
Abstract
Background
Amidst the caregiving stressors that primary carers experience while providing care for their child with a neurodevelopmental disorder (NDD), the perception of having family, friends and significant others to support and navigate difficult situations would enable the carers to cope effectively during caregiving. Among a couple, raising a child with special needs, it is imperative to have spousal support that helps in navigating through the marital relationship.
Purpose
Oftentimes, when a child with a disability is born into a family, due to a lack of readiness and mutual support among the spouses, it results in marital and familial conflicts leading to divorce or separation. Thus, the study attempts to explore the perceived social support among the parents of children with NDDs and delve deeper into the narratives of single mothers, either divorced or physically separated, and the challenges that they experience in providing care for their children in the absence of spousal support.
Method
One-hundred fifty parents (99 mothers and 51 fathers) were administered the Multidimensional Scale of Perceived Social Support Scale (MSPSS) to assess the perceived social support followed by an interview of 12 single mothers to gain insights into the lived experiences and challenges faced by single mothers while providing prolonged care for children with NDDs.
Results
There exists no significant difference between perceived social support and sociodemographic profiles of parents such as gender, age, family types, occupation, hours spent providing care and primary diagnosis of the child. The findings indicate that all single parents were mothers and themes such as sole parental responsibilities, lack of support from spouse and in-laws, poor physical and mental health and lack of marital stability emerged from the interview deciphering challenges experienced as a single mother.
Conclusion
The study highlights the importance of implementing effective policies that support single mothers who are divorced, abandoned or separated while providing care for their child with a disability.
Keywords
Introduction
The birth of a child is an eager expectation in the family. Parents and family hold an abundance of hopes, desires and dreams when a child is born. However, it turns out to be a shocker when the child is born with a disability or condition, crashing down the parents’ dreams and expectations for the future. 1 The behavioural and functional capabilities of children diagnosed with neurodevelopmental disabilities gradually change across the lifespan as they transition from childhood into adolescence and adulthood; however, few disabilities are permanent 2 and these children would require assistance throughout their lives. 3
Neurodevelopmental disorders (NDDs) are defined as a group of conditions with onset during infancy, childhood or adolescence and result in significant impairment in everyday functioning. 4 Providing support and primary care for such children is often viewed as the responsibility of the parents. As primary caregivers, parents of children diagnosed with NDDs undertake a long-term commitment, which can extend throughout their lives. 5 Parenting a child with special needs is not the same as parenting a normal child as the former involves consistent planning, scheduling appointments, therapy, arranging special transportation, and being vigilant about medical emergencies, harmful behaviours and autistic meltdowns. 6
Exposure to endured caregiving has physical and psychological impacts on primary carers 7 and research findings illustrate that parents providing care for children with NDDs are at greater risk of experiencing early mortality, 8 health problems 9 and mental health issues than parents who do not have children with disabilities or chronic conditions. 10 A child with a disability within a family could result in various stressful situations such as financial burden, psychosocial problems and relationship strain between parents. 11 Positive reappraisal, social support, family adaptation, effective coping and adaptive functioning act as a catalyst to improve the health and psychosocial well-being of carers.12, 13 Social support is an effective coping resource that describes how an individual copes with stress and adapts to the situation. 14 Social support encapsulates the help, assistance and support received by primary care providers from their spouses, family, friends and the community. 15 It plays an imperative role in relieving stress 16 and improving physical and psychological health. 17 Parents often experience social isolation from family and community while providing care for their children with special needs. 18
Beyond all the social support received, spousal support plays a significant role in the navigation of the marital relationship while providing care. The presence of spousal support shows good marital quality among mothers of children with autism and is associated with improved adjustment, caregiving efficiency, well-being, 19 and enhanced physical and mental health functioning among mothers of critically ill children. 20 However, less is known about the details of the parents’ marital relationship leading to divorce or separation while providing care for children with special needs. It is disheartening to identify research studies indicating a higher rate of parental divorce, separation and marital discord among parents of children with disabilities in comparison with parents of children with normal development. 21 Marital life of parents of children with developmental disabilities is often revealed as strained, dysfunctional, conflicting, lacking marital adjustments and satisfaction and resulting in divorce or separation. 22 On the contrary, other studies have found no risks of divorce 23 and no identified difference in marital status among parents of children with developmental disabilities in comparison with parents of children with no developmental disabilities. 24
Study Rationale
Amidst the discussion on risk versus no risk for divorce or separation among parents of children with NDDs, it is crucial to gaze at the perspectives that divorce holds in a country like India. Divorce is still a social taboo in India, 25 and often people turn their heads away from having conversations on such a stigmatised topic. Clarity on dysfunctional families, marital adjustment, marital satisfaction and family conflicts among parents and family members arising from caregiving are established through research findings.26–28 Nevertheless, the risk of divorce or separation and challenges experienced by single parents of children with developmental disabilities are not clearly defined and understudied in India. Therefore, this study strives to gather data from parents of children with NDDs regarding the extent to which they perceive the presence of social support. In the second phase, these parents were filtered to include parents who were divorced or separated to explore the lived experience of being a single mother with a lack of spousal support in providing care and its impact on the psychological and social experience among the carers.
