
Abstract
Background
Family interaction plays a pivotal role in the overall well-being of each member of a family unit. It is foreseeable that a family caring for an individual with a mental or physical health condition could experience negative family interactions for various reasons. Expressed emotion refers to the family environment based on the relatives’ interaction with the individual diagnosed with a specific illness. Expressed emotion in the families of a person with any form of mental condition could pose potential psychological distress and burden to family members, notably the primary caregivers.
Purpose
The current study intends to explore the expressed emotion of the primary caregivers toward children with neurodevelopmental disorders (NDDs). The association between expressed emotion, stress experienced by the caregiver, and the self-sufficiency of the child diagnosed with neurodevelopmental disorders was examined.
Methods
The Five-Minute Speech Sample (FMSS), Kingston Caregivers’ Stress Scale (KCSS), and Waisman Activities of Daily Living (WADL) were used to assess expressed emotion, stress, and a child’s self-sufficiency, respectively. The snowball sampling technique was adopted, and data were collected from 35 primary caregivers through telephonic interviews. A mixed-method research design was adopted, and the data were analyzed qualitatively and quantitatively.
Results
The findings reveal that there is a significant association between expressed emotion and caregivers’ stress, expressed emotion, and the child’s self-sufficiency and a significant relationship between the caregivers’ stress and the child’s self-sufficiency. The qualitative analysis suggests the influence of factors such as future concerns, family factors, and relationship strains contribute to expressed emotion.
Conclusion
It can be concluded that those primary caregivers who reported extreme caregivers’ stress and low self-sufficiency in their child exhibited high negative expressed emotion and diverse individual and systemic factors influenced the display of high expressed emotion within the family.
Introduction
Positive interaction within a family unit ideally fosters healthy behaviors, enhances self-esteem, improves one’s ability to cope effectively, and promotes individual well-being across the lifespan. 1 As humans, we are all social beings; we thrive for social connection and belongingness that profoundly impacts our well-being. 2 Exposure to stressful events could influence an individual’s well-being. One such probable stressful event is the strained relationship between family members. 3 Those receiving protective resources, like social support from loved ones in the family, experienced a greater feeling of self-esteem, self-worth, emotional reserve, optimism, sense of meaning, financial stability, and improved mental and physical well-being.4–8
An antithetical situation where a person is deprived of social support or exposed to a strained relationship such as arguments, being critical, or a clash of opinions leads to increased stress. Deprivation of social support results in health-compromising coping behavior and immune alterations ensuing physiological and psychological concerns. 9 Every family unit experiences a strained relationship at some point in life. However, the complexity of strained relationships within the family caring for a child with neurodevelopmental disorders (NDDs) must be emphasized especially for parents with primary caregiving roles as it is often challenging and involves long-term day-to-day caregiving. 10
Neurodevelopmental disorders (NDDs) are behavioral and cognitive conditions that appear throughout the developmental phase and are characterized by significant difficulties in the development and performance of a particular set of intellectual, motor, and social functions. 11 Although NDD is characterized as a childhood disorder, it is largely been recognized as a lifelong condition. 12 Thus, caring for children with NDD is a lifelong process. Primary caregivers of children with NDD experience physical and psychological distress during caregiving. 13 The family caretakers experience a great deal of stress and burden as a result of the increased caregiving tasks, roles, and responsibilities, and this could potentially result in high expressed emotion. 14
“Expressed emotion is a measure of the affective relationship between two people and is characterized by criticism, hostility, and an emotionally over-involved attitude.” 14 Expressed emotions among family members of a person with schizophrenia and other psychiatric disorders are well-researched and documented in the Indian context.15–18 However, research in the area of expressed emotion among primary caregivers of children with NDDs is limited. Research suggests that expressed emotion can predict clinical outcomes and relapse rates in a person diagnosed with a particular mental disorder.19, 20
Expressed emotion impacts family members by raising their stress levels, often increasing depression and anxiety among family members. 21 The caregivers’ stress and expressed emotion could also be largely determined by the child’s level of self-sufficiency. “Self-sufficiency is an acceptable level of functioning either by the person themselves or through the adequate organization help from informal or formal care providers.” 22 Caregivers’ psychological well-being and level of expressed emotion could also influence the future behavioral problems exhibited by children with NDD. Likewise, expressed emotion in the families of a person with any form of mental condition could also pose potential psychological distress and burden to family members, notably the caregivers. 23
Therefore, it is imperative to address the family interaction, relationship quality, and caregivers’ emotional experience during caregiving and provide resources in the form of counseling, psychosocial support networks, training, and strategies. It is essential to introduce family-based intervention to improve caregiver–child interaction, treatment outcomes and reduce the stress and burden of caregiving, and improve the family well-being. Thus, the current study intends to explore the expressed emotion exhibited by the primary caregivers of children with NDD and associate it with their level of stress and self-sufficiency in the activities of daily living in their children.
