
Abstract
Rationale:
India has a high prevalence of noncommunicable diseases (NCDs), which can be lowered by regular physical activity. To understand this association, recent population data is required which is representative of all the states and union territories of the country.
Objective:
We aimed to investigate the patterns of physical activity in India, stratified by zones, body mass index (BMI), urban, rural areas, and gender.
Method:
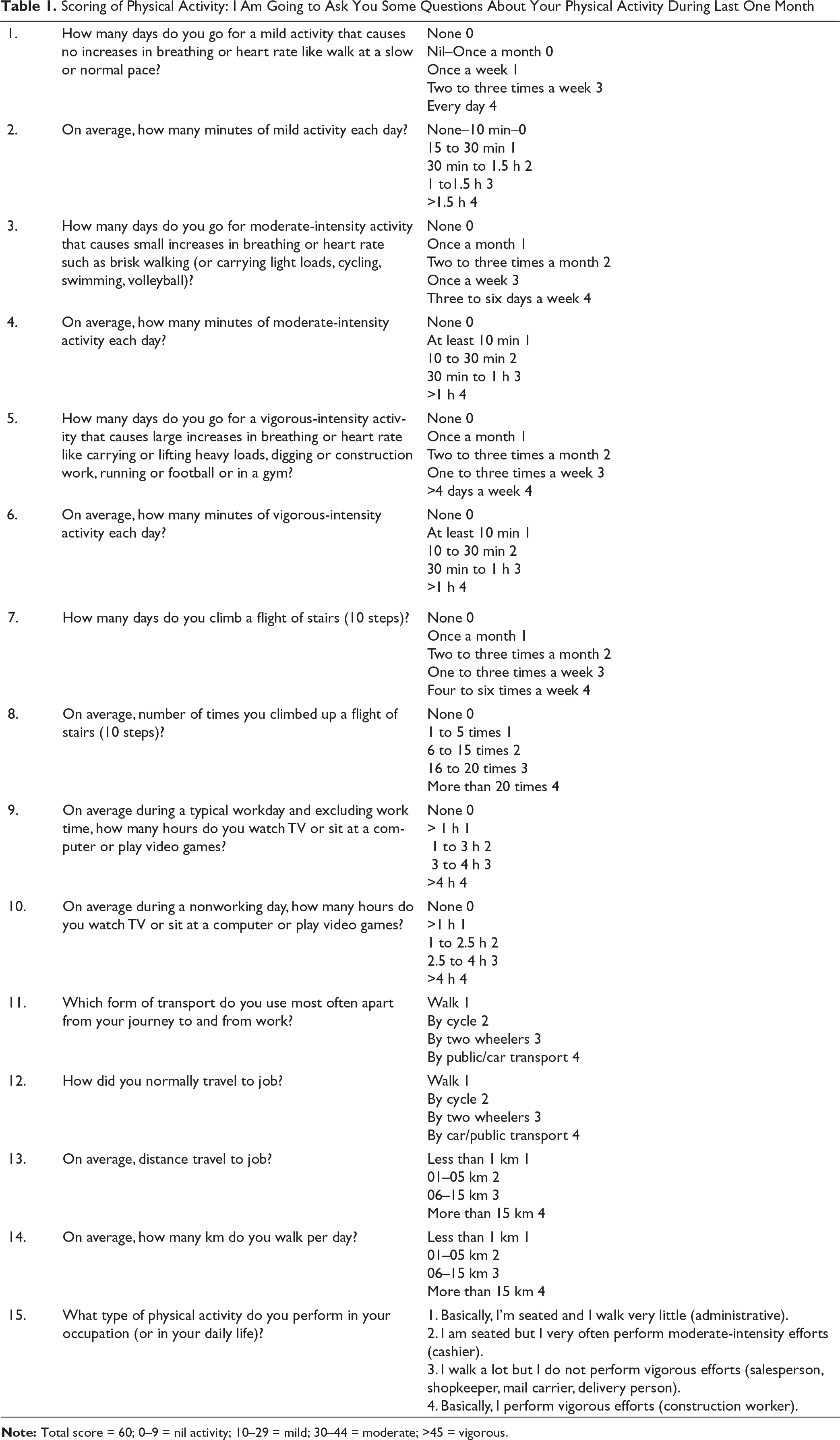
We present the analysis of physical activity status from the data collected during the phase 1 of a pan-India study. This (Niyantrita Madhumeha Bharata 2017) was a multicenter pan-India cluster sampled trial with dual objectives. A survey to identify all individuals at a high risk for diabetes, using a validated instrument called the Indian Diabetes Risk Score (IDRS), was followed by a two-armed randomized yoga-based lifestyle intervention for the primary prevention of diabetes. The physical activity was scored as per IDRS (vigorous exercise or strenuous at work = 0, moderate exercise at home/work = 10, mild exercise at home/work = 20, no exercise = 30). This was done in a selected cluster using a mobile application. A weighted prevalence was calculated based on the nonresponse rate and design weight.
