
Abstract
Background
Postural instability is a common problem in patients with Parkinson’s disease (PD). The appropriate cooperation of vestibular, visual, and proprioceptive signals along with apt anticipatory and adaptive postural responses is essential for postural stability. Abnormalities in this sensorimotor admixture lead to postural instability in PD. The function of vestibular otolith function and its central connections in postural instability of PD is still obscure. Cervical vestibular-evoked myogenic potentials (VEMP) can be used to assess the function of the saccular part of otolith and its connections.
Purpose
We aimed to study the role of dysfunction of the saccule and its connections at the brainstem by comparing the VEMP with normal controls and correlating it with the postural instability in patients with PD.
Methods
Thirty patients with PD and 30 healthy volunteers were included in the study, after obtaining the institutional ethical committee approval. Patient’s demographic data, stage and duration of illness, treatment history, history of fall, postural instability, Unified Parkinson’s Disease Rating Scale (UPDRS) score, and Non-Motor Symptoms Scales (NMSs) were noted. Cervical VEMP analysis was done for both patients and controls.
Results and Conclusion
Patients with absent VEMP had significant postural instability, a history of falls, and a high UPDRS score. Mean P13 and N23 latencies were prolonged, and the amplitude was significantly low in patients with PD. Absent cVEMP was significantly associated with postural instability, non-motor symptoms, especially gastrointestinal, miscellaneous symptoms, and mood/cognition. VEMP can be considered an early electrophysiological marker for dysfunction of otolith and its central connections.
Introduction
The incidence of Parkinson’s disease (PD) increases as age increases, and age is an important risk factor for it. The incidence of PD in females above 40 years was 37.55 per 100,000 person-years and 61.21 in males above 40 years. 1 The disease is disabling with many motor manifestations like postural instability, tremors, dysequilibrium, freezing gait, and the substantial falls. Prospective studies have found that 18% to 65% reported recurrent falls, and 35% to 90% of patients reported at least one fall per year. 2 Freezing of gait, impaired anticipatory and reactive balance, and impaired orientation are associated with falls in PD. 3 There is a drop in survival after the first fall in PD to that of atypical Parkinson’s syndromes. 4 Multisensory inputs, such as somatosensory, visual, and vestibular sensations, operate on different levels of the brain, allowing for flexible posture-gait control. 5 The appropriate cooperation of vestibular, visual, and proprioceptive signals along with apt anticipatory and adaptive postural responses are essential for postural stability. Abnormalities in this sensorimotor admixture lead to postural instability in PD. The function of vestibular otolith function and its central connections in postural instability of PD is still obscure. Cervical vestibular-evoked myogenic potentials (VEMP) can be used to assess the function of the saccular part of the otolith. In this study, we intended to study the role of dysfunction of the saccule and its connections at the brainstem by comparing the VEMP with normal controls and correlating it with the postural instability in patients with PD.
Methods
This cross-sectional case-control study was conducted at the Neurology department, a tertiary care center in South India. The sample size of 31 was obtained with a 2% prevalence of PD, a confidence interval of 95%, and a 5% margin of error. 6 After obtaining the institutional ethical committee approval (ECR/270/Inst./20022014), Thirty patients with idiopathic PD and 30 healthy volunteers were included in the study. Patients with Parkinson’s plus syndrome, conductive hearing loss, tinnitus, and patients on labyrinthine sedatives were excluded from the study. Informed written consent was obtained from all the participants before the study. The patients’ demographic data, clinical history, including duration of illness, modified Hoehn and Yahr staging and Unified Parkinson’s Disease Rating Scale (UPDRS), history of fall, and pull test for postural instability were noted. Non-motor symptoms (NMS) were noted as per the NMS scale. 7
VEMP Recording
Subjects were examined in the recumbent position. Active electrode, reference electrode, and ground electrodes were placed over the middle of the sternocleidomastoid (SCM), medial end of the clavicle, and over the sternum, respectively. The subjects were asked to lift their head against gravity to activate the SCM. A surface electromyogram (EMG) was sampled from 20 ms to 100 ms after the stimulus onset. Unrectified EMG averages were used to measure reflex latencies.