Objectives
To determine the association between expressed emotion and caregivers’ stress.
To determine the association between expressed emotion and caregiver-reported self-sufficiency in children with NDD.
To determine the relationship between caregivers’ stress and caregiver-reported self-sufficiency.
To understand the factors influencing expressed emotion within the family through the caregivers’ speech samples.
Hypotheses
Method
A mixed-method research design was used. The data were collected from the participants through a telephonic interview and analyzed both quantitatively and qualitatively. The non-probability sampling design was adopted, and the snowball sampling technique was used to recruit participants for the study. Thirty-five primary caregivers of children with NDD who fulfilled the criteria volunteered to participate in the study. The primary caregivers were recruited in two ways: (1) The known people who are parents and/or primary caregivers of children with NDD were approached through phone calls by the researchers. (2) Call for participants for a one-on-one telephonic interview was advertised through various social media platforms. The recruitment of participants was stopped once data saturation was achieved.
Inclusion criteria
Primary caregivers between the age group of 25–60 years.
Caregiver (mother, father, or grandparents) involved in the child’s primary care.
Primary caregivers of children between 10 and 18 years diagnosed with NDD (ASD, cerebral palsy, learning disability, and intellectual disability) and its comorbidities.
Primary caregiver who has lived with the child for more than six months and takes care of their essential needs.
Exclusion criteria
Primary caregivers of children or persons with other physical or mental health conditions apart from the NDDs chosen for the current study (ASD, cerebral palsy, learning disability, and intellectual disability) and their associated comorbidities.
Caregivers having other significant persons with psychiatric or medical illness for whom they are providing care.
Procedure
The primary objective of the research study was briefed, and the recruited participants were asked to participate in the current study through a telephone interview. The Five-Minute Speech Sample (FMSS), Kingston’s Caregiver Stress Scale (KCSS), and Waisman’s Activities of Daily Living (WADL) were administered by telephone. The one-on-one telephonic interview of the FMSS was recorded, transcribed, and analyzed to interpret the data.
The following instructions were provided to the primary caregiver to obtain the FMSS. “I would like to hear your thoughts about your kid _________ in your own words. I want you to speak for the next five minutes without my interruption, describing the kind of person your child is, how you two get along, and the kind of connection you have with them. I want to reassure you that your answers will be anonymous, confidential, and used only for research. Do you have any queries you’d like to ask me before we start?” Once the FMSS was obtained, then the participant was instructed on responding to the KCSS and WADL, respectively.
Measures
Sociodemographic Details
The demographic details of each participant such as age, gender, profession, socioeconomic status, relationship with the child, diagnosed condition (type of NDD), duration of the condition, duration of caregiving, and other relevant details were obtained at the beginning of the telephonic interview.
FMSS
The FMSS was developed by Magaña et al. 24 for assessing expressed emotion towards a family member with mental illness. It has an internal consistency of (> (or) = 0.8) and a test–retest reliability of (r = 0.64). 25 The FMSS is scored based on five categories: initial statement, relationship, criticism, dissatisfaction, and emotional over-involvement. Based on the scoring on the five categories, each participant is categorized into exhibiting high, borderline, and low expressed emotion. Participants are categorized in high expressed emotion if they score high on criticism, hostility, dissatisfaction, and emotionally over-involved tendencies based on their speech samples.
