
Abstract
Background
Schizophrenia is a life-shortening disease. The standardized mortality ratio has been higher than that of the general population, and it has doubled what it was 3-4 decades ago. This rise is mostly attributed to the increased cardiovascular risk associated with high second-generation antipsychotic (SGA) use. Evidence from the first-generation antipsychotic (FGA) era shows a lower prevalence of hypertension (HTN) but data regarding SGAs is scarce.
Purpose
The purpose of the study was to assess the prevalence of HTN and related factors using standardized methodology in patients with schizophrenia on treatment with SGAs.
Methods
A cross-sectional study through convenient sampling was done. Blood pressure, anthropometry, physical activity, and health-related lifestyle factors were assessed using the standard World Health Organization (WHO) methodology of cardiovascular survey methods and the Global Physical Activity Questionnaire (GPAQ) version 2. The prevalence of HTN, obesity, inadequate physical activity, and other demographic and clinical correlates like antipsychotic use, duration of illness, and family history of non-communicable diseases (NCDs) were studied.
Results
The prevalence of HTN is 20.50%, and it increases with age. SGAs with the use of a single agent are the most common. In total, 45.50% of persons with schizophrenia have a positive family history of a NCD; 22.00% and 07.50% are current tobacco and alcohol users, respectively; and 70% have abdominal obesity, and 54% have generalized obesity. Waist circumference, obesity, and family history of NCDs are significant correlates of HTN. A family history of NCDs is the most significant predictor.
Conclusion
The prevalence of HTN is lower than that of the general population despite the high prevalence of SGA use, obesity, and inadequate physical activity.
Keywords
Introduction
Schizophrenia is a chronic, disabling, lifelong disorder. Schizophrenia has been described as a “life-shortening disease.” A person with schizophrenia has an increased standardized mortality ratio than the general population. In addition to this, an important finding in the epidemiology of schizophrenia in the last 2–3 decades is that persons suffering from it are dying much earlier than they were 3–4 decades ago. This is reflected in the recent increase in the standardized mortality ratio, which is attributed to newer second-generation antipsychotics (SGAs). 1 The comorbidity of schizophrenia with physical illness has become one of the major issues in the last two decades and accounts for 60% of premature deaths not related to suicide. There is evidence from population-based data that this is mainly due to increased cardiovascular cases,2, 3, 4–7 related proximate risk factors, that is, diabetes mellitus (DM), dyslipidemia, metabolic syndrome, obesity, and distant risk factors, that is, health-related poor lifestyle (substance use, unhealthy dietary pattern, and decreased physical activity) and anthropometric physical factors (increased body mass index (BMI)).8–10
In general, hypertension (HTN) is also one of the well-established proximate risk factors for cardiovascular morbidity and mortality, like other factors. There is mixed evidence for the prevalence of HTN in people with schizophrenia. Studies done before the introduction and wide use of SGAs found that HTN prevalence is low in comparison with the general population5, 11, 12, 13 as well as compared to persons with mood and anxiety disorders. 14 A possible reason for this could be the central anticholinergic activity of antipsychotic drugs. Newer studies done after the introduction of SGAs have found HTN to be more prevalent among inpatients with schizophrenia than the general population in Taiwan, and HTN was significantly associated with a higher BMI. 15 HTN without any other cardiometabolic comorbidity is found to have more accelerated cardiac effects than the age-matched general population. 16 The prevalence of cardiovascular diseases and their risk factors has increased worldwide, and similarly for persons with schizophrenia. In a person with schizophrenia, SGAs have furthermore increased the metabolic risk factors. Distant cardiometabolic risk factors like health-related lifestyle behavior have always been poor in persons with schizophrenia. These health-related factors have further deteriorated in the general population, and they might be further worsened in persons with schizophrenia as well.4–10
There is evidence that the prevalence of HTN in persons with schizophrenia might be increasing compared to the pre-SGA era.1, 15 This might be due to metabolic risk mediated by an increased body mass index due to these SGA medications and health-related lifestyle factors. Therefore, we aimed to study the prevalence of HTN, biophysical parameters, and health-related lifestyle behaviors (physical activity and substance use) in persons with schizophrenia attending outpatient services, with our hypothesis being that the prevalence of HTN will be higher than that of the general population.
Methods
This cross-sectional study was carried out in the outpatient services of a tertiary care hospital in north India. A total of 200 patients with schizophrenia on stable antipsychotic prescription (no change in antipsychotic drug or dose) for at least the past 6 months were assessed. The sample size was chosen based upon previous clinical studies on metabolic risk factors in people with schizophrenia in clinical settings. Patients with schizophrenia were both men and women aged 18–75 years. Patients with intellectual disability, organic brain syndrome, substance intoxication and/or withdrawal, and acute febrile illness in the last 2 weeks were excluded. A written informed consent was obtained from all participants who fulfilled the selection criteria. Socio-demographic and clinical profiles, including substance use/abuse, were obtained from patients and their caregivers, along with available medical records. Assessment of biophysical parameters was done as per the guidelines of Cardiovascular Survey Methods of WHO 3rd Edition. 17 Blood pressure (BP) measurement was done by an automated sphygmomanometer, and anthropometric parameters, such as height, weight, waist circumference, and BMI, were assessed as per Cardiovascular Survey Methods of WHO, 3rd Edition. Physical activity was assessed by the Global Physical Activity Questionnaire (GPAQ) version 2, 18 which will be applied by the researcher as per the document developed by World Health Organization (WHO). Information from the patient’s caregiver was also included while administering this questionnaire, wherever required. The scores were entered and calculated as per the analysis guidelines of the GPAQ questionnaire. The scoring of the GPAQ was done for various scores on the Likert scale, which were converted to weighted domain scores for comparison. Also, an overall score was generated as a continuous variable, and a category of adequate vs. inadequate level of physical activity was also created based on the WHO cut-off to yield categorical variables. Similarly, both categorical and continuous variable data were generated for anthropometric measures and BP assessments. Statistical package for social sciences (SPSS) version 28 was used for analysis. For descriptive analysis, categorical variables were expressed as frequency (%) and continuous variables were expressed as mean ± standard deviation (SD). Categorical variables were compared using the Chi-square test or its variation of the Fisher’s exact test and Yates correction, whichever was applicable. Normally distributed continuous variables were compared using independent t-tests or otherwise nonparametric tests like the Mann-Whitney U test. Correlations between various socio-demographic, clinical, anthropometric parameters, and health-related lifestyle variables (substance use and physical activity) were carried out with the presence/absence of HTN (a categorical variable) using point biserial correlation for continuous variables and Pearson Chi-square for categorical variables. Regression analysis was done to find predictors of HTN using binomial logistic regression. For statistical analysis, the level of significance was fixed at 0.05. This study was approved by the Ethics Committee of the institute.
Results
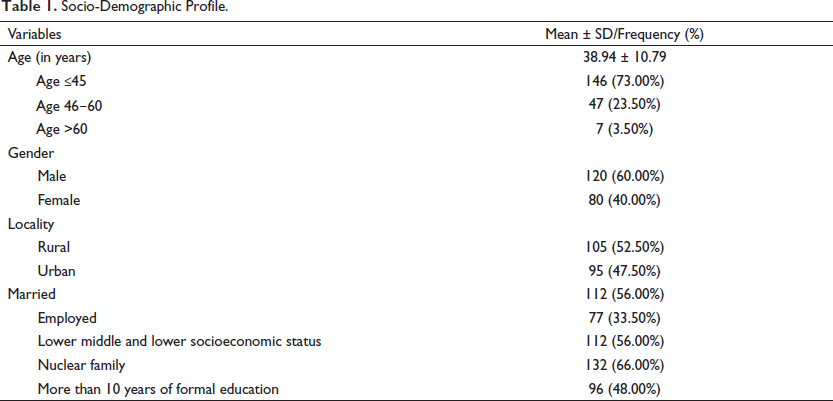
Socio-Demographic Profile.
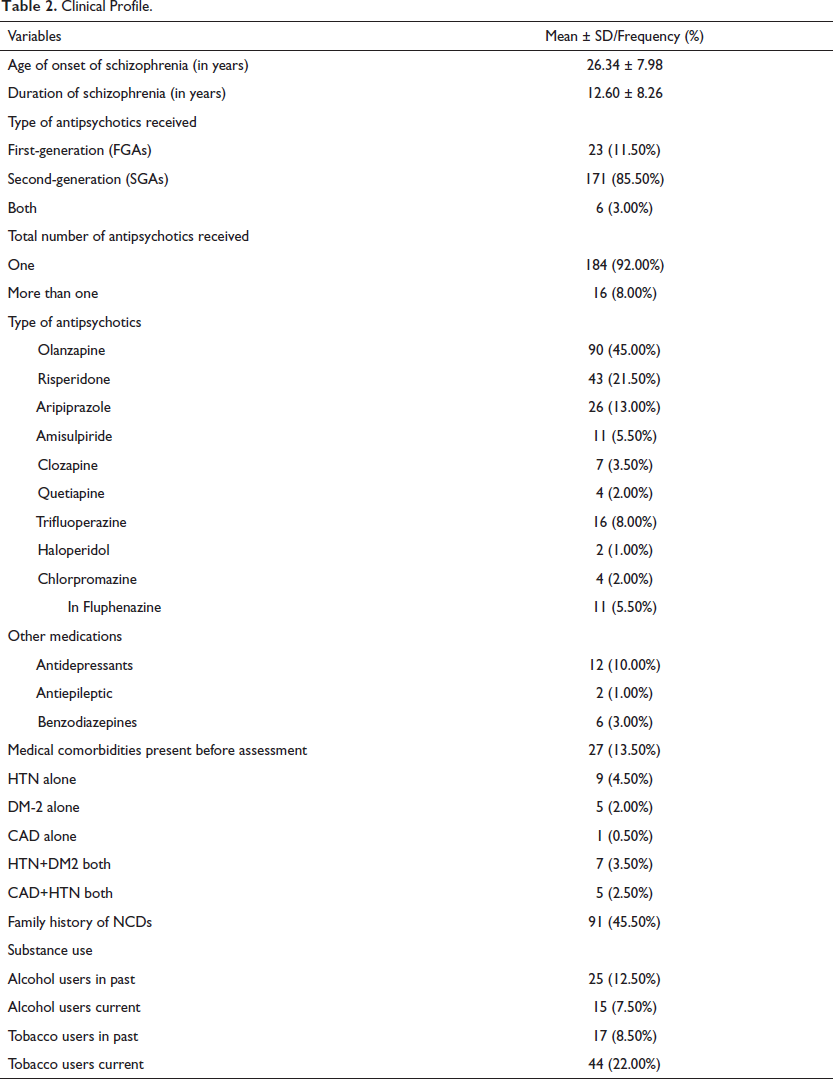
Clinical Profile.
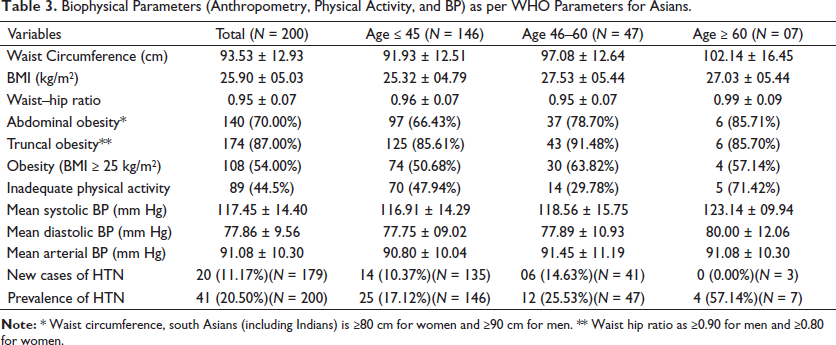
Biophysical Parameters (Anthropometry, Physical Activity, and BP) as per WHO Parameters for Asians.
Prevalence and Correlates of HTN in the Study Population.