Objective
The study aimed to evaluate the level of perceived social support received by parents identified as primary carers of children with NDDs and explore the phenomenological experience focusing on the challenges faced by single mothers of children with NDDs.
Hypothesis
The hypothesis was formulated to test the phase 1 quantitative research data:
Methods
Research Design
A mixed-method research design was used. A quantitative research method was used to assess the level of perceived social support among parents identified as primary carers and qualitative research was conducted to explore the lived experience and challenges faced by single mothers of children with NDDs.
Participants
The study was conducted in two phases. In the first phase, 150 parents (99 mothers and 51 fathers) of children with NDDs involved in the primary care of the child with NDDs as per the Right to Person with Disability (RPWD) Act in India, 2016 were included. The disorders included autism spectrum disorders (ASD), intellectual disability (ID), specific learning disability (SLD), cerebral palsy (CP) and its related co-morbidities, such as speech and language disability, attention-deficit hyperactivity disorder (ADHD) and neurological conditions such as epilepsy and seizures were selected. A purposive sampling technique was used to recruit the parents. The inclusion criteria were parents between the age group of 25 and 55 providing primary care for children diagnosed with NDDs aged between 6 and 18 years for at least two years or more. The exclusion criteria were parents caring for children with other NDDs related to the nervous system not specified by the RPWD Act, 2016, and providing care for another significant person diagnosed with a chronic illness. In the second phase, 12 single mothers either divorced or physically separated, and providing care for their children with NDDs were interviewed.
Procedure
The parents were recruited from three established non-profit special schools registered under the Government of India, located in Chennai district, Tamil Nadu, India. The administrative authorities of the following special schools were approached, and permission was sought. Written informed consent was obtained from parents who consented to participate in the study. In the first phase, the parents were administered the Multidimensional Scale of Perceived Social Support (MSPSS). In the second phase, the parents who fulfilled the criteria of being a single parent, either divorced or physically separated, and providing care for their child with NDD were interviewed face-to-face using a semi-structured interview schedule. Questions were asked to elucidate caregiving experiences and challenges as a single parent. Data accuracy and credibility were ensured through response summarisation and participant validation.
Data Collection
The MSPSS was administered to assess the level of perceived social support among parents (either mother or father) providing primary care for children with NDDs. The questionnaire was administered to 150 parents (99 mothers and 51 fathers) of children with NDDs related to the nervous system and followed by a one-on-one interview with 12 single mothers who are providing care for their children with NDDs identified from the phase 1 study. The interview schedule was prepared by the researcher, who is a qualified counselling psychologist, holding a master’s degree in counselling psychology. The interview schedule was content validated by another counselling psychologist before initiating the interviews. Each one-on-one interview lasted for an average of 20–25 minutes. Each interview was recorded by the researcher by taking field notes.
Caregiving-related experience questions were asked to the single mothers focusing on challenges experienced in the absence of spousal and family support. The eight semi-structured interview questions include: (a) What are the challenges that you face as a single parent providing care for a child with special needs? [Probe for challenges as a single parent in the absence of spouse and family] (b) Could you narrate the situation that led to the divorce or separation of you and your partner? (c) Can you describe in detail the different types of support that you receive while providing care? [Probe for the presence of social support as a single parent from family, friends, and significant others] (d) What are some instances during which you’ve felt a lack of support from your family, friends, and significant other? [Probe for lack of social and family support among single parents] (e) How do you think the situation would have been different if you received spousal support? [Probe for spousal support] (f) How do family members support you during caregiving? [Probe for support from family and in-laws] (g) How did lack of social support from spouse and family affect you? (h) Do you feel socially isolated as a single parent providing care? If yes, what are the instances during which you felt socially isolated? [Probe for social isolation, and loneliness]
Measures
Sociodemographic Details
The sociodemographic details of each parent such as age, gender, occupation, relationship with the child, family type, time spent providing care, and child’s information such as age, gender, and diagnosed neurodevelopmental condition, and other necessary details were obtained before the administration of the questionnaire.
