
Abstract
Background:
Indian Diabetes Risk Score (IDRS) is a screening tool for quantifying the risk of diabetes mellitus (DM) development in the Indian population. The present study has evaluated the level of risk of developing DM in Chandigarh and Panchkula based on the IDRS score.
Methods:
As a part of a national diabetes control trial funded by the Ministry of Health and Family Welfare (MoHFW) and the Ministry of AYUSH, Government of India, 1,916 participants from the Chandigarh and Panchkula regions were assessed for the risk of developing DM. Risk assessment was done on the basis of the IDRS score which includes age, family history, waist circumference, and physical activity as its contributing factors. Participants with an IDRS score <30 were in the low-risk category, those with 30 to 50 were in the moderate-risk category, and those with >60 were in the high-risk category for DM.
Results:
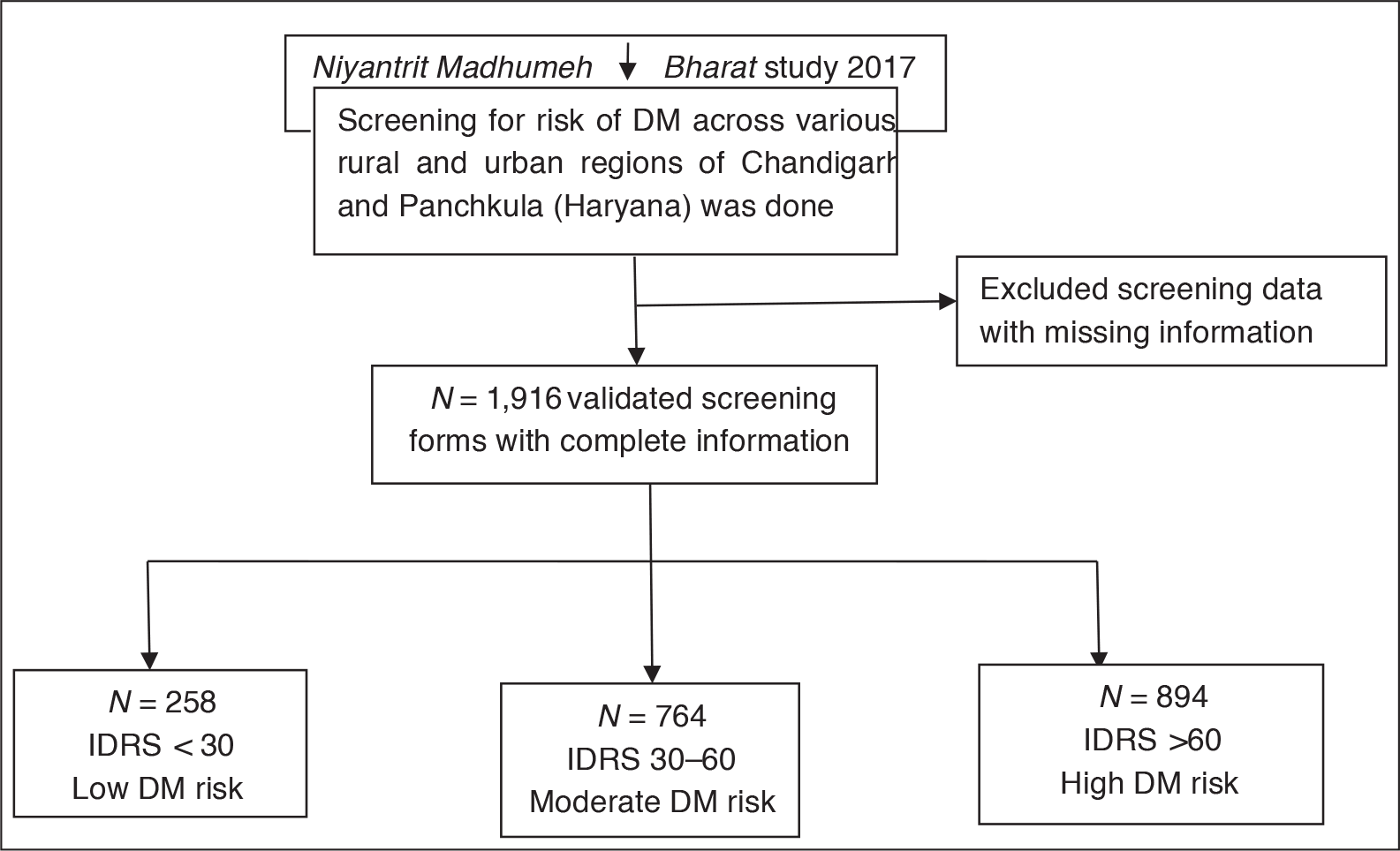
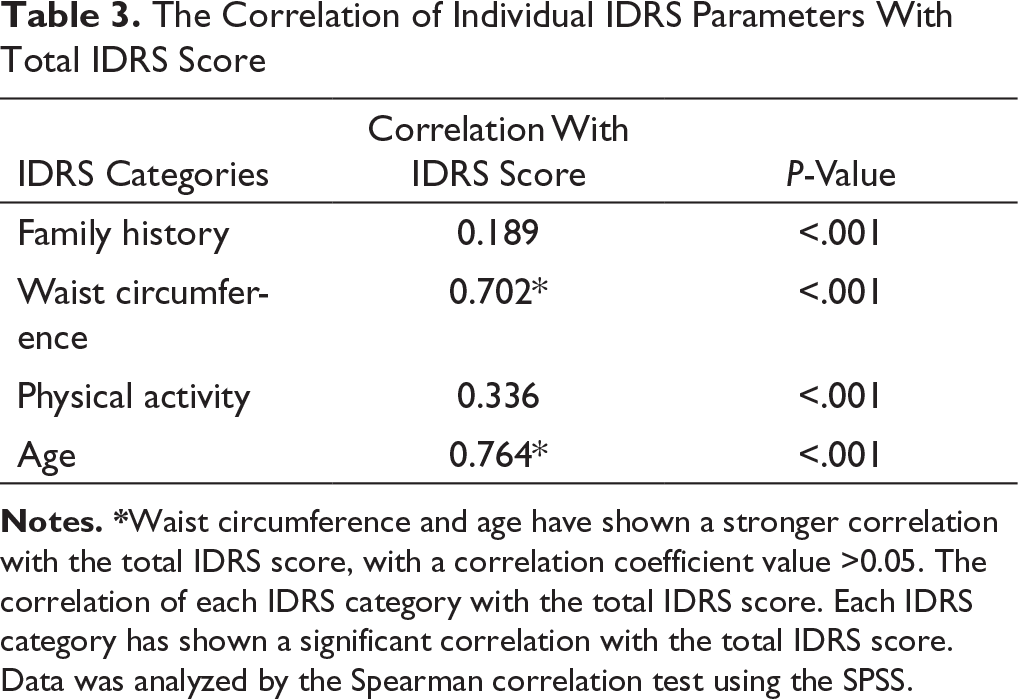
Out of the 1,916 screened respondents (59.86% females and 40.14% males), 894 participants (46.65%) were at a high risk for DM (IDRS >60), 764 (39.87%) were at a moderate risk (IDRS = 30–60), and 258 (13.46%) were at a low risk (IDRS <30). Waist circumference contributed to 35.90% of the high-risk category followed by age (19.67%) and physical activity (11.67%). Age and waist circumference also showed a strong correlation with the total IDRS score.
Conclusion:
The Chandigarh and Panchkula population showed a high tendency to develop DM based on the IDRS score. Modifiable risk factors such as waist circumference and physical activity were the major contributing factors. Apart from the modifiable risk factors, age was also another major contributing risk factor. Based on these outcomes, lifestyle modifications like yoga and exercise can be proposed for this population as a preventive approach to reduce the risk of developing DM and other associated cerebrovascular complications.