VEMP Stimulus
Brief high-intensity click stimuli were delivered via headphones to each ear, starting at 60-decibel hearing level (dBHL) till 110 dBHL. Analysis was done for 100 ms with a stimulation rate of 3 Hz. Average of 128 stimuli was noted. This method was repeated once to ensure reproducibility by using the Medelec Premiere EMG system. P13 and N23 latencies were measured from stimulus onset to the peak of the initial positivity and the next negativity. Peak-to-peak amplitude was also measured. The latencies and amplitude were measured on the same side of the stimulated ear.
Statistical Analysis
SPSS version 21 (IBM, USA) was used for statistical analysis. Quantitative variables were mentioned as mean and standard deviation. Qualitative variables were mentioned in number and percentage. An unpaired t-test was done for quantitative variables. Chi-square or Fisher exact test was done for qualitative variables. P value <.05 was considered significant.
Results
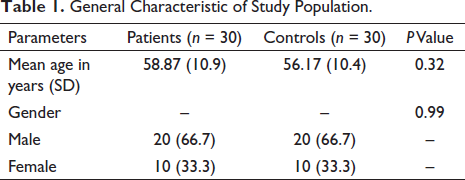
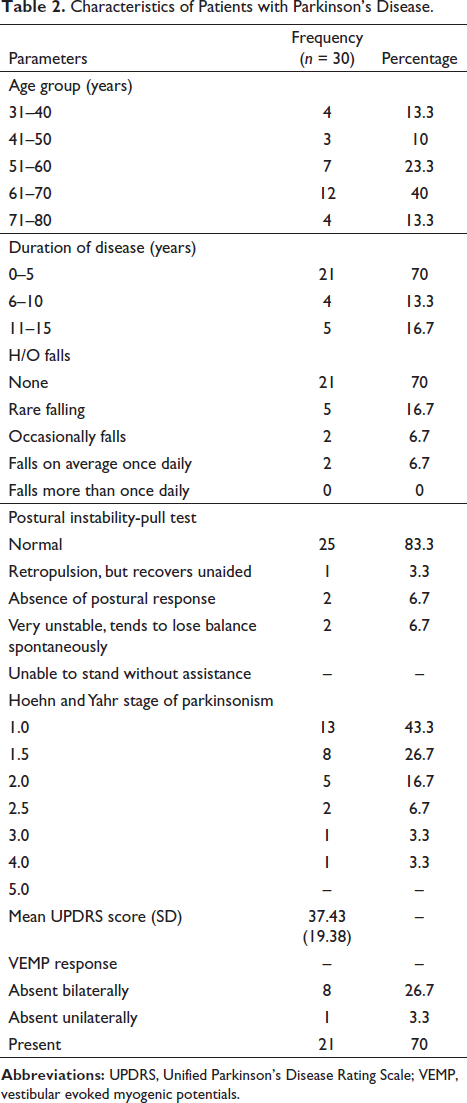
The mean age of patients was 58.87 and the control was 56.17 years, which was comparable. Both groups had 20 male and 10 female participants (Table 1). The maximum number of patients were in the age group of 61 to 70 years, and most of the patients had PD for less than 5 years. Twenty-one patients had no history of falls, and 9 had variable incidences of falls, and 5 had postural instability as diagnosed by pull test. Most of the patients were in Stage 1 of the Hoehn and Yahr stage of PD, followed by stages 1.5, 2, 2.5, 3, and 4. The mean UPDRS score of 37.43. Of 30 patients, 21 patients showed bilateral VEMP response, 8 did not show VEMP response bilaterally, and 1 had a unilateral VEMP response (Table 2).
General Characteristic of Study Population.
Characteristics of Patients with Parkinson’s Disease.