Multidimensional Scale of Perceived Social Support
The MSPSS was developed by Zimet and Colleagues. 29 It is a brief questionnaire to measure the perception of social support from three sources: friends, family, and significant others. The scale consists of 12 items with 4 items for each subscale. The validation of the scale was conducted on 270 family carers of people with dementia and the internal consistency for the total score was α = 0.92 and three subscales (α = 0.92–0.94). The test-retest reliability was excellent for the total score r = 0.90 at 95% confidence interval (CI) and subscales r = 0.84–0.89. The mean score was calculated by summing the total scale and each subscale item and dividing by 12 and 4 (total number of items), respectively. A score of 1–2.9 indicates low support, 3–5 indicates moderate support and 5.1–7 indicates high support.
Data Analysis
The obtained data were analysed using the Statistical Package for the Social Sciences (SPSS), IBM® SPSS® Statistics version 23.0. The numeric data was analysed through descriptive statistics such as percentage, mean and standard deviation and inferential statistics such as independent sample t-test, analysis of variance (ANOVA) test and Pearson product-moment correlation. The qualitative data was analysed by using the thematic analysis suggested by Braun & Clarke. 30
Results
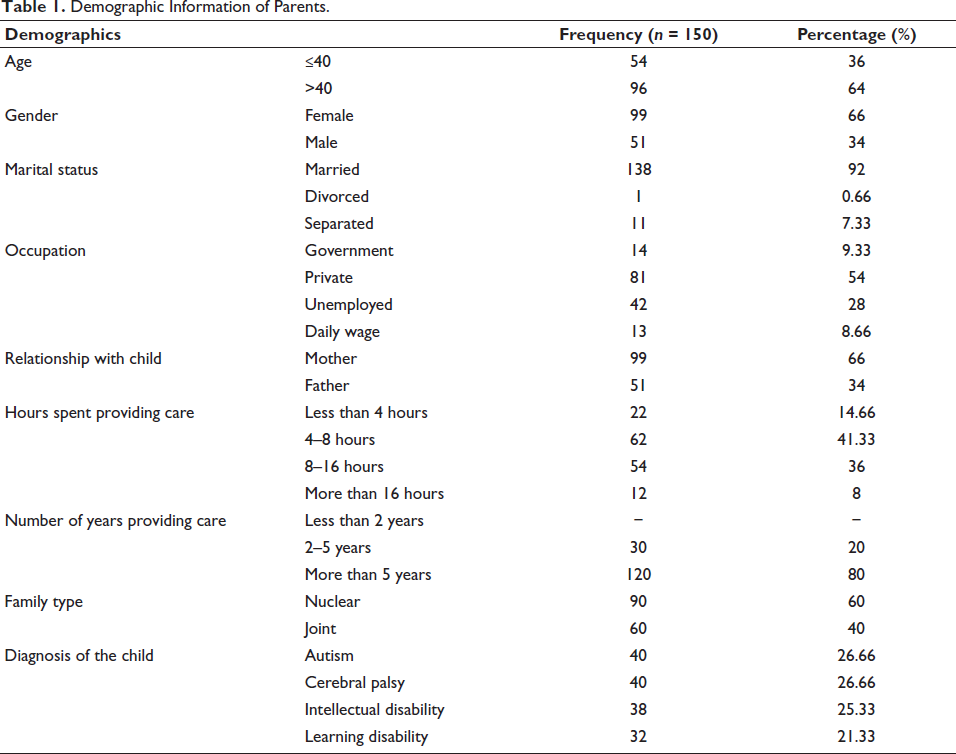
Table 1 indicates that the majority of the parents who identify themselves as primary carer who have participated in the study are female (n = 99), with the maximum number of parents working in the private sector (n = 81), providing care for 4–8 hours (n = 62) or 8–16 hours (n = 54), living in a nuclear family setup (n = 90), and providing care for children with following NDDs such as autism (n = 40), CP (n = 40), ID (n = 38) and learning disability (n = 32). Out of 150 parents, 12 parents are single mothers who are divorced (n = 1) or separated (n = 11).
Demographic Information of Parents.
An independent sample t-test was conducted to compare the level of perceived social support among gender, age groups and family types. Table 2 indicates that there exists no significant difference in the level of perceived social support between the genders of the parents (P > .05). Similarly, there exists no significant difference among caregivers who are less than or equal to or above 40 years and belong to a joint or nuclear family setting. The mean scores indicate that they pose moderate perceived social support (i.e., mean score ranging between 3 and 5).
The Mean Difference of Perceived Social Support Among Demographic Variables.