Introduction
Diabetes mellitus (DM) is a metabolic disorder that is prevalent in the middle-aged and elderly population. 1 The population with DM has reached alarming proportions in India with 2.4% in rural and 11.6% in urban areas. 2 Lifestyle and stress are some of the major causes of DM, 3 and these could also lead to the development of major neurological disorders. DM is also associated with complications like hypertension, dyslipidemia, and obesity, which can lead to microvascular and macrovascular complications resulting in strokes, coronary artery disease, renal failure, retinopathies, and depression.4, 5 DM is also strongly correlated with dementia, vascular dementia, and Alzheimer’s disease,6, 7 and also diabetic retinopathy which most commonly leads to blindness in adults. 8 DM and complications related to it also majorly impacts quality of life. 9
A lack of effective screening methods for DM risk complicates the scenario. An early identification of the risk of development of DM may help in reducing the prevalence of DM by creating awareness. To ease this situation, Indian Diabetes Risk Score (IDRS) has been developed as an effective screening tool to detect the risk. 10 IDRS was developed as a screening tool by the Madras Diabetes Research Foundation and validated in a Chennai Urban Rural Epidemiology Study (CURES) study in 2005 by Mohan et al. 11 Based on the IDRS score, participants can be categorized into low, moderate, and high risks of developing DM. Numerous studies have shown high sensitivity and specificity of IDRS to diagnose undetected DM.12–14. If physicians can predict the risk of DM based on simple scales like IDRS with high sensitivity and specificity, this will not only help in the prevention of DM, but also in the prevention of above-stated complications related to DM.
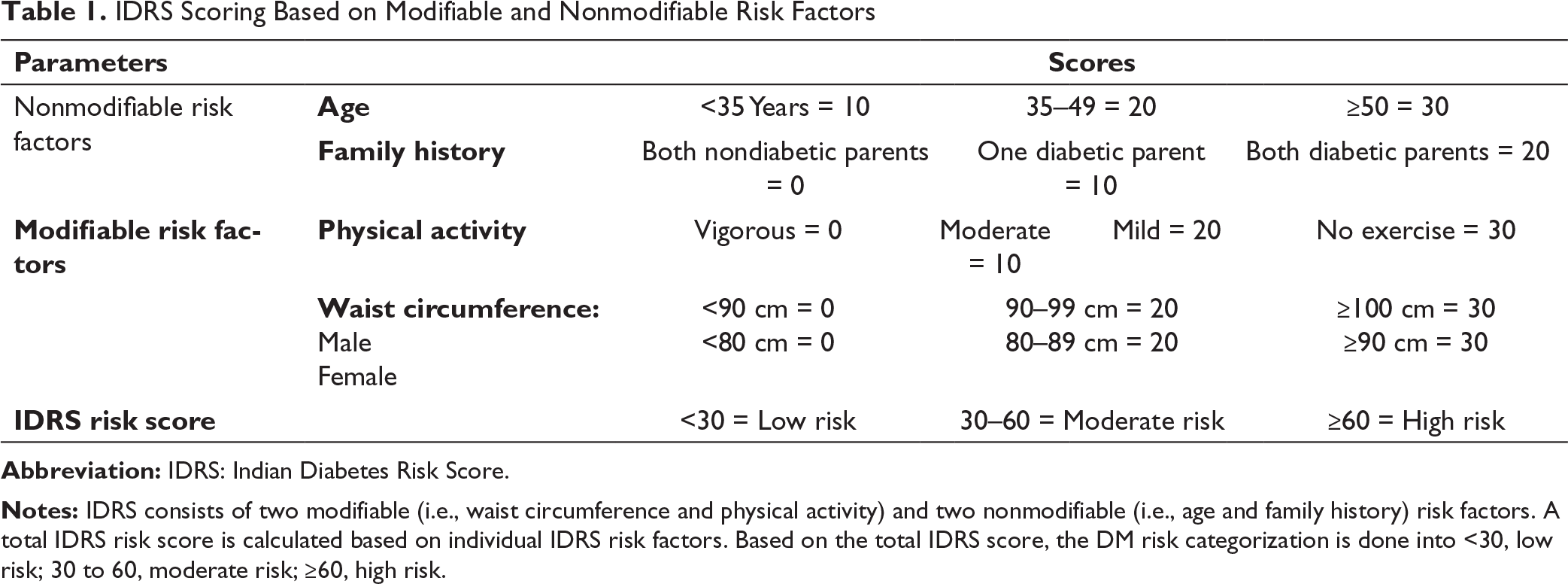
The IDRS score is calculated based on two modifiable (physical activity and waist circumference) and two nonmodifiable risk factors (family history and age). Modifiable risk factors such as waist circumference and physical activity have been linked to DM occurrence time and again. 1 These can be moderated with lifestyle management activities like yoga and exercise that can provide some benefits by decreasing the contribution of the modifiable contributing factors and may thus decrease the overall IDRS score, which eventually decreases the risk of DM along with other associated comorbidities.