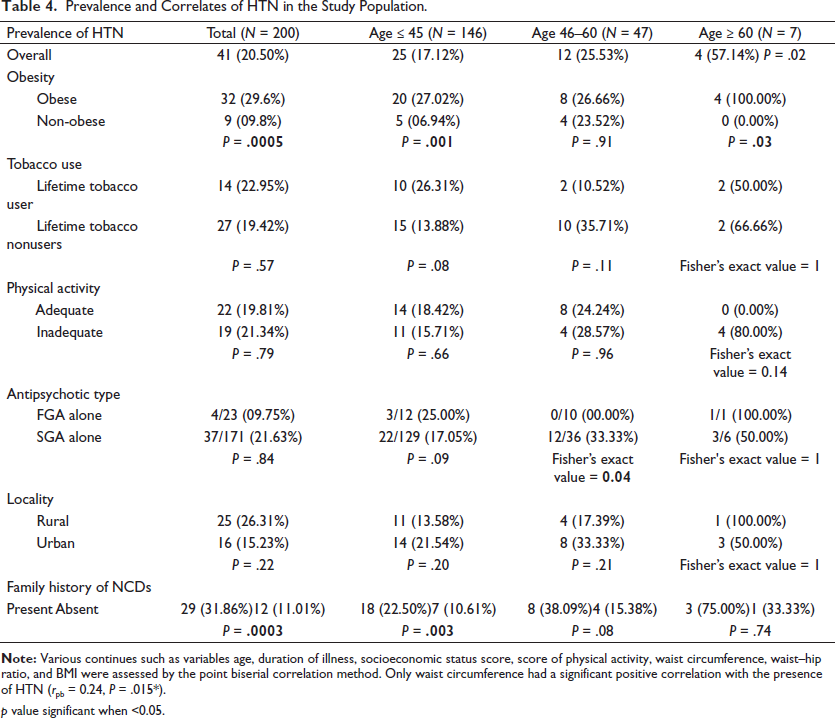
p value significant when <0.05.
Discussion
This study aimed to study the prevalence of HTN and lifestyle factors related to it in clinically stable outpatients with schizophrenia. The inclusion of clinically stable patients in our study removes the confounding factor of the severity of illness from outcome parameters like physical activity level, which might be affected by illness severity. Outpatients in our study are more representative of persons with schizophrenia living in the community compared to inpatients, who have generally more medical comorbidities. The mean age of patients is 38.94 years, which is comparable to other studies and reviews that have studied HTN and its risk factors in patients with severe mental illness (SMI) like schizophrenia and bipolar disorder.19–22
The antipsychotic prescription pattern of our study has more olanzapine (45%) than risperidone (21.50%), which is the reverse of the Indian trend of antipsychotic prescription patterns.23–25 FGA prescriptions are half (11.25%) as common as in other Indian studies (25.15%). Polypharmacy is present in 8% of our sample, compared to 22.36% in other Indian studies.23–25
A standard WHO methodology was used for assessment. In our study, we defined HTN as per JNC VII guidelines as systolic blood pressure (SBP) equal to or more than 140 mm Hg and/or diastolic blood pressure (DBP) equal to or more than 90 mm Hg. The newly diagnosed cases were 11.17% and here also, males have a statistically significant higher incidence than females. This is a very important finding because poor screening and detection are common even in a tertiary care teaching hospital where a psychiatrist is supposed to be more sensitive to screening physical illness. The total prevalence (new + old cases) of HTN was found to be 20.50%. The possible reason for this has already been described above.
The prevalence of HTN in our study population (20.50%), that is, patients with schizophrenia, is lower than in the general population in older studies from the FGA era. From the various studies done in the general population, the range of HTN is 20–40%. Lower prevalence is found in rural populations. The overall prevalence of HTN in India is 29.8%. 26 Approximately 33% of urban and 25% of rural Indians are hypertensive, while in Punjab and Haryana, it is even higher in the range of 40%. 27 The global burden of HTN worldwide is estimated to be 34% in males and 32% in females in the adult population in recently pooled data. 28 In this study, males (21.66%) had a slightly higher prevalence of HTN than females (18.75%), but this was not statistically significant. The prevalence of HTN increases from younger to older age groups in our study, which is like the trend in the general population, but this is less than that of the general population in the region.29, 30
Among the various correlates of HTN, such as abdominal obesity (70%), truncal obesity (87%), and overall obesity (54%)—all are very highly prevalent in our study sample. This increases as age increases and is more common in females. Still, all these prevalences are lower than those of the general population of the geographical region.29, 30 Inadequate physical activity (44.50%) was very much prevalent and was much higher than that of the general population of the geographical region.29, 30 Current smokers (22.50%) were higher, and current alcohol users (07.50%) were like the general population trend of the geographical region. An increase in waist circumference, waist–hip ratio, BMI and the resultant abdominal obesity, truncal obesity, and overall obesity can be explained by significantly more use of SGAs and a sedentary lifestyle reflected by a high percentage of inadequate physical activity due to schizophrenia-related symptoms. This is true even though our sample has relatively good demographic features like employment, married families, and educated individuals with employment in a significant number of patients.