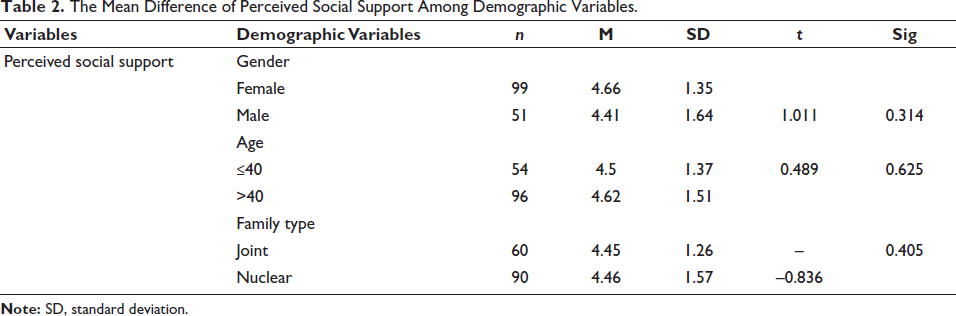
Note: SD, standard deviation.
ANOVA test was conducted to compare perceived social support with various occupations, hours spent providing care and the primary NDD diagnosis of the child. Table 3 shows that perceived social support did not differ among caregivers providing care for different durations, enrolled in various job roles or unemployed and caring for children with different NDDs (P > .05).
Perceived Social Support and Demographic Variables Hours Spent Providing Care, Occupation and Primary Diagnosis of the Child.
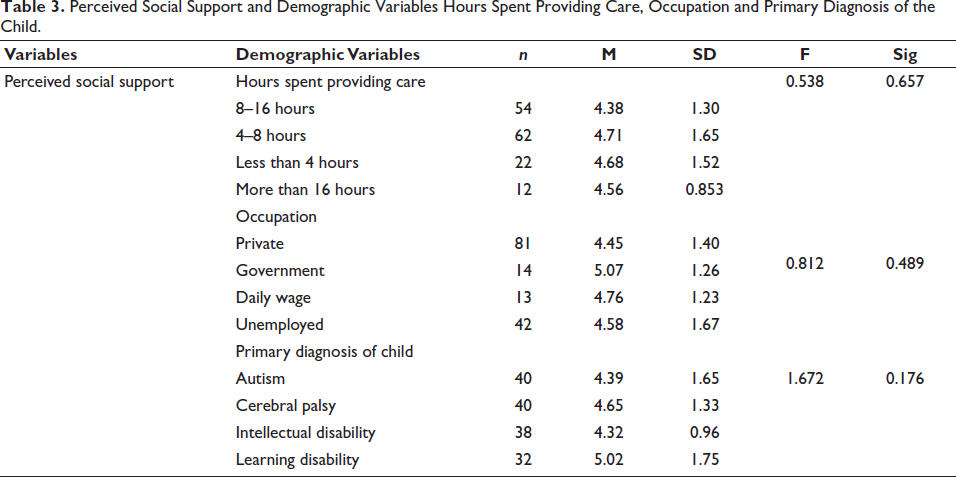
Table 4 shows that all the single parents identified from the survey for participation in the one-on-one interview included single mothers (n = 12) providing care for children with three major NDDs including autism (n = 6), CP (n = 3), and ID (n = 3), out of which only one was divorced and rest were physically separated (n = 11).
Demographic Information of Single Parents Participating in Phase 2 of the Study (Interview).
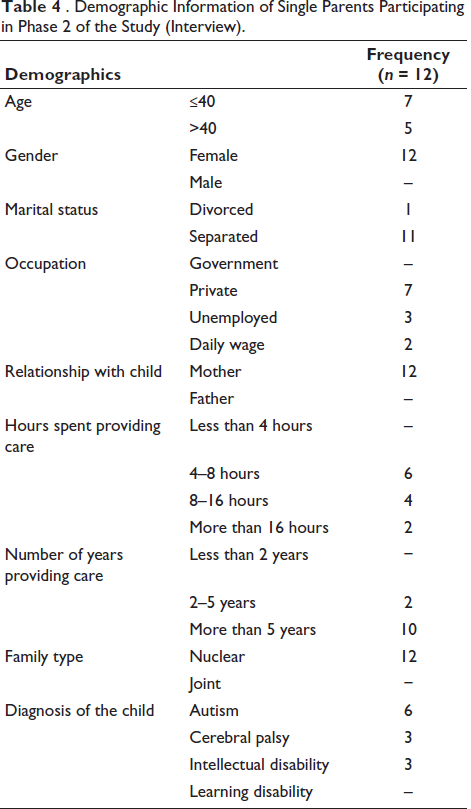
Table 5 shows the themes and sub-themes emerged from the qualitative data.