We have been previously working on biomarker discovery and genetic screening for neurological diseases such as amyotrophic lateral sclerosis,15–18 age-related macular degeneration,19–22 and Parkinson’s disease, 23 developed various animal models for retinal degeneration and memory loss,24–26 and studied the efficacy of umbilical cord blood-derived stem cells in rescuing retinal degeneration and memory loss.26–28 Now we have shifted toward the public health sector, and through this study we wanted to identify the proportion of population of Chandigarh and Panchkula under the risk of DM development based on the IDRS scoring. We also wanted to identify the most contributing IDRS factor in the high-risk category.
Methodology
Study Settings and Design
As a part of a national study (Niyantrit Madhumeh Bharat 2017), 11 a door-to-door screening across various regions of Panchkula (Haryana) and Chandigarh was done. Information about the IDRS parameters was collected. Along with IDRS parameters, information about habitat, gender, and age was also collected.
Schematic Representing the Study Participant Distribution on the basis of IDRS Score.
Sample Size and Sampling
Various rural and urban areas of Chandigarh and Panchkula were selected for this study. Based on inclusion and exclusion criteria, participants were screened for DM risk using the IDRS score.
Data Collection
Data was collected in a questionnaire-based screening form, and the details of the participants such as name, age, gender, and habitat were collected and noted in the forms. Information about IDRS parameters such as age, physical activity, and family history of diabetes was obtained from the participants, and waist circumference (another parameter of the IDRS score) was measured using a measuring tape and was recorded in centimeters.
IDRS and Its Parameters
IDRS Scoring Based on Modifiable and Nonmodifiable Risk Factors
Data Analysis
