
Abstract
Background
Ulcerative colitis (UC) is a chronic condition characterised by inflammation of the large intestine, causing an impact on a patient’s psychological well-being. Earlier research has demonstrated the important role of locus of control (LOC) in facing the challenges brought out by many gastrointestinal system diseases.
Purpose
The aim of this research is to assess LOC in patients with mild-to-moderate UC as compared to non-UC individuals. This study also explored the impact of various demographic variables: age, gender, education level, type of family, working status, socio-economic status (SES), marital status and region of residence, on LOC among UC patients
Methods
A cross-sectional survey was conducted for a period of two months. The tool used was Multidimensional Health Locus of Control (MHLC). A chi-squared test was used to investigate the LOC among individuals with UC (100 patients) in comparison to a control group of non-UC (100) healthy individuals. The age group was between 30 and 50 years.
Results
In the UC group, 31% endorsed an internal LOC, while 40% attributed outcomes to chance, and 29% believed in powerful others. A chi-square test indicated a significant association between LOC and UC, χ²(2) = 38.1, P < .001. These findings suggest that individuals with UC are more likely to attribute outcomes to external factors, such as chance or powerful others, rather than their own actions. A positive effect of SES, region and working status on LOC was seen.
Conclusion
The observed tendency towards external LOC highlights the need for targeted interventions aimed at enhancing patients’ sense of agency and control over their health. Healthcare professionals can help people with these chronic conditions live better lives and achieve better results by enabling them to actively participate in their health.
Introduction
Ulcerative colitis (UC) and Inflammatory Bowel Disease (IBD) are chronic conditions characterised by inflammation of the digestive tract, leading to a range of distressing symptoms. 1 Beyond the physical challenges, these conditions can significantly impact an individual’s mental and emotional well-being. One psychological concept that holds relevance in understanding how patients cope with UC/IBD is the locus of control (LOC). LOC refers to an individual’s belief about the extent to which they can control events in their lives. 2 Individuals who have an internal LOC believe that they have control over their life events. On the other hand, those with an external LOC attribute their experiences to external forces or luck.
LOC can play a critical role in UC/IBD patients as they need to adapt to the challenges posed by their condition. Those with an internal LOC have a belief that they have power over circumstances which means believing they can do something about it too. 3 Such people will are proactive in taking care of their health and managing their illnesses, are more likely to stick to treatments when things take a turn for the worst. They are also better equipped to handle the stress of chronic illness. This includes seeking information and making lifestyle changes in order to improve their condition. 4 On the other hand, patients with no control over their health will feel powerless as they blame external forces for their situation. This perspective is dangerous because it can lead to feelings of depression and anxiety which may make it hard for them to focus on self-care. 5 Doctors should acknowledge and address this mindset as it can have a massive impact on how successful treatment is for people with UC/IBD.
Many studies have given insight into the psychological aspects of UC. In distressed patients with UC, Boye et al.’s (2008) INSPIRE study investigates the relationship between personality traits and disease-specific quality of life. 6 According to the research, there is a correlation between various personality traits and different dimensions of quality of life. This demonstrates the complex psychological effects of IBD on people and emphasises the significance of taking personality factors into account when providing patients with holistic care. Another study conducted by de Dios-Duarte et al. (2022) delves into the relationship between flare-ups in Crohn’s disease, a subtype of IBD, and psychological factors, particularly stress and external LOC. 7 The findings suggest a significant association between external LOC and the occurrence of flare-ups. Mussell et al. (2004) investigated the predictors of disease-related concerns and similar other aspects of health-related quality of life in outpatients with IBD. 8 The study highlights the significant influence of psychological factors on the well-being of UC patients. It emphasises the significance of understanding the LOC in managing UC, suggesting that an internal LOC may contribute to improved quality of life. Similarly, Náfrádi et al. (2017) present a systematic review exploring the relationship between self-efficacy, health LOC, and medication adherence. 9 This study highlights the crucial role of patient empowerment and self-belief in adherence to medication regimens. Understanding the influence of LOC on medication adherence in UC patients provides a critical perspective for healthcare providers seeking to optimise treatment outcomes. A study by López-Larrosa (2013) delves into the connection between quality of life, treatment adherence, and LOC, particularly in the context of chronic medical illnesses. 10 The study emphasises the role of family dynamics in shaping an individual’s sense of control over their health. This research shows the importance of considering the broader support system when addressing LOC in UC patients. These studies emphasise the pivotal role of psychological factors and LOC in the context of IBD, providing valuable insights for healthcare professionals aiming to optimise patient care and treatment adherence.
Recent research has delved into the intricate relationship between coping mechanisms and the LOC in individuals grappling with IBD. Yeates (2017) studied coping mechanisms in young individuals with IBD, highlighting the impact of LOC on adaptive coping. 11 Those with an internal locus engaged in effective problem-solving and adaptive techniques, suggesting potential intervention strategies for young IBD patients. Pellissier et al. (2010) delve into the psychological adjustment and autonomic disturbances in individuals with IBDs and irritable bowel syndrome. 12 The study suggests that an internal LOC may positively influence the psychological adjustment to UC, potentially leading to better outcomes. Hence, the research discussed demonstrates the significant impact of LOC and perceived control over health outcomes on coping strategies for individuals with IBD, offering valuable insights for the development of targeted interventions and improved patient outcomes.
The above researches highlight how LOC is an important psychological factor that influences how individuals with UC/IBD perceive and manage their condition. Research has consistently shown that individuals with an internal LOC tend to exhibit better coping strategies, adherence to treatment regimens, and utilisation of support systems. Therefore, incorporating interventions aimed at enhancing LOC can be a valuable component of holistic care for patients with UC/IBD. By empowering individuals to take an active role in their health, healthcare providers can contribute to improved outcomes and a better overall quality of life for those living with these chronic conditions. The current study aims to understand the level of LOC in patients with UC, as compared to non-UC individuals. We hypothesise that fewer individuals with UC will have an internal LOC than the non-UC population and more will have external LOC.
Methods
Sample
The study encompassed a cohort of 200 Indian participants, comprising 100 individuals in normal health (non-UC, non-diabetic, without any cardiac, renal or psychiatric issues) and an equivalent number diagnosed with UC. Each group exhibited an equal distribution of 50% males and 50% females. Participants were carefully selected within the age bracket of 30–50 years. Any age group can be affected by UC. The age of onset peaks between the ages of 15 and 30 and between the ages of 50 and 70. 13 Hence this age group was chosen where patients have mild-to-moderate symptoms. Mild-to-moderate UC is defined as patients with less than four to six bowel movements per day, mild-to-moderate rectal bleeding, no constitutional symptoms, a low total inflammatory burden, and no signs of high inflammatory activity. 14 These patients were selected from three hospitals in the Nagpur region on the basis of colonoscopy and other symptoms after talking to the gastroenterologist. The sample was diverse in terms of socio-economic status (SES) encompassing individuals from various economic strata. 15 Additionally, the study accounted for both urban and rural residences, thereby providing a comprehensive representation across different living conditions.
Test Details
The Multidimensional Health Locus of Control (MHLC) scales are pivotal tools in health psychology research, offering insights into individuals’ perceptions of control over their health outcomes. The widely utilised Forms A and B, initially introduced by Wallston, Wallston, and DeVellis in 1978, consist of three 6-item subscales: internality, powerful others externality, and chance externality. 16 Over the past three decades, Forms A/B have been instrumental in over a thousand studies and extensively cited in the literature. Form C, designed for condition-specific assessments, allows for tailored evaluation in populations with existing medical conditions, such as UC. There are six items on Form C, and scores range from 6 to 36, with higher scores denoting stronger internal control beliefs. 17 Examples of such statements are: ‘The main thing which affects my condition is what I myself do’ and ‘If my condition worsens, it is my own behaviour which determines how soon I will feel better again’. Test-retest reliability, construct validity, and internal consistency reliability are all sufficiently demonstrated by the MHLC. 17 With test-retest stability coefficients ranging from 0.60 to 0.70 across studies and Cronbach alphas ranging from 0.60 to 0.75, the scales are generally considered to be moderately reliable. 18
Procedure
The research procedure involved administering a pencil–paper test to a sample of 200 individuals. Participants were briefed on the study concerning LOC in Persons with UC and those without the condition. They were informed that the questionnaire aimed to gather specific information related to their perceived control over influencing factors in their lives. Participation was voluntary, and prior to commencement, participants were required to sign an informed consent form granting their approval for involvement. Clear instructions were provided regarding the questionnaire they were about to answer. The completion time for the entire set of questions was estimated to be a maximum of 10–15 minutes. Participants were assured that all information and responses collected would be kept strictly confidential. They were also explicitly informed of their absolute right to decline participation or withdraw from the study at any point without the necessity of providing a reason. Inclusion criteria included persons receiving the diagnosis of UC based on colonoscopic investigation, and histological criteria. Patients with mild-to-moderate disease activity were considered for this study. Exclusion criteria included those with any major medical issues (diabetics, cardiac issues, kidney failure, neurological diseases, cancer etc and any psychiatric disorders on medications). In all 236 participants were given the data collection tool. The forms received back were 208. Out of the total participants, 28 students did not provide responses, resulting in a response rate of 88%. However, some of the received forms were incomplete and so were excluded from the study. As a result, the research included the responses of 200 participants who provided complete and usable data for the study.
Analysis
The analysis of this study involved the application of a chi-squared test, a robust statistical tool suitable for non-parametric and categorical data, to investigate the LOC among individuals afflicted with UC in comparison to a control group of non-UC healthy individuals. This study also explored the impact of various demographic variables: age, gender, education level, type of family, working status, SES, marital status and region of residence, on the experience of UC patients. Thus, the research aimed to gain deeper insights into the potential correlations and associations that may exist between these demographics and the manifestation and management of UC.
Results
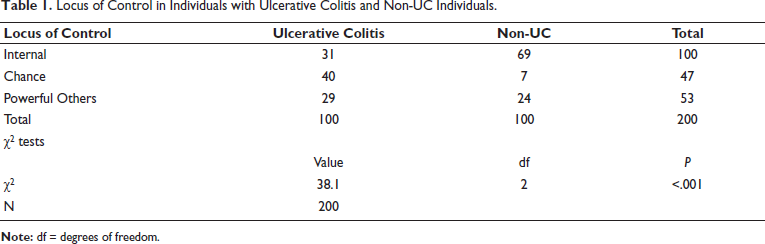
The study aimed to explore the relationship between LOC and UC in a sample of 200 individuals, with 100 UC patients and 100 non-UC participants. In the control group, 69% reported an internal LOC, 7% attributed outcomes to chance, and 24% believed in powerful others’ influence. Conversely, in the UC group, only 31% endorsed an internal LOC, while 40% attributed outcomes to chance, and 29% believed in powerful others’ influence. A chi-square test indicated a significant association between LOC and UC, χ²(2) = 38.1, P < .001, with 2 degrees of freedom (Table 1). These findings suggest that individuals with UC are more likely to attribute outcomes to external factors, such as chance or powerful others, rather than their own actions. This insight into LOC may have implications for understanding coping mechanisms and psychological adjustment in individuals with chronic conditions like UC.
Locus of Control in Individuals with Ulcerative Colitis and Non-UC Individuals.
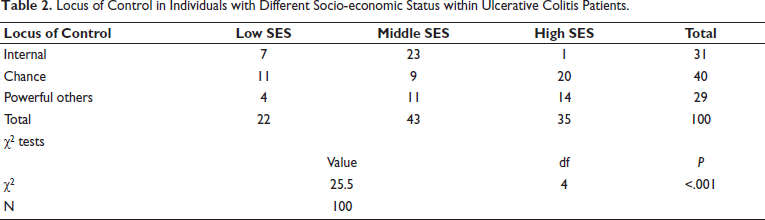
Additionally, within the UC patient group, further analysis was conducted on demographic variables, revealing a positive effect of SES, region and working status on LOC. Specifically, in the high SES group, 1 individual had an internal LOC, 20 individuals attributed outcomes to chance, and 14 believed in powerful others’ influence. In contrast, in the middle SES group, 23 individuals had an internal LOC, 9 attributed outcomes to chance, and 11 believed in powerful others’ influence. Finally, in the low SES group, only seven individuals endorsed an internal LOC, 11 attributed outcomes to chance, and four believed in powerful others’ influence. The chi-square test indicated a significant association between SES and LOC within the UC patient group, χ²(4) = 25.5, P < .001 (see Table 2).
Locus of Control in Individuals with Different Socio-economic Status within Ulcerative Colitis Patients.
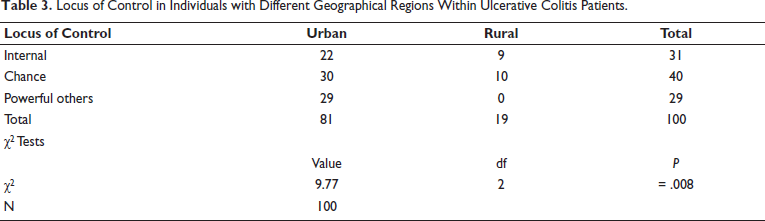
Similarly, in the urban region, 22 individuals had an internal LOC, 30 attributed outcomes to chance, and 29 believed in powerful others’ influence. In contrast, in the rural region, 9 individuals endorsed an internal LOC, 10 attributed outcomes to chance, and none believed in powerful others’ influence. The chi-square test indicated a significant association between region and LOC within the UC patient group, χ²(2) = 9.77, P = .008 (Table 3).
Locus of Control in Individuals with Different Geographical Regions Within Ulcerative Colitis Patients.
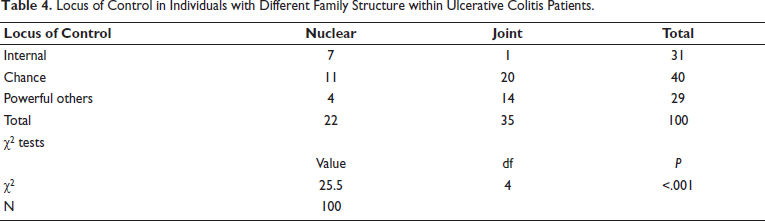
Furthermore, when considering family structure, within nuclear families, four individuals had an internal LOC, 20 attributed outcomes to chance, and 23 believed in powerful others’ influence. In contrast, in joint families, only 27 individuals endorsed an internal LOC, 20 attributed outcomes to chance, and six believed in powerful others’ influence. The chi-square tests indicated significant associations between family structure and LOC within the UC patient group, χ²(2) = 26.8, P < .001 (See Table 4).
Locus of Control in Individuals with Different Family Structure within Ulcerative Colitis Patients.
Discussion
The aim of this study was to investigate the LOC in patients with UC compared to a control group. The MHLC scale was employed to assess the individuals’ perceptions of control over their health-related outcomes. The primary hypothesis was that patients with UC would exhibit a higher tendency towards external LOC as compared to the non-UC control group. The chi-squared test demonstrated a significant association between UC patients and higher external LOC. These findings are in line with previous research that suggests chronic illness may be correlated with an increased belief in external factors influencing one’s health outcomes.
Not many researchers were found in adults in this particular age group, but several researches on IBD consistently found that children and adolescents with IBD exhibited an external LOC.19–21 They attributed their illness and health issues to external factors rather than their own actions or behaviours. A study by Mussell et al. (2004) emphasised this concern for those outside factors too, specifically in outpatients with IBD. 8 Their research showed that people with IBD oftentimes have more concerns about their condition than necessary, creating a sort of heightened fear around it. Our results also showed a similar trend among our UC patients. The increased prevalence of LOC could reflect an externalised nature, potentially stemming from the fact that they have been living through a chronic illness for so long. Another study especially focusing on health LOC, looked at individuals with IBD and healthy individuals to study their coping strategies. 22 The results they found were that people with IBD were more likely to use coping strategies centred around external control. 22 A big emphasis was on the factors outside of them that could influence their health. Similarly, a study by Engstrom in 1999 aimed to see the correlation between family interaction and LOC in children and teenagers diagnosed with IBD. 23 The findings showed that a significant number of these young individuals only exhibited an external LOC towards life’s situations. This suggests that the way they perceive their sickness is influenced by external factors such as family dynamics and medical interventions. Woods et al. (2020) looked at somatisation and childhood disease exacerbation. This showed that children with IBD had a greater propensity to somatise their symptoms, which was indicative of an external LOC tendency. This suggests that the children often attribute their physical symptoms to stressors or other external factors. In a similar study, Yeates (2017) looked at coping strategies in young people with IBD and found that a sizeable percentage of them relied on outside sources of control to manage their condition. 11 This dependence on outside sources draws attention to the general theme of external LOC in the community of individuals with IBD. These studies collectively show the consistent pattern of an external LOC in individuals with UC and IBD.
In clinical practice, identifying and addressing this external LOC can help develop more individualised and successful interventions for these people. This increased external LOC can be due to the erratic and uncontrollable nature of the illness. Due to this UC patients believe that events in their life are primarily controlled by external factors rather than one’s own actions or decisions.8, 12 The complex interplay between the psychological and physiological components of UC was highlighted by Pellissier et al. (2010). 12 Having a chronic illness like UC can have a negative emotional impact and make it more difficult for a person to see how other people are influencing their experiences. One way that this emotional impact manifests itself could be through an increased external LOC. In addition to individual factors, family dynamics can also significantly influence how UC patients perceive their LOC. Wong and White (2002) investigated the association between the health LOC and adults with ostomies. 24 The significance of familial relationships for individuals with chronic illnesses is underscored by this study, even though the focus was not on only UC patients. An external LOC may be exacerbated in UC patients by their perception of their family’s involvement in their care as an outside force impacting their well-being. De Dios-Duarte et al. (2022) investigated the impact of stress and external LOC on IBD flare-ups associated with Crohn’s disease. This study highlights the part that psychological variables play an important role in symptom exacerbation. 7 Because UC is a chronic condition, patients may further reinforce their external LOC by attributing variations in their condition to outside forces. In addition, patients might find it difficult to manage their UC, which includes following their medication schedule and making lifestyle changes. Patients may feel powerless to influence their health outcomes due to the complexity of managing a chronic condition. 9 A heightened external LOC may result from patients coming to believe that external factors are the primary determinants of their health. For clinical practice, it is important to consider the consequences of UC patients having a primarily external LOC. Healthcare professionals should be aware of these patterns and put plans in place to enable patients to manage their conditions on their own. A patient’s sense of agency over their health, education about the disease process, and active participation in treatment decisions can all help lessen the negative effects of an external LOC on UC patients’ general well-being.25–27
Limitations and Future Implications
It is important to recognise the limitations of this study even though it offers insightful information about the LOC of UC patients. First of all, the small sample size may have affected how broadly the results could be applied. The use of self-reported measures also runs the risk of introducing response bias. Furthermore, cross-cultural validation was warranted because the study primarily concentrated on a single cultural context. Regarding potential future implications, increasing the sample size and adding objective measurements may improve the results’ robustness. Considering broader sociocultural factors and examining longitudinal trends may provide a more thorough understanding of LOC UC. Lastly, researching specialised interventions to improve UC patients’ emotional well-being may have a major positive effect on their quality of life.
Conclusion
To conclude, this research offers a significant understanding of the LOC in individuals suffering from UC. The tendency toward external LOC that has been observed emphasises the necessity of focused interventions meant to strengthen patients’ sense of agency and control over their health. Healthcare professionals can help create a more thorough and efficient strategy for managing UC and enhancing the general well-being of those who are impacted by it by addressing these psychological aspects. A number of factors, including family dynamics, psychological adjustments, disease-related worries, and the stress of managing a chronic illness, contribute to the high level of external LOC seen in UC patients.
Footnotes
Abbreviations
UC – Ulcerative Colitis
LOC – Locus of control
MHLC – Multidimensional Health Locus of Control
IBD – Inflammatory Bowel Disease
SES – Socio-economic status
Acknowledgements
The authors would like to thank the patients of ulcerative colitis who participated in this research. We would also like to thank the hospitals for giving permission for conducting this research.
Authors Contribution
Dr Shaini Suraj, Ms Nayna Rane and Dr Anand Prakash have conceptualized and designed the study, led data collection, and have analysed the data. The original manuscript draft was prepared by Dr Shaini Suraj, Dr Pradeep Patil and Dr Deepa Sangolkar. Dr Pradeep Patil and Dr Anand Prakash provided guidance on study design and data analysis. All authors contributed to the revision of the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Ethical Committee has confirmed that no ethical approval is required due to the nature of the study. Permission was taken from concerned authorities of the hospitals where study was conducted. Full confidentiality was maintained by assigning a code to each participating patient’s document. Data was stored with security code.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Participants were informed of the confidentiality of their responses and all doubts were clarified before they filled the on-line questionnaire.