Themes and Sub-themes Emerged from the Qualitative Data.
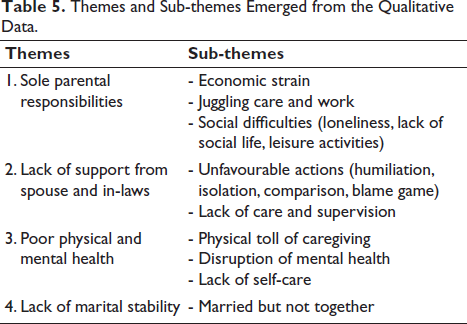
The following emergent themes and sub-themes were derived from the one-on-one interview conducted with single mothers providing care for children with NDDs and are discussed meticulously below.
Theme 1: Sole Parental Responsibilities
As a single parent, the sole responsibility of providing care and fulfilling the child’s needs would lie on the parent providing primary care. This could cause difficulty in being able to keep up with financial needs, juggling between work, home, and care and engaging in social leisure activities.
Economic Strain
Single mothers face difficulties in fulfilling the monthly needs of their children and home expenditures with the payments that they receive from work or through financial support from the family.
My salary alone is not sufficient for covering the expenses of home and my sons’ monthly expenses for treatment and therapy. (Mother of a child with autism) The medicines are very expensive and my source of income is not enough. (Mother of a child with cerebral palsy) I do not receive any financial support from my husband or his family, and although my family is ready to help, I feel hesitant to ask them. (Mother of a child with intellectual disability)
Juggling Between Care and Work
The absence of no one to support during caregiving makes it difficult for single mothers to juggle between care and work.
I have no one at home to look after my child, I had to quit my full-time job. I currently do a part-time job in the evening, that’s also challenging. (Mother of child with autism) My workplace doesn’t understand my situation that I will need flexible work hours as I care for a child with a disability that too without a partner to support. (Mother of a child with intellectual disability) I don’t have anyone at home to take care of my child and the little I earn through the part-time job is not enough. (Mother of a child with autism) I am grateful that my workplace understands my situation and supports me but sometimes work and providing care together gets overwhelming. (Mother of a child with cerebral palsy)
Social Difficulties
Single mothers providing care for a child with special needs may have to constantly supervise their child, due to which they may have to let go of their social leisure activities with friends or avoid attending any social gatherings such as weddings.
Few other mothers at my child’s special school talk about taking a break for themselves while their husband looks after the child, I am less privileged to take such breaks and connect with my friends. (Mother of a child with intellectual disability) I have to be home by evening after picking up my child from school and weekends are completely for him, in this scenario, there is no opportunity that I can attend team lunch with my colleagues. (Mother of a child with autism) My husband and I live separately, I often feel my daughter’s condition hasn’t impacted his work or social life as much as it has affected mine. Every decision that I take includes my daughter’s safety and comfort because of which I always avoid religious and family gatherings. (Mother of a child with autism) I don’t remember the last time I attended a wedding or went out for leisure. (Mother of a child with cerebral palsy)
Theme 2: Lack of Support from Spouse and In-laws
Most mothers reported that when a child with a disability is born into the family, the sole reason for the cause is blamed on the mother and she perceives a lack of support and kindness from her spouse and family.
Unfavourable Actions
Most mothers conveyed that their spouse and in-laws showed unfavourable actions towards them in the form of blaming, humiliating, comparing their child with another child and isolating the child and mother during social gatherings which made them feel isolated, humiliated and unloved. These initial unfavourable actions transformed into abandonment by the spouse and their family or the mother choosing to leave the family.
My mother-in-law often used to taunt and humiliate me for my child’s condition. She keeps telling me I am cursed, I had no choice apart from leaving that house. (Mother of child with cerebral palsy) I would have been happy if my husband supported me when my in-laws went against me but he also left me. (Mother of a child with autism) My husband stays in his parent’s house and I stay with my child in my parent’s house. He and his family do not support anything related to my child. It’s better we get divorced than live separately. (Mother of a child with autism) My child is often compared with my husband’s brother’s son, no one supported me so I chose to leave. (Mother of a child with intellectual disability)
Lack of Care and Supervision
Single mothers of children with special needs also felt that there was a lack of care and supervision for their child by other members of the family, especially their in-laws.