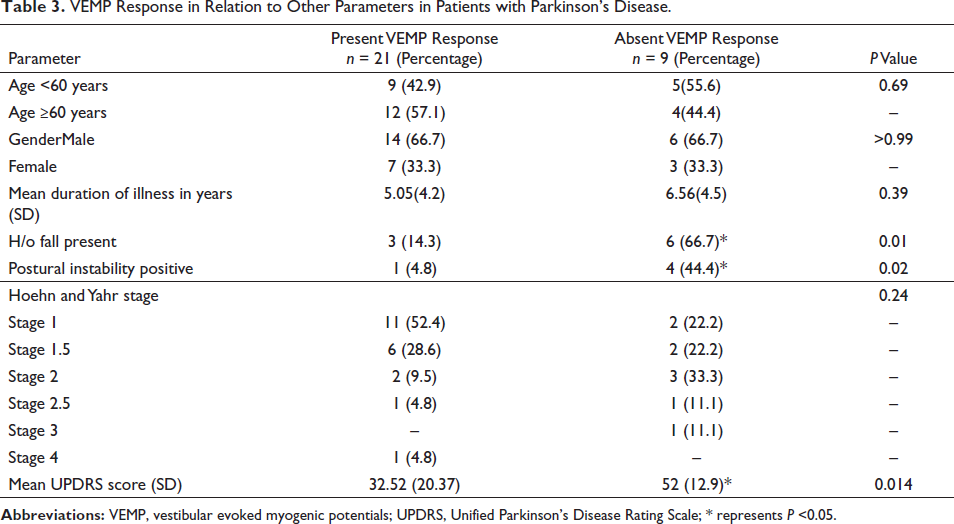
The absence of VEMP response was seen in five of them in the age below 60 years and four above 60 years. The duration of illness though slightly higher in the absent VEMP response group but statistically not significant. The history of falls and postural instability were significantly higher in the absent VEMP response group. The Hoehn and Yahr staging showed no significant difference between the two groups. The mean UPDRS score was significantly greater in the absent VEMP response group (Table 3).
VEMP Response in Relation to Other Parameters in Patients with Parkinson’s Disease.
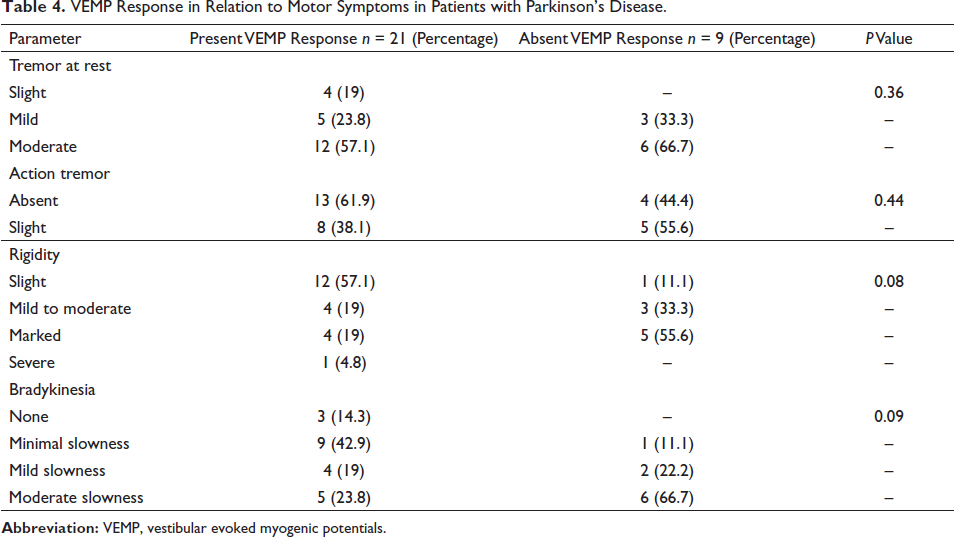
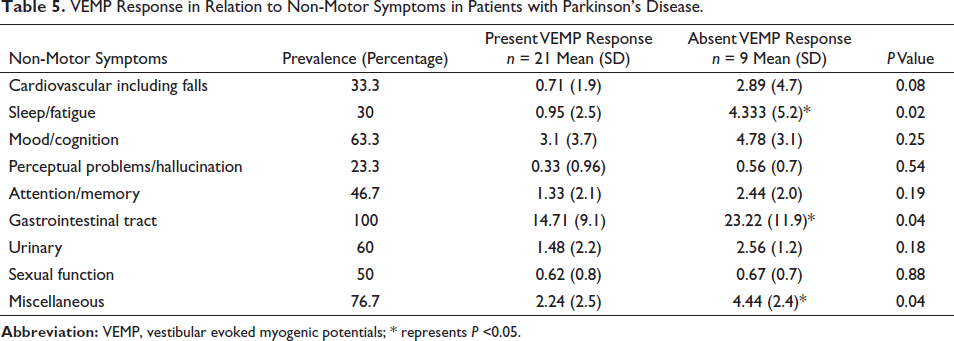
Motor symptoms such as tremor and rigidity were present in all the participants. Bradykinesia was seen in 86% of the study population. These motor symptoms were not significantly associated with VEMP response (Table 4). Gastrointestinal symptoms were the commonest NMS (100%), followed by miscellaneous symptoms such as pain, change in taste/smell/body weight and excessive sweating (76.7), and mood/cognition symptoms (63.3). The NMS, especially sleep/fatigue, gastrointestinal symptoms, and miscellaneous symptoms, were significantly associated with absent VEMP response (Table 5). Comparing the mean P13 latency and N23 latency, the patients with PD had significantly prolonged values. The mean amplitude was significantly reduced in patients with PD (Table 6).