Statistical analysis was done by using IBM SPSS 22. The numbers of participants falling in different categories were reported by using descriptive statistics. A chi-square test was done to compare the risk factors within each IDRS risk category. A one-sample Kolmogorov Smirnov (KS) test was used to check the normality of the data. Correlation between the IDRS factors was done using Spearman’s Rho correlation. Values <0.05 were statistically significant.
Results
Number of Participants in Each IDRS Risk Factor Category
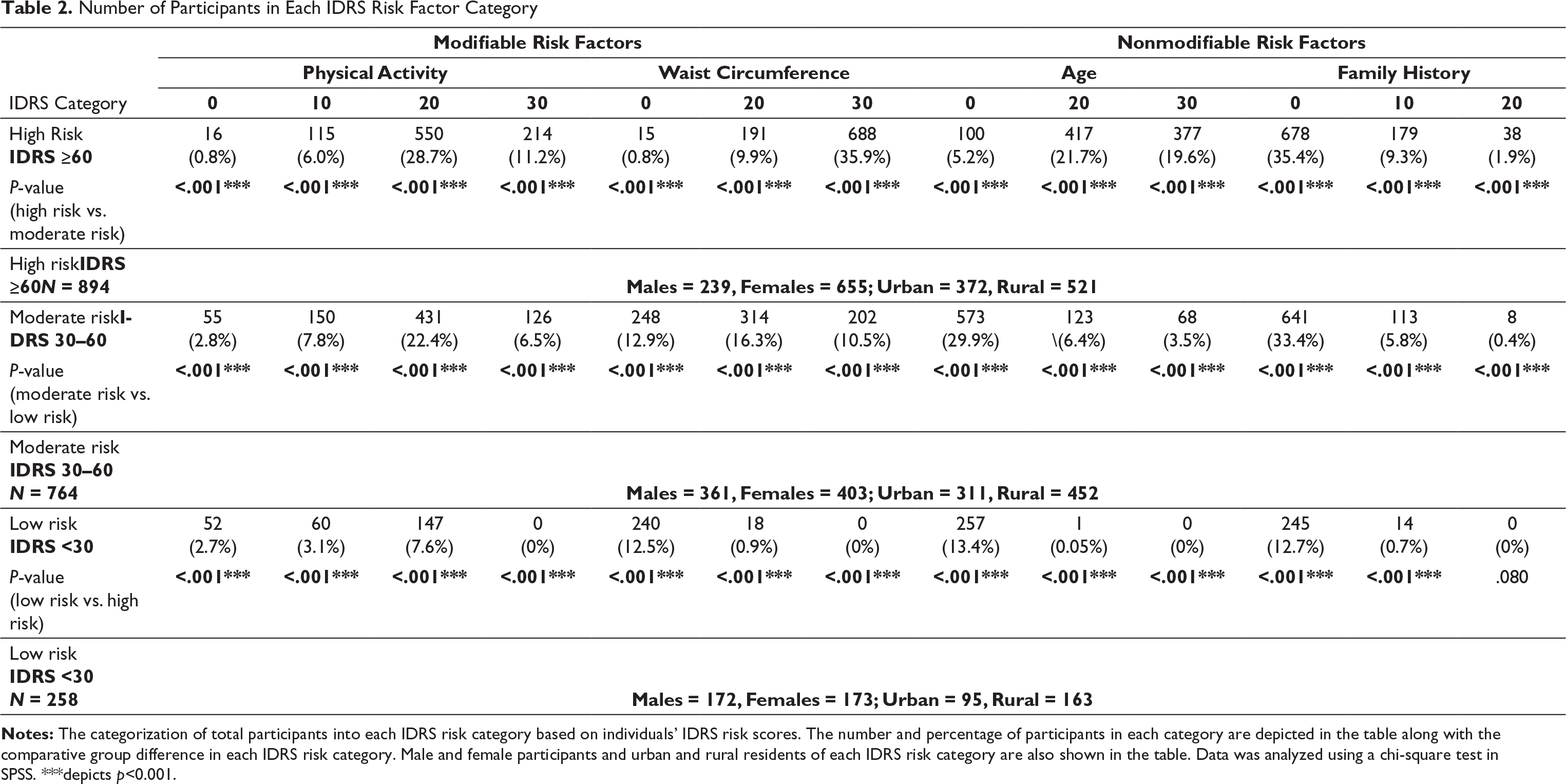
difference in each IDRS risk category. Male and female participants and urban and rural residents of each IDRS risk category are also shown in the table. Data was analyzed using a chi-square test in SPSS. ***depicts p<0.001.
Distribution of Total Population Based on Modifiable and Nonmodifiable Risk Factors of IDRS
In the high-risk category, waist circumference contributed to 35.9%, whereas age contributed to 19.7%. No or low physical activity contributed to 11.1% and 28.7% in the high-risk category, respectively.
Overall, modifiable risk factors such as waist circumference and low physical activity contributed to 46.65% of high IDRS score, and nonmodifiable risk factors contributed to 21.7% of high IDRS score (Table 2).
IDRS Distribution Based on Gender and Habitat
Based on gender, females were more prone to DM with 34.2% in the high-risk category as compared to 12.5% males. In the moderate-risk category also, more females were there (21%) in comparison to 18.9% males. In case of the low-risk category, the numbers of both male (8.9%) and female (9%) participants were almost similar.
Based on habitat in the high-risk IDRS category, more participants were from the rural areas (27.2%) in comparison to urban areas (19.4%). The moderate-risk group also had more participants from rural areas (23.6%) in comparison to 16.2% from urban areas. In the low-risk category, 8.5% were from rural areas and 4.9% were from urban areas (Table 2).