I was staying in a joint family at my husband’s place, despite having so many people at home, I never received any help or support to care for my child and I had to quit my job. (Mother of a child with CP) My husband did not even support me, he left for work and was never available to support and his parents often blamed me for everything and never helped me to look after my son. (Mother of a child with autism) Two years back my child fell from the wheelchair and my in-laws did not even care to help him despite seeing until I realised and came running. I could never trust them and leave my child with them. (Mother of a child with cerebral palsy)
Theme 3: Poor Physical and Mental Health
Most single mothers reported experiencing physical and mental health issues due to continued caring for their children with special needs, especially in the absence of spousal and family support.
Physical Toll of Caregiving
Endured caregiving for children with special needs especially issues with motor coordination could result in physical strain among parents. Most single mothers reported having body aches and pains as a result of assisting their child with mobility and activities of daily living (ADL).
Most of the time, I find it difficult to carry out routine activities of my child and I am unable to ask my aging mother for help. She is doing the little help that she can. (Mother of a child with autism) If only I had someone to help me through this when I fall sick, there is no one apart from me to take care of my child. (Mother of a child with cerebral palsy) Aches and body pain have become a part of my life now as I continue to care for my son. My body is no more supporting me to provide care single-handedly. (Mother of a child with cerebral palsy) I was abandoned by my husband and family, yet I did not lose hope, but now as I am getting older and unwell, I fear who will look after my child. (Mother of child with intellectual disability)
Disruption of Mental Health
Single mothers collectively expressed their worry about their child’s future and also worried about their child’s situation after their life as most of them independently look after their children without spousal and familial support.
I often worry a lot and also get anxious about my child’s future. What will happen to him once I am gone. (Mother of a child with intellectual disability) Sometimes I am unable to sleep worrying about my daughter and feeling helpless about our situation. I feel all alone. (Mother of a child with autism) I often experience an emotional breakdown and don’t have anyone to console me, especially my partner. (Mother of a child with cerebral palsy) There are days when I don’t feel like doing anything at all, I feel completely isolated and alone, the only reason I am living is for my daughter. (Mother of a child with autism)
Lack of Self-care
Self-care seems like an unattainable luxury among single mothers who are unable to share their caregiving role with another person to prioritise and take care of their physical and mental health.
I have completed a fashion designing course, and it’s my passion to design dresses, so when my son is asleep I try to stitch some and it makes me happy and helps me get distracted from my usual routine. If only my spouse and family supported me properly, I didn’t have to do this all by myself. (Mother of a child with autism) At this point being a single mother, I can only care for one person and that’s my daughter taking care of myself takes a back seat. (Mother of a child with intellectual disability)
Theme 4: Lack of Marital Stability
Marital stability is remaining legally married without divorce, physical separation, or legal separation. However, most single mothers of children with NDDs conveyed that they lacked marital stability and were physically separated. Only one among the twelve mothers who participated in the interview was legally divorced. Almost all mothers conveyed that it was their husbands and their in-law family that initiated or forced them to separate through their actions.
Married but not Together
Most single mothers part of the interview expressed that they are physically separated from their spouses and their spouses never, rarely or occasionally visit their children.
I stay with my mother and daughter, when my daughter was diagnosed with cerebral palsy at three years old, my husband and in-laws did not even support me. Now, my child is 8 years old, and he sometimes occasionally visits her. (Mother of a child with autism) My husband abandoned me and my child, I moved from the village in search of a treatment facility for my son. I don’t even know where my husband is now. (Mother of a child with CP) He left us when he got to know my child will never get cured, he never returned and chose his family over our family. (Mother of a child with ID) My husband stays with his parents and continues to work, I quit my job, and I am looking after my son. He chose what was best for him and I chose what was best for me and my son. Sometimes he comes and visits him. (Mother of a child with autism)
Discussion
Keeping a marriage together while raising a child with special needs is often stressful resulting in poor psychological well-being 31 and requires continuous efforts and an optimistic viewpoint by both parents. 32 The feelings of guilt, resentment, anger and regret accompanied by actions of blaming, being impatient, and critical could make any of the parents feel left out or ineffective. 33 Mothers are often viewed through the lens of providing primary care by assisting the child with ADL such as grooming, showering, dressing and feeding, and fathers as carers focused on employment and income for providing financial aspects of caring. 34 Parents must work as a team to provide care for the child diagnosed with NDD, such that they are well-equipped to navigate the caregiving process as well as the marital relationship.