This becomes interesting when we consider the correlates and predictors of HTN. Here, the family history of non-communicable physical illness, which is present in 45.50% of the study sample, emerges as the most significant predictor. Increased waist circumference, obesity, and duration of illness are others, but their contributions are minimal in comparison to a family history of NCDs. Our study sample has a very high use of olanzapine, which causes maximum weight gain after clozapine. Along with inadequate physical activity, SGAs might have led to a very high prevalence of obesity in the general population. But this has not translated into the high prevalence of HTN in our sample, despite very high rates of family history of NCDs. Rather prevalence of HTN is still lower than that of the general population representing the geographical region. This implies that factors other than those studied might be responsible for the finding of a lower prevalence of HTN in our sample. This is reflected in our logistic regression analysis because factors in our sample could account for low variance. Our findings on the prevalence of HTN are lower than those of a study done in Taiwan, 15 which had mostly inpatients who were more severely ill. But obesity and SGA use are similar to the findings of the Taiwan study. The strength of our study is the standardized assessment of BP and other biophysical parameters along with physical activity level in accordance with WHO and JNC III guidelines. The limitations of our study include a small sample size limited to outpatients from a clinical setting only. Only a limited number of correlates of HTN are studied. In spite of high metabolic risk and a poor lifestyle, there is a low prevalence of HTN in our study sample. Future studies with a well-designed methodology are needed to reexamine this finding with samples from large clinical outpatients, inpatients, and community-living patients. A standardized assessment of risk/protective factors related to HTN in these various samples must be examined separately and in combination for better understanding. This has implications for physical health monitoring and the prevention of adverse cardiac events in patients with schizophrenia.
Conclusion
The prevalence of HTN in stable outpatients of schizophrenia is less than that of the general population of the same geographic area, despite very high SGA use. Antipsychotic use and inadequate physical activity have resulted in an increased waist circumference and obesity. Despite being a correlate of HTN diagnosis, these have not resulted in a higher prevalence of HTN. This implies that there might still be some unknown factors and interactions among various factors resulting in a lower prevalence of HTN than in older studies from the FGA era.
Footnotes
Abbreviations
BMI: Body mass index
BP: Blood pressure
CAD: Coronary artery disease
DBP: Diastolic blood pressure
DM: Diabetes mellitus
FGA: First-generation antipsychotic
GPAQ: Global Physical Activity Questionnaire
HTN: Hypertension
JNC: Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
SBP: Systolic blood pressure
SGA: Second-generation antipsychotic
NCD: Non-communicable disease
SPSS: Statistical package for social sciences
WHO: World Health Organization
Acknowledgement
Akhilesh Sharma and Devender Singh Basera have contributed equally and should be considered co-first authors.
Authors’ Contribution
AS was involved in conceptualizing and designing the study, review of clinical studies and literature, analysis and interpretation of data, and preparation and editing of manuscript.
DSB was involved in conceptualizing and designing the study, review of clinical studies and literature, acquisition and interpretation of data, and preparation of manuscript.
VS was involved in conceptualizing and designing the study, interpretation of data, and preparation and editing of manuscript.
SMS was involved in conceptualizing and designing the study, review of clinical studies and literature, interpretation of data, and preparation and editing of manuscript.
The manuscript complies with ICMJE guidelines.
Statement of Ethics
This study was approved by IEC (Institutional Ethical Committee). All the participants were informed about the study and were involved after giving written informed consent.
This study protocol had been approved by the Institutional Ethics Committee of the Postgraduate Institute of Medical Education and Research, Chandigarh, vide Reference Number NK/4256/MD/3188-89.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.