neural transmission times. Studies showing the gender difference to be caused by head size were absent until recently. The women, however, continued to have shorter latencies when they were compared to men with smaller heads.9, 12 Numerous studies have reported that the reason why females’ BAEP latencies are lower than those of males might be related to their faster neural conduction (shorter conduction time), relatively explained by their smaller heads and greater body core temperatures. 32
Studies have shown that acetylcholine (Ach) may be one of the neurotransmitters involved in the auditory pathway, and that oestrogen and Ach may interact to enhance the transfer of auditory information. Also, it has been suggested that female sex hormones, particularly oestrogen, have a positive impact on the neuronal plasticity and metabolic levels of neurotransmitters, leading to a reduction in the time it takes for neurons to conduct electrical impulses in the auditory pathway. 33 In addition, studies also emphasise on effect of functional changes of hormones on BAEPs. Synaptic transmission was impacted by ovarian steroids, oestrogen, and progesterone at the level of the brainstem. Gamma-aminobutyric acid (GABA) secretion has likely been modulated in a counter-regulatory manner, which is the most likely explanation. Oestrogen may strengthen the inhibitory effects of GABA by promoting its secretion, hence the process is delayed. Progesterone, on the other hand, may lessen neurons’ sensitivity and attenuate the oestrogen-potentiated GABA release. The auditory conduction mechanism is thought to be slowed down by the elevated levels of oestrogen that are present during pregnancy. 34 In women who have a male twin and during menopause, the gender gap in hearing is lessened. The hormonal hypothesis is also supported by the fact that females with Turner syndrome, a chromosomal defect that causes an oestrogen deficiency, have longer BAEP latencies and earlier presbycusis, similarly to males. Females’ menstrual cycles are correlated with changes in their auditory sensitivity. ABR and electroencephalography (EEG) show changes during the menstrual cycle. 35 Allison et al. (1983) explained these variations in BAEPs latency ascribed to the difference in body size between males and females. ABR wave amplitude and latency differences might result from differences in head size, which affects the length of the auditory neural circuit. 19
The cochlear duct is longer in men than in women, which contributes to longer cochlear travelling durations in men. Moreover, greater basilar membrane stiffness and shorter cochlear ducts in females may lead to earlier ABR latencies than in males. The travelling wave’s velocity increases, causing small increases in neuronal synchronisation. In addition, the olivo-cochlear bundle (OCB), a component of the efferent auditory system, functions differently in males and females. Studies demonstrate that males have a more active auditory efferent system, which may have an impact on peripheral mechanisms. Moreover, behavioural and imaging investigations have demonstrated that the auditory cortex processes acoustic inputs differently in males and females revealed through fMRI studies have revealed that the language regions of the cortex are more active in females. 36 The fact that the results of the earlier research involved older people, whereas the subjects in our study were younger, can help to explain some of the differences between the outcomes of the two investigations.
The clinically important implication of the study suggests employing gender specific normative data when using BAEPs for therapeutic applications. The value of this normative data can also be utilised for comparing data of people with compromised auditory functions. To obtain the typical range of BAEPs in a healthy, normal person, well-organised, large-scale investigations are unquestionably required. Also, there is an urgent need to conduct more such research on a regional basis, given the dearth of studies of this age range. Also, this would assist in uniformising the BAEP waveform pattern across groups of people who are developing into emerging adults.
Conclusion
The present study revealed that, subject’s variable, that is, gender, has a statistically significant influence on BAEPs latency in emerging adults belonging to Northern India. Gender might influence how ABRs are interpreted, and clinicians should take these factors into account in clinical settings. Consequently, different norms for various age groups and genders should be developed in clinical practise.
Footnotes
Abbreviations
BAEPs: Brainstem auditory evoked potentials
ABRs: Auditory brainstem responses
BAERs: Brainstem auditory evoked responses
BERA: Brainstem evoked response audiometry
IPL: Inter-peak latency
SNHL: Sensorineural hearing loss
SPL: Sound pressure level
OCB: Olivo-cochlear bundle
GABA: Gamma-aminobutyric acid
EEG: Electroencephalography
CCT: Central conduction time
BCT: Brainstem conduction time
QD: Quartile deviation
Acknowledgements
The authors are thankful to all the enrolled subjects, without whose active participation, this work would not have been possible. We are also grateful to the Physiology Department and the institute for all their help and support.
Authors’ Contribution
AG made substantial contributions to the conception of the study as well as the whole design of the research work, SKS have substantively reviewed the study, HBS contributed to the analysis and the interpretation of data, JSY supported in the acquisition of the data, and AC helped in editing the manuscript. All authors contributed to the article and approved the submitted version.
Consent For Publication
All of the registered subjects were given a written consent form after being given information about the study in their own language. Without their consent, there would be no exposure of their identities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Statement of Ethics
The study protocol was approved by the Research Ethical Committee of the Institute. Name of ethics committee: Institute Ethical Committee. Reference no.: Dean/2019/EC/1755.