Rearing a child with special needs is extremely stressful both individually and within a marital relationship. The prevalence of divorce or separation is found to be alarmingly high in families of children with special needs. 35 However, divorce is still considered a social taboo in India. Separation is a common way in which legally married couples split up. Most often, separation may or may not be followed by divorce. Separation is more socially acceptable than adopting a complex legal battle. Thus, many Indians across diverse religions chose to be separated rather than divorced. 36 In this study, almost all single mothers reported being non-legally separated from their spouses except one who was legally divorced. A non-legal separation, also known as living separately, is different from a legal separation as the latter involves a formal decision from the court. However, non-judicial or non-legal separation has its de-limits such as not being able to have clarity on child custody and not receiving financial or any other form of support from the spouse and their family. 37 The findings of this study also reflect similar de-limits experienced by single mothers where fathers occasionally visit their children and do not provide support and financial assistance. Previous studies explored several domains of marital relationships among parents of children with special needs such as marital adjustment, marital conflicts, marital quality or satisfaction.38–41 Therefore, this study attempts to delve deeper by gaining insights into the narratives related to separation by exploring the perceived social support among primary carers and investigating the presence of social support by emphasising spousal support, familial support and the challenges experienced by single mothers of children with NDDs.
From the quantitative data collected from 150 parents providing primary care for children with NDDs during the phase 1 study, it is revealed that parents identifying as primary carers both mother and father reported moderate levels of perceived social support indicating no gender difference. This is contrary to the popular research findings that elucidate gender differences in perceived social support, 42 in which few findings reveal men having greater perceived social support than the female which is explained through socialisation experiences and gender roles carried out in a society,42, 43 and few results indicating the converse. There existed no significant differences in the level of perceived social support among other sociodemographic profiles of parents such as age, family type, occupation, hours spent providing care and the diagnosis of the child indicating that individuals from all diverse demographic profiles had perceived receiving social support to a similar extent. Therefore, hypothesis (H01) was accepted.
In phase 2 one-on-one interview, it is indicative that all the single parents in this study are mothers taking up sole responsibilities for providing care for their children with NDDs. Mothers being the primary carers and the sole responsibility being transferred to a mother when a child is identified with a disability make it difficult for them to navigate through the caregiving process. This indicates gender disparity in the role of caregiving where women are placed in the forefront as caregivers within the family. Women experience subjective burden, depression and enduring sadness, 17 while men experience greater stress due to the impact of caregiving on marital life and marital intimacy, leaving no quality time to spend with the spouse to openly express one’s emotions of sadness, rage and anger, causing strain in the relationship 44 due to which they abandon their family more frequently. 34 Most single mothers reported not receiving support from their husbands and in-laws and often felt alone in the caregiving process. They also reported that initiation of separation and abandonment was mainly from the spouse and the spouse’s family.
Based on the narratives, they experience an enormous amount of financial strain as a consequence of providing care. Most single mothers expressed the expensive nature of therapies and medications and their inability to meet them within the financial aid received from the government. 45 Single mothers rearing children with NDDs reported that they experience a lack of familial support and support from the community and government mainly financially to provide care.46, 47 They found it burdensome to juggle between work, caregiving and home but could not afford to quit their job. In addition, single mothers also felt that their social lives were stagnated and expressed their worry about not being able to attend social events and gatherings. They also conveyed their desire to participate in social activities like other women but communicated their dismay and helplessness due to the lack of spousal and familial support to care for the child in their absence. 48
Single mothers perceive a lack of support from their spouse and in-laws; they reported that initially it began through unfavourable actions towards the child and the primary carer (mother in this context) by humiliation and blaming the mother for the child’s disability and isolation of the mother and child from family gatherings. A similar study exploring the difficulties of mothers living with children with ID revealed that most mothers were blamed by their in-laws for their child’s disability and often felt lonely. 49 Most single mothers also reported a lack of care and supervision by family members which made it difficult for them to leave the child alone at home or unattended by trusting other family members. Mothers while staying with the spouse’s family perceived receiving lesser spousal support as their spouse worked outside for long working hours and were only involved in more logistical care tasks and did not engage in resolving conflicts arising within the family regarding providing care. 50
Single mothers providing care for children with NDDs face the dual challenge of providing for their families while managing challenges associated with caring for a child with a disability without the help of the spouse. 51 It is established that the experience of chronic stress and adverse health issues is common among parents of children with various NDDs. 52 They exhibit substantial physical and mental health symptoms that toil the body’s cardiovascular, immune and gastrointestinal systems along with the occurrence of psychological disturbances. 53 Perhaps, mental and physical health issues are even more intense among single parents providing care for a child with disability single-handedly without spousal and family support. 54 Self-care practices are important to have a balance between physical and mental health. However, as a single mother self-care is perceived as a luxury that cannot be afforded amidst caregiving. Most single mothers expressed their worry about not being able to pursue their hobby and passion as they do not have a significant other to support them through their pursuit.