Correlation of Each IDRS Category With Total IDRS Score
The Correlation of Individual IDRS Parameters With Total IDRS Score
Discussion
In the present study, IDRS was used as a screening tool to assess the risk of type 2 diabetes mellitus (T2DM) development in the population of Chandigarh and Panchkula. A high proportion of the recruited population (46.6%) were found to be at a high risk of DM. Major contributing factors in the high-risk category were modifiable risk factors with waist circumference contributing to 35.9%, and no or low physical activity contributing to 11.2% and 28.7%.
IDRS is a successfully used parameter to assess the individual’s risk to T2DM in the Indian population. It has been proved by various studies on the Indian population that a high IDRS score is directly correlated to the development of diabetes or prediabetes.29, 2 A high proportion of the population under the modifiable risk category would signify a higher prevalence of sedentary lifestyle in the population. In our population, a high contribution of modifiable risk factors in the high-risk category shows the need of lifestyle management practices for this group of population. It was found that approximately half of the participants (46.6%) were at a high risk of DM based on their IDRS score. Waist circumference (measure of obesity) contributed highest to this high-risk category, with 35.90% of the participants having a waist circumference ≥100 cm in case of males and ≥90 cm in case of females. Obesity is indeed associated with DM development, 30 and abdominal (visceral fat) obesity indicated by a high waist circumference is a known indicative factor for cardiometabolic diseases. 31 Abdominal obesity also affects the brain structure through neurodegenerative or vascular processes and can thus lead to cognitive decline and dementia.32, 33
A high proportion of the Chandigarh population in the high waist circumference category have shown a higher tendency of developing cardiometabolic disorders. We also observed that the physical activity pattern was also a reason for the high proportion of the population being at a high risk, out of which 11.2% were performing no physical activity and 28.7% were mildly physically active. Low physical activity, which is another parameter of sedentariness, has previously been linked to the increase in the incidence of DM 34 and also neurodegenerative diseases 18 as it increases the oxidative stress. As in our population we have found waist circumference and physical activity as the major contributors in the high-risk population, this shows that a large proportion of this population are prone to sedentariness, which puts them at a high risk of developing DM and this could also further lead to the development of cardiometabolic disease and neurodegenerative diseases.
Our data is consistent with the previous studies which have shown a high prevalence of T2DM and prediabetes in the Chandigarh population.35, 36 The Chandigarh population has shown a higher acceptance about the role of yoga in the DM management. 37 Hence, this data not only highlights the high risk of this population of developing DM, but also highlights the need of lifestyle management through practices such as yoga and exercise, which may act through alteration in the molecular patterns and thus protect from development of lifestyle disorders like DM. 38 Yoga may also help in improving lifestyle by reducing stress and anxiety, which are a common part of today’s lifestyle and the cause of many metabolic disorders such as DM, hypertension, etc. 39 The modifying risk factors (i.e., waist circumference and physical activity) are strongly responsible for a high DM risk in this population. Modifying these factors through lifestyle management activities not only reduces the risk of DM, but also can prevent various cardio vascular diseases (CVDs) and neurological disorders.
Conclusion
This study shows that the population of Chandigarh and Panchkula is at a high risk of developing DM. Apart from age, low physical activity and waist circumference are the major contributors. This indicates that screening programs like this can be cost-effective doable measures at the grassroots level before a referral for the mainstream health care. This study also highlights the importance of incorporating physical activities like yoga to reduce the risk of DM through modulating the risk parameters of DM.
Footnotes
Acknowledgments
The authors acknowledge the support of the Indian Yoga Association for manpower, Ministry of Health and Family Welfare, and Ministry of AYUSH for bearing the overall cost of the project.
Authors Contribution
Declaration of Conflicting Interests
Ethical Statement
Informed consent was obtained from all the volunteers who participated in the study.
Funding
This research work was supported by the Ministry of AYUSH, Government of India (grant number: 16-63/2016-17/ CCRYN/RES/Y&D/MCT/ dated 15.12.2016).