Results:
We analyzed the data from 2,33,805 individuals; the mean age was 41.4 years (SD 13.4). Of these, 50.6% were females and 49.4% were males; 45.8% were from rural areas and 54% from urban areas. The BMI was 24.7 ± 4.6 kg/m 2 . Briefly, 20% were physically inactive and 57% of the people were either inactive or mildly active. 21.2% of females were found physically inactive, whereas 19.2% of males were inactive. Individuals living in urban localities were proportionately more inactive (21.7% vs. 18.8%) or mildly active (38.9% vs. 34.8%) than the rural people. Individuals from the central (29.6%) and south zones (28.6%) of the country were also relatively inactive, in contrast to those from the northwest zone (14.2%). The known diabetics were found to be physically inactive (28.3% vs. 19.8%) when compared with those unaware of their diabetic status.
Conclusion:
20% and 37% of the population in India are not active or mildly active, respectively, and thus 57% of the surveyed population do not meet the physical activity regimen recommended by the World Health Organization. This puts a large Indian population at risk of developing various NCDs, which are being increasingly reported to be vulnerable to COVID-19 infections. India needs to adopt the four strategic objectives recommended by the World Health Organization for reducing the prevalence of physical inactivity.
Introduction
Diabetes mellitus (DM) is a global pandemic and is straining the public health worldwide especially with the threat of coronavirus disease-2019 (COVID-19). Current global estimates of DM prevalence indicate that 415 million people are affected and are projected to escalate to 642 million by the year 2040.1, 2 India is one of the epicenter for this global pandemic of DM. Rapid demographic changes and socioeconomic development have likely contributed to the substantial rise in the prevalence of DM in India. The higher number of DM patients with consequent health complications substantially increase the health care burden and costs, and limit the quality of life.3, 4
Diabetes treatment in India has witnessed a rapid escalation in costs with increasing prevalence. It was previously reported that the annual cost on diabetes care was $227 in India, which substantially overburdened patients with DM because 85% to 95% of their estimated health care costs are borne by these individuals and their families. 5 India is also facing an additional burden on the health care system because of the rapid increase in COVID-19. The explosive increase in its prevalence has been found to be associated with DM, which has been a result of the adoption of unhealthy lifestyles. A few of the major modifiable risk factors for many noncommunicable diseases (NCDs), including DM, are physical inactivity and unhealthy diets.