KCSS
Kilik and Hopkins developed the KCSS. 26 It assesses the family caregivers perceived level of stress during the process of caregiving. The overall score is the sum of the individual’s responses to each statement. The score ranging from 10 to 14 indicates a mild stress level, 15 to 23 indicates a moderate level of stress, and 24 to 50 indicates a severe stress level. Cronbach’s coefficient alpha is 0.89 and internal consistency between the caregiving and the family domain is 0.88 and 0.88, respectively.
WADL
Maenner et al. 27 developed The WADL to assess the level of self-sufficiency through the child’s activity of daily living reported by their primary caregivers. The item scores are summed to produce an overall score. The higher the score, the higher the level of self-sufficiency and the lower the score, the lower the level of self-sufficiency in daily living activities. Cronbach’s alpha ranged from 0.88 to 0.94. Test–retest reliability with weighted kappa’s is between 0.92 and 0.93.
Results
The collected data were scored and interpreted against the tools’ standardized norms. The FMSS was transcribed and analyzed for content and scored based on the FMSS manual. Thematic analysis suggested by Braun and Clarke 28 was used on the participants’ speech samples to identify initial codes and emerging themes that determine the factors influencing expressed emotion. The data was statistically analyzed using the Statistical Package for Social Sciences (SPSS) version 20 software. The chi-square test for association was employed to examine the association between expressed emotion and caregivers’ stress and expressed emotion and their child’s self-sufficiency in activities of daily living (ADL) and Pearson’s correlation was employed to examine the relationship between caregivers’ stress and self-sufficiency level.
Thirty-five primary caregivers of children with NDD participated in the study out of which nine are primary caregivers of children with learning disability, autism, and intellectual disability and eight are primary caregivers of children with cerebral palsy. All primary caregivers who participated in the current study were mothers.
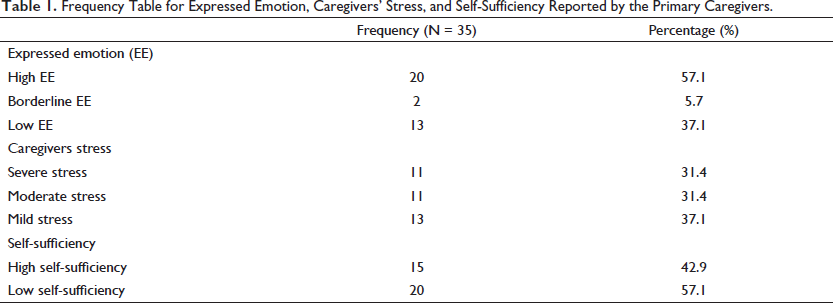
From Table 1, it can be inferred that 20 out of 35 (57.1%) primary caregivers of children with NDD exhibited high expressed emotion, by showing negative expressed emotion such as high criticism, hostility, or emotional involvement towards their children. It can also be observed that 11 out of 35 primary caregivers (31.4%) scored moderate, 13 scored mild (37.1%), and 11 scored severe (31.4%) on levels of caregivers’ stress. Concerning self-sufficiency in activities of daily living, 20 primary caregivers (57.1%) reported low levels of self-sufficiency in ADL, indicating that the children diagnosed with NDDs could not carry out activities of daily living independently and required the caregiver’s assistance. On the other hand, 15 caregivers (42.9%) reported high levels of self-sufficiency in ADL by their children, indicating their child’s ability to carry out ADL independently without assistance.
Frequency Table for Expressed Emotion, Caregivers’ Stress, and Self-Sufficiency Reported by the Primary Caregivers.