VEMP Response in Relation to Motor Symptoms in Patients with Parkinson’s Disease.
VEMP Response in Relation to Non-Motor Symptoms in Patients with Parkinson’s Disease.
Comparison of P13 and N23 Latencies and Amplitude of VEMP in Patients with Parkinson’s Disease and Controls.

Discussion
The age of participants of both groups was comparable; PD is a disease of the elderly, usually above the age of 60 years, and as age progresses, the risk of PD increases. 8 In our study, the maximum number of patients were in the age group of 61 to 70 years. The duration of disease varied from 0 to 15 years, and most of them had the disease for 5 years. Usually, PD arises at 60 years, and the disease can last 10 to 15 years as the disease progresses, the life expectancy decreases8-10, and men are more affected than women. 11
In our study, 21 patients had no history of falls, 9 had variable incidences of falls, and 5 had postural instability as diagnosed by a pull test. 79% of PD patients have a natural history of falls followed over 54 months. 12 Another study reported 38.6% of falls, and it has been seen hypofunction of cholinergic function. 13 The pedunculopontine nucleus (PPN), which represents thalamic anticholinesterase activity, is the key node for gait control. 13 Around 60.5% of the diseased patients reported at least one fall, and 39% reported recurrent falls. 2 There are many factors associated with falls: (a) a positive fall history, (b) increased disease severity and duration, (c) increased motor impairment, (d) treatment with dopamine agonists, (e) increased levodopa dosage, (f) cognitive impairment, (g) fear of falling, (h) freezing of gait, (i) impaired mobility, and (j) reduced physical activity. There are several tests to assess the probability of falls, but there are reports that instead of a single test prediction, falls in PD benefit from a balance test in addition to a history of falls. 14
The severity of the PD is assessed by motor manifestations, ability to do daily activities, and the response to the treatment. UPDRS and Hoehn and Yahr staging are commonly used to assess the severity of PD. 15 Hoehn and Yahr staging is the most widely used for patients with PD. It involves staging from zero to five of the motor manifestations of PD; combines features of motor impairment, progression, and disability. Hoehn and Yahr staging is ideal, as it depends on examination. 15 UPDRS includes four subscales: the first covers the mentation, behavior, and mood; the second scale rates the activities of daily living; the third scale is a clinical rating of the motor manifestations; and the fourth scale includes complications of therapy. Both these scales are not interval scales; they are basically ranks. 15 In our study, most patients were in Stage 1 of the Hoehn and Yahr stage of PD, followed by the stages 1.5, 2, 2.5, 3, and 4. A study demonstrated that most patients had a Hoehn and Yahr Scale score of Stage 2 or higher. 16 . There was no significant difference in VEMP response among the various Hoehn and Yahr stage of PD in our study, similar to other studies.17, 18 de Natale et al. have observed that VEMP abnormalities increase with the severity of the disease. 19 The mean UPDRS score was significantly high in patients with absent VEMP response, similar to the study by Shalash et al. 20
A postural disturbance in PD is a common finding, often unresponsive to treatment. The vestibulocollic reflex is one of the brainstem pathways involved in postural balance. In our study, out of 30 patients, only 21 bilateral responses were recorded and 1 patient showed a unilateral response. A similar study reported bilateral absent ocular VEMP responses in PD patients with dizziness, but the frequencies of bilateral absent cervical VEMP responses were not different between the dizzy and non-dizzy groups. 21 Interestingly, our study has also shown that absent VEMP response patients had a significantly higher incidence of history of falls and instability. This is similar to a study where 41.7% of patients with PD had altered cervical VEMP. It has been postulated that abnormalities in VEMP may suggest brainstem dysfunctions in PD patients, which are well correlated with postural and REM sleep disorders. 22 . An abnormal VEMP with postural instability is suggestive of a vestibular pathology. 21