Most single mothers conveyed about not being legally divorced but separated from their spouse for years due to conflicts that arose within the family regarding caregiving for the child with NDD. Among single mothers, reasons for choosing non-legal separation over legal divorce were explored which revealed that many families viewed divorce as unacceptable; therefore, they resorted to being physically separated. Single mothers reported greater abandonment by their husbands which left them stranded and clueless about their ability to provide care for their child alone. Based on the interview, it was evident that separated single mothers received limited or did not receive any support from their spouse, in-laws’ family as well as their own family. A few single mothers also expressed receiving support from their own family during separation and currently while providing care for their child but conveyed that the support was accompanied by occasional taunts, humiliation and conflicts making them feel extremely lonely within their own family. The challenges faced by single mothers highlight the imperative need for law enforcement across all communities for divorced or abandoned women or those who choose a non-legal separation and do not receive any support from their husbands or their family, 36 especially while providing care for a child with special needs.
Implications
The study would facilitate mental healthcare professionals and other allied health professionals to focus on identifying the problems and challenges faced by single mothers providing care for children with NDDs and formulating effective interventions and coping strategies to alleviate physical and psychosocial concerns. The findings of the study shed light on the importance of having marital and family counselling for parents and families of children with NDDs to enable efficacious marital adjustments and family adaptation while providing constructive care. Policies across the country should not only focus on the person with disabilities but also on the families providing care. This study highlights the imperative need to introduce caregiver-family therapy in India. The government should also be conscious of special cases such as single parenting of a child with a disability and provide financial aid to support their lives as a caregiver.
Limitations and Future Recommendations
The study focused on adopting a non-categorical approach for the selection of carers providing care for children diagnosed with distinct NDDs to facilitate diverse responses to understand carers’ experiences. Thus, bias in the findings due to heterogeneity in the listed disorders is possible. The study did not use audio or video recordings to collect the data to avoid hesitation among parents and to obtain more candid information, as participants were sharing personal and sensitive experiences. A small sample size representing parents of children with NDDs could limit the generalisability of the findings. Although only 12 single mothers out of 150 parents of children with NDDs were identified, it is imperative to understand the challenges faced by single mothers while providing care and caregiver research should emphasise on promotion of well-being among couples providing care for children with special needs. This study focuses on single mothers of children with NDDs, while future studies should consider single parents from diverse backgrounds providing care for other forms of chronic illnesses.
Conclusion
Most parents of children with NDDs perceived moderate social support. All the single parents identified through this study are mothers who took up the sole responsibility of caring for their children when faced with separation and abandonment by their spouse. Exploring in detail the challenges faced by the single mothers of children with NDDs in the absence of spousal support through qualitative analysis led to emergent themes such as sole responsibility, lack of support from spouse and in-laws, poor physical and mental health and lack of marital stability. The following themes encapsulated concerns faced by single mothers such as economic strain, juggling care and work, social difficulties, unfavourable actions by husband and in-laws, lack of care and supervision, the physical toll of caregiving, disruption of mental health, lack of self-care and strain in the marital relationship resulting in living separately.
Footnotes
Acknowledgement
The authors would like to extend their heartfelt gratitude to the primary carers and single mothers of children with NDDs for taking out time to fill out the questionnaire and cooperating for the one-on-one interview. The authors are also grateful to the management of the three special schools for providing permission to conduct the research. The authors would also like to thank the authorities of the university for offering support and resources throughout the investigation.
Authors’ Contribution
All authors contributed to the research formulation and execution. KPB performed research statement formulation, review of literature, data collection, analysis and manuscript drafting. Duplication checks, reviewing, analysis and finalisation of the draft were performed by MB.
Statement of Ethics
The research adheres to the International Committee of Medical Journal Editors (ICMJE) and World Health Organization (WHO) guidelines for conducting, reporting, editing and publication. This study is a part of the author’s doctoral program. The Institutional Ethical Committee for Studies on Human Subjects (IECH) has approved the proposed doctoral study focusing on the biopsychosocial concerns and well-being of the primary caregivers of children with NDDs.
Declaration of Conflicting Interests
The authors declare that the paper has not been submitted for publication or accepted for publication elsewhere. The manuscript has been read and approved by all the authors, the criteria for authorship have been met and each author approved that the manuscript represents honest work. The authors also declare that to the best of their knowledge, the article does not infringe any copyright or property rights.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written consent was taken from all the primary caregivers to participate in the current research. Participants were informed of the anonymity of their identity, confidentiality of their responses and voluntary nature of the study before obtaining consent.