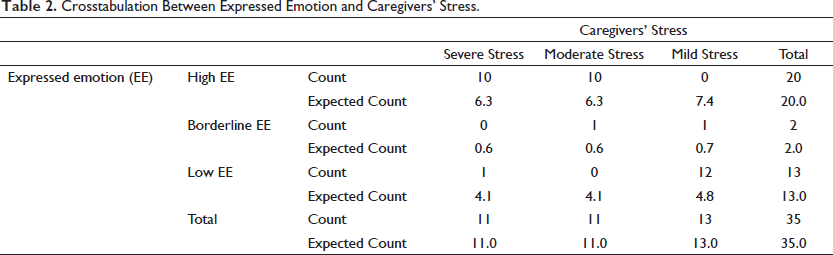
From Table 2, it can be inferred from the cross-tabulation that most of those primary caregivers who scored moderate to severe on caregivers’ stress exhibited high expressed emotion and those who scored mild on caregivers’ stress exhibited low expressed emotion.
Crosstabulation Between Expressed Emotion and Caregivers’ Stress.
A chi-square test of association was performed to examine the association between expressed emotion and caregivers’ stress. From Table 3, it can be inferred that Pearson’s chi-square value violates the assumption of the chi-square test, that is, more than 20% of cells have expected values <5. 29 Therefore, the likelihood ratio value was adopted (i.e., 39.129, df = 4, p = .000, p < .05). The findings indicate that there exists a significant association between expressed emotion and caregivers’ stress. This suggests that the display of expressed emotion by the caregivers of children diagnosed with NDD is associated with the experience of stress in caregivers.
Association Between Expressed Emotion and Caregivers’ Stress.

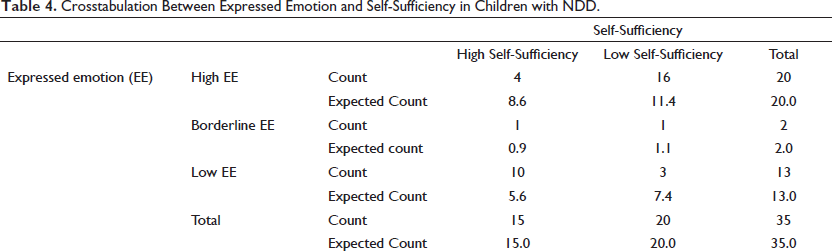
From Table 4, it can be inferred that self-sufficiency in activities of daily living in relation to expressed emotion, most primary caregivers who exhibited high or borderline levels of expressed emotion reported low levels of self-sufficiency in their children. Notably, those who reported high levels of self-sufficiency exhibited low levels of expressed emotion.
Crosstabulation Between Expressed Emotion and Self-Sufficiency in Children with NDD.
A chi-square test of association was performed to examine the association between expressed emotion and self-sufficiency in ADL in children diagnosed with NDD as reported by the primary caregiver. From Table 5, it is evident that Pearson’s chi-square value violates the assumption of the chi-square test, that is, more than 20% of cells have expected values <5. 29 Therefore, the likelihood ratio value was adopted (i.e., 10.970, df = 2, p = .002, p < .05). The findings indicate a significant association between expressed emotion and self-sufficiency in children with NDD.
Association Between Expressed Emotion and Self-Sufficiency in ADL in Children with NDD.

From Table 6, it can be inferred that there is a significant negative correlation (r = –0.433, p = .009, p < .05) between caregivers’ stress and caregiver-reported self-sufficiency in activities of daily living. This indicates that with an increase in the level of self-sufficiency in children, there is a decrease in the level of stress experienced by the caregiver.
Pearson’s Correlation Coefficient Between Caregiver Stress and Self-Sufficiency in ADL.

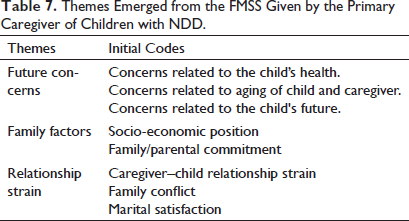
From Table 7, it can be inferred that in addition to the five dimensions, initial statement, relationship, criticism, dissatisfaction, and emotional overinvolvement assessed through the FMSS to explore expressed emotion; three major themes emerged from the speech samples of the participants to identify the factors influencing expressed emotion within families of children with NDD. The three major themes include future concerns, family factors, and relationship strain.
Themes Emerged from the FMSS Given by the Primary Caregiver of Children with NDD.
Future Concerns
Mothers of children diagnosed with NDD held worries and concerns about their own and their child’s future. Future concerns relating to their career and financial independence and their child’s career and settlement. The main future concern amongst most mothers was their worry for their child during their old age or after their death.
“I sometimes feel clueless and worried about my child’s future." I don’t know who will take care of him after me,” reported a mother of a 13-year-old child diagnosed with Intellectual disability. “I don’t know if he will be able to be in a position to take care of himself with the given condition. If only I had answers to all my questions,” remarked a mother of a 12-year-old child diagnosed with mild autism and seizures. “I quit my job and don’t think I’d ever return and join the workforce. I want to devote all my time to providing the best for my son,” Narrated a mother of a 10-year-old child diagnosed with Cerebral Palsy.
Family Factors
Most mothers reported financial problems as one main setback in treating their children with NDD. They said that services such as occupational and speech therapy sessions are expensive, and the family could not afford those services.
“I feel frustrated and angry with myself that I do not have enough money to treat my child properly,” described a mother of an 11-year-old with Cerebral Palsy and seizures. “I feel helpless that I am not being able to provide him with the best treatment, and this sometimes gets converted into anger towards him and his health problem,” conveyed, a mother of a 12-year-old child diagnosed with cerebral Palsy and has a co-morbid condition of epilepsy.
From the speech sample, it can also be deciphered that lack of parental knowledge about the condition and lack of parental or family involvement or commitment to the child’s condition and its related treatment were crucial factors in the exhibition of negative expressed emotion towards the child.
“I get so angry when he does not listen to me. I feel like he is doing it intentionally without putting in the effort, which frustrates me,” commented a mother of an 11-year-old child diagnosed with Learning Disability. “Although the doctors tell me he would take time to process the information, I sometimes lose my patience,” described a mother of a 14-year-old child diagnosed with Learning Disability.”
Relationship Strain
The final theme that emerged from the FMSS was relationship strain. From the speech sample, it was evident that relationship strain between caregiver–child, caregiver–spouse in the form of marital satisfaction, and family conflict between other family members influenced expressed emotion of the primary caregiver or family members toward the child.
“Often, the anger and frustration are not just directed to him but also toward my husband, and we end up fighting,” reported a mother of a 14-year-old child diagnosed with Learning Disability. “My husband does not support me through the caregiving process but often blames me if something goes wrong or if I fail to look after the child even for a second. This makes me feel so disappointed,” reported a mother of a 10-year-old child diagnosed with Cerebral Palsy.
Discussion
This research aims to offer a glimpse of the expressed emotion exhibited by the primary caregivers towards their children diagnosed with NDD by associating it with caregivers’ stress and the child’s level of self-sufficiency in activities of daily living. The expressed emotion exhibited by the primary caregivers is a negative expressed emotion, such as criticism, emotional display, self-sacrificing actions or overprotection, and sharing of excessive details indicating undue worry and concern despite the slight presence of positive emotions in the speech such as positive initial statement, positive regard, and warmth. On the other hand, those primary caregivers who exhibit low or borderline expressed emotion showed absence or low level of criticism, hostility, emotional display, self-sacrificing, or overprotection and exhibited positive initial statements, relationships, and warmth towards their children.
The current study unveils that those primary caregivers exhibiting high expressed emotion reported higher caregivers’ stress. The findings were akin to the results of De Clercq et al.; 30 high emotional over-involvement, criticism, and low expression of warmth were associated with high levels of parenting stress. Similarly, those who scored mild on caregivers’ stress exhibited low levels of expressed emotions representing low expressed emotion as an indicator of a positive family climate and reduced stress. Another notable finding suggests that parents with high expressed emotion experience high-stress levels and reported using less support and advice outside the family than parents with low expressed emotion. 31 Therefore, hypothesis (H1), which states that there is a significant association between expressed emotion and caregivers’ stress, is accepted. A similar study on non-clinical children revealed that parents exhibiting high expressed emotion reported higher family non-adaptive functioning, helplessness in caring for their child, and extreme parental stress. 32 In that case, the complexity for families of clinical children diagnosed with NDDs or any form of disabilities is much higher and must be further studied and intervened.
With regard to expressed emotion and self-sufficiency, primary caregivers who exhibited high expressed emotion reported a low level of independence in their children. This suggests that the display of expressed emotion in the form of criticism or emotional over-involvement by the parents or primary caregivers is highly associated with the level of self-sufficiency in activities of daily living in children. Therefore, hypothesis (H2), which states that there is a significant association between expressed emotion and self-sufficiency, is accepted. In the current study, it is observed that those caregivers who reported high levels of self-sufficiency in their children reported lower levels of stress and exhibited low expressed emotion. The findings are consistent with a similar study in which a significant negative correlation between activities of daily living, caregiving burden, and expressed emotion was identified. 33 Expressed emotion displayed in the form of warmth, criticism, hostility, or overinvolvement towards their child is closely associated with the extent to which the adolescents are self-sufficient in carrying out activities of daily living independently (e.g., taking a shower, eating on their own, dressing up, etc.).
Similarly, the findings reveal a negative relationship between caregivers’ stress and self-sufficiency in activities of daily living of their children.This suggests that with an increase in the level of self-sufficiency in children, there is a decrease in the level of stress experienced by the caregiver and vice-versa. Therefore, hypothesis (H3), which states that there is a significant relationship between caregivers’ stress and caregiver-reported self-sufficiency in children, is accepted. Furthermore, the findings demonstrate that when children are more capable in carrying out daily activities independently, caregivers experience less stress. The Stress Process Model by Pearlin et al. 34 proposed that objective stress, such as assisting the individual with ADL and managing behavioral and psychological symptoms, is related to subjective caregivers’ stress (such as role overload or burden). Therefore, the lower the level of self-sufficiency in a child diagnosed with NDD, the higher the level of strain experienced by the primary caregivers to help them with their essential needs.
In addition to quantitative analysis, exploring expressed emotion exhibited by primary caregivers towards their child with NDD, qualitative data were utilized to expand the understanding of critical factors influencing expressed emotion within families. The FMSS obtained from the caregivers revealed vital factors such as future concerns, family factors, and relationship strain as prime considerations for exploring expressed emotion within the family.
Future concerns related to the aging of the child and oneself, and caregivers’ concerns related to the child’s future were central for determining the expressed emotion of primary caregivers toward their child. This indicates that the caregivers could experience future anxiety, which is defined as “a negative emotional state and the experience of fears, uncertainty, and threats connected with the subjective representation of events and states in a distant future.” 35 The future concern could be displayed as negative expressed emotions such as self-sacrifice and emotional over-involvement towards the child by their mother. Although some caregivers reported strong optimistic beliefs and future expectations of their children, 36 most caregivers exhibited worry, concerns, and anxiety related to their own and their child’s future.37–39 Few studies reported that mothers of children with developmental delays reported higher levels of future anxiety about their future health and their ability to provide care and meaning in life in comparison to mothers of children with typical development.40, 41
Family factors such as socioeconomic positions and family/parental commitment could also play an imperative role in expressed emotion within the family. Low-income households reported more significant distress within the family. 42 Mothers of children with NDD belonging to low socioeconomic status exhibited high negative expressed emotions such as hostility and criticism. Disrupted family cohesion, parental criticism, and aggressive parental disciplinary behavior result in trauma, behavioral problems, and the diagnosis of specific conditions such as attention deficit hyperactivity disorder, mood disorder, oppositional defiant disorder, and physical abuse in children and adolescents.43, 44 In contrast, a family with knowledge and awareness about mental illness and showing parental involvement and commitment exhibited positive expressed emotions with warmth and positive regard. 45
Relationship strain between caregiver–spouse, the relationship between caregiver and child, and family conflict that revolves around the child and their disability also contribute to expressed emotion within the family. Parents of children with NDDs were found to be at increased risk of conflicting and unsatisfied relationships.46–48 Satisfactory family and marital environment are linked to low expressed emotion. In contrast, extreme family conflicts were linked to high expressed emotion. 49
Based on the analysis of the FMSS, it is evident that the expressed emotion exhibited within the family and between the primary caregivers and the child is influenced by numerous personal and systemic factors. Identifying and directing attention toward each factor affecting expressed emotion could be strenuous. However, regulating the negative expressed emotions within the family by identifying the triggers, labeling, monitoring, and adopting self-soothing strategies could improve positive interaction and communication within the family. 50
Conclusion
This study aimed to provide insight into expressed emotion and its association with caregivers’ stress and self-sufficiency in activities of daily living in children with NDD. The study findings indicate that most primary caregivers exhibited high expressed emotion, often involving unpleasant and negative emotions such as criticism, overinvolvement, and self-sacrifice. Those caregivers showing high expressed emotion reported high levels of caregivers’ stress and low levels of self-sufficiency in activities of daily living in their children. Caregivers with moderate to severe stress reported lower levels of self-sufficiency in activities of daily living in their children. The qualitative analysis of the FMSS revealed that factors such as future concerns, socioeconomic status, family dynamics, family commitment, and relationship strain could significantly influence the expressed emotion within the family.
Limitations
The analysis was limited to the data that were collected from a small section of primary caregivers providing care to children with certain NDDs. The primary caregivers providing care for other forms of chronic physical and mental health conditions were not included in the current study. Mothers providing primary care for children with NDD participated in the study, but expressed emotion of other family members providing care was not explored. A potential threat to the trustworthiness and credibility includes that primary caregivers may have provided a viewpoint that they believe is pleasing to the interviewer. However, to obtain reliable data, the researcher assured the participants of utmost confidentiality and anonymity with a non-judgmental and safe space to express honestly.
Future Implications
This study could help mental health and other allied health professionals work collaboratively with children and caregivers to treat NDDs and develop strategies to improve positive family interaction. Emphasis on the psychological needs of parents or primary caregivers of children with NDDs is the need of the hour. The intervention and strategies for the child’s effective treatment outcomes, caregivers’ well-being, quality of parent–child interaction, and family dynamics could be more appropriate and beneficial for caregivers and their child than the conventional child-centric interventions provided in special schools and neurodevelopmental or rehabilitation centers. It is vital to focus on caregiver-centric and family-based intervention centering on improving expressed emotions and their associated outcomes that focus on enhancing the family interaction, caregivers’ well-being, and the child’s treatment outcome.
Footnotes
Acknowledgements
The authors of the study would like to thank the primary caregivers of children with NDDs for their participation and cooperation in conducting the research. The authors also extend their gratitude to the authorities of the universities for offering support and resources throughout the investigation.
Authors’ Contribution
All authors contributed to the research formulation and execution. KPB performed research problem formulation, data collection, and analysis. Analysis of data, duplication check, reviewing, and finalization of the final draft were performed by MB.
Statement of Ethics
The research adheres to the International Committee of Medical Journal Editors (ICMJE) and World Health Organization (WHO) guidelines for conduct, reporting, editing, and publication. The current study is a part of the author’s doctoral research study. The Institutional Ethical Committee for Studies on Human Subjects (IECH), Vellore Institute of Technology, Ref. No. VIT/IECH/XIII/2022/04c has approved the proposed title for the doctoral research focusing on the biopsychosocial concerns and well-being of the primary caregivers of children with NDD.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Verbal informed consent was taken from the primary caregivers to participate in the study as the researchers and the participant did not meet in person. Participants were informed of the anonymity of their identity and confidentiality of their responses and the voluntary nature of the study.