The motor and NMS of the PD have been related to the degeneration of several brainstem nuclei. Tremor is the commonest motor symptom in PD. In our study rest tremor was the most common motor symptom in all the participants. Rigidity also was present in all the patients in the current study. Motor symptoms were not significantly correlated with the cVEMP response in the present study. This finding was supported by other similar studies.22-24 In contrast to our study, Shalash et al. found a significant relation between cVEMP and rigidity and bradykinesia but not tremor. 20
NMS are common in the early stage of the PD, and its course varies depending on the treatment and progression of the illness. These symptoms constitute the important early clinical markers of PD also. In a prospective study of PD by Erro et al., 97.8% of the study population had at least one NMS on two years follow-ups. Depression and concentration symptoms improved with dopamine agonists. 25 Tibar et al., stated that all patients had at least one NMS; urinary symptoms were the commonest, followed by sleep disturbances. 26 In our study also, all the patients with PD had at least one NMS. Gastrointestinal symptoms, especially excessive salivation, are the commonest NMS, followed by pain and mood symptoms. NMS, especially sleep/fatigue, gastrointestinal symptoms, and miscellaneous symptoms, were significantly associated with absent VEMP response in the current study. Shalash et al. found that sleep, perception, memory, and urinary symptoms were significantly correlated with cVEMP. 20
In our study, the mean P13 and N23 latencies were significantly prolonged in patients with PD; and the mean amplitude was significantly low. Similar results were observed by Hussein et al. and Shalash et al.; significantly delayed P13 and N23 latencies and smaller P13–N23 amplitude in both ears were seen in patients with PD than controls.20, 27 Contralateral abnormal VEMP correlated with rigidity and bradykinesia. 20 They also demonstrated the correlation of VEMP to the motor and some NMS. A correlation between VEMPs and motor and non-motor features is useful in managing neurodegenerative Parkinson’s syndromes. The amplitude of the VEMP was significantly increased by dopa administration rather than subthalamic stimulation in PD patients; however, they didn’t notice any change in latencies. 18 This prolonged latency is suggestive of decreased excitability of the vestibular nucleus. de Natale et al. observed that VEMP abnormalities increase with the severity of the disease. 19 VEMP can be used as an early biomarker for brainstem involvement. We have not correlated the motor disturbances with VEMP; this would have given important insight into the association.
Conclusion
There was a significant association between VEMP and postural instability. There was a prolonged latency in P13, N23, and reduced amplitude in patients with PD. An extensive examination of motor and electrophysiological investigation like VEMP can give insights into the pathophysiological dynamics of otolith and its connection involvement. Correlation of VEMP with motor and NMS, especially the NMS, will give a better insight into disease progression as NMS, and abnormal VEMP are early signs of PD. Apart from this, VEMP can be considered an early electrophysiological marker for dysfunction of otolith and its central connections.
Footnotes
Authors’ Contribution
Conceptualization: RR, CC, AG; Methodology: RR, CC, DS; Formal analysis and Investigation: CC, DS, VS; Writing-Original draft preparation: AG, RR, DS; Writing - Review & Editing: CC, VS.
Statement of Ethics
Ethical approval was taken from institutional ethical committee(ECR/270/Inst./2002014). The present research complies with the guidelines for human studies and the research was conducted in accordance with the World Medical Association Declaration of Helsinki. Informed consent was obtained from the participating patients.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.