Many NCDs, such as coronary artery disease, hypertension, DM, breast and colon cancer, can be prevented and treated by regular physical activity. However, a recent study revealed a higher (27.5%) global age-standardized prevalence of suboptimal physical activity in 2016, with the lowest levels seen in East and Southeast Asia (17.6%). 6 Because of the strong association between physical inactivity and NCDs, the World Health Organization (WHO), by 2030, has agreed to a global target of 15% reduction in physical inactivity, so as to accelerate the prevention and treatment of NCDs. 7
Additionally, the COVID-19, caused by the SARS-CoV-2 virus, pandemic has caused a devastating threat to the health, economy, and lifestyle. Several studies have showed that the aged population with comorbidities (e.g., DM, hypertension, chronic obstructive pulmonary disease or any respiratory illnesses, liver or renal diseases) have a higher risk of morbidity and mortality from COVID-19 because of an increased rate of hospitalization and intensive care unit admissions.8, 9 Currently, there are limited availability of effective vaccines and no available specific therapeutics for COVID-19, and thus implementing behavioral policies such as physical distancing can limit the spread of the virus and the resultant morbidity and mortality. 8 Moreover, public health recommendations of closing gymnasiums, parks, and fitness centers have resulted in a reduced scope for physical activity. Studies have shown that physical activity can boost our immune system and reduce the burden of the comorbid conditions, including obesity, DM, hypertension, cardiovascular and cerebrovascular diseases, which together can reduce the severity of COVID-19. 10 Earlier studies have shown that physical exercise impacts the antiviral defenses of the immune system.11, 12 For example, moderate-intensity exercises were found to counter respiratory viral infections by decreasing inflammation and improving the immune system. 12 In an animal experimental study, it was found that moderate-intensity exercises after or before infecting mice with influenza virus and herpes simplex virus type 1 resulted in reduced mortality and morbidity because of infections.13, 14 However, we have very
little evidence about how physical activity can interact with our immune system to fight SARS-CoV-2. Even though previous studies have been shown to exert immunomodulatory benefits, this will require retrospective studies to establish the relation of physical activity with SARS-CoV-2 infection outcome. 15 The scientific community is currently searching for the safe and effective vaccine against SARS-CoV-2 and its variants. As the physical fitness can augment seroconversion, it may potentially reduce the chronic inflammation and further improve the important immune markers in disease conditions. 8 Therefore, it is prudent to present the physical activity pattern in India as it can help in institutionalizing the effective public health policies to combat NCDs and COVID-19. Therefore, India needs to adopt effective national policies in solidarity with the global efforts led by the WHO. Nationwide and regional monitoring of current patterns of physical inactivity can enable the identification of high-risk groups and consequent effective planning. 6
There are several studies from western countries which have estimated patterns of physical activity; however, more extensive literature search reveals a paucity of studies from India that provide a nationally representative pattern of physical activity. Most of such studies were conducted in small scales and conducted in a few states and cities of India. A previous large-scale study on physical activity patterns in India was studied in three states and one union territory (UT) of India with a small sample size. Therefore, updated information about the physical activity pattern will help policy makers to review the efficacy of currently implemented policies and plan for the institution of better policy and programs based on validated and recent data.
The current nationwide study aims to investigate the physical activity patterns in India, stratified by zones, body mass index (BMI), urban, rural areas, and gender. To our best knowledge, this is currently the largest nationwide study in India investigating physical activity patterns with a
representative sample of 29 states and UTs.
Methodology
The data used in this analysis were collected during the phase 1 of the Niyantrita Madhumeha Bharata (NMB) 2017 trial, a large translational multicenter, cluster sampled research trial aimed to assess the efficacy of yoga-based lifestyle modification as a primary prevention strategy for diabetes in a community setting. The methodological details of the study have been reported previously.16, 17 In brief, the data collection was aimed at the screening of 4,000 adults per district in randomly selected 60 districts, representative of the Indian adult population.
Sample Size Estimation
Keeping in mind the twin objectives of the study, the sample size estimation was based on the relative risk reduction (30%) among prediabetics, reported in community lifestyle improvement program study. 18 We used annual incidence rates of diabetes as 18.3% in the control conditions as per Indian Diabetes Prevention Programme (IDPP-1) study. 19
This provided a conversion rate at three-month follow-up to be 4.57% and 3.0%, respectively, for the control and intervention conditions. The required sample size for a two-group design, with α = 0.05 and (1-α) = 0.80, was estimated to be 1,949 for each group (a total of 3,898 individuals). Factoring an attrition of 20%, the final sample size was estimated to be 4,678 individuals with prediabetes. To obtain 4,678 individuals with prediabetes, it was calculated that there was a need to screen 77,967 adults above the age of 20 years (4,678 × 100/6); the least reported prevalence of prediabetes in India has been 6.0%. 21 Thus, the study plans included a screening of approximately 1,55,933 individuals across 60 Indian districts (10% of all districts as per the 2011 Census of India), assuming a nonresponse rate of 50%. Consequently, the study targeted approximately 4,000 adults per district with equal involvement of the urban and rural areas.
Assessments
Scoring of Physical Activity: I Am Going to Ask You Some Questions About Your Physical Activity During Last One Month
Sampling Strategy
NMB 2017 had dual objectives, namely a survey for the prevalence and lifestyle intervention for the population at high risk and known diabetes. Details of the methods have been published earlier.16, 17 In brief, a four-stage [zone–state–district–town, ward, census enumeration block (CEB) in urban/villages in rural] strategy was adopted for identifying the study locations. Clustering was performed by dividing each state into districts, and each district into rural and urban localities. CEB were randomly selected from the randomly selected wards, and all eligible individuals (both genders between 20 and 70 years) within the CEB were contacted. The door-to-door survey enlisted eligible individuals and specifically enquired about the status of diabetes and scored them on the IDRS.
Ethical Statement
The study was conducted after getting the ethical clearance from the Institutional Ethics Committee (IEC) of the Indian Yoga Association (IYA) vide IEC reference no: RES/IEC-IYA/001 (dated 16/12/16). Data was collected among the participants with age >18 years after obtaining their informed consents during the door-to-door survey.
Statistical Statement
The statistical analysis was done using the Statistical Package for Social Sciences (IBM Statistics for windows, SPSS v23.0) at the Swami Vivekananda Yoga Anusandhana Samsthana, Bengaluru, India. The physical activity scores obtained from the 15 questions were classified as mild, moderate, vigorous activity, and inactivity for IDRS scoring based on our total score (0–9 = inactivity; 10–29 = mild; 30–44 = moderate; >45 = vigorous). A further analysis was carried out by stratifying them based on zones, age, region, BMI, and DM status.
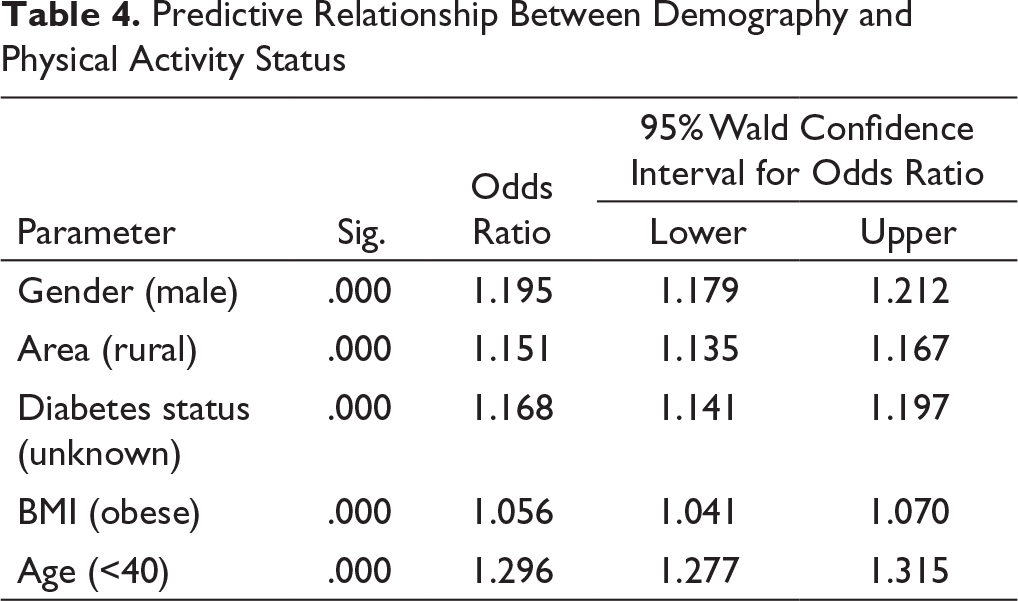
For every variable, a cross-tabulation of activity with gender, area, age (<40 and >40 years), region, and BMI was done with physical activity categories. A weighted prevalence was calculated based on design weight (which was calculated zone-wise based on the census population and response samples of each zone) and nonresponse rate. It was weighed by using SPSS weighing cases. Cross-tabulations and frequencies were calculated by putting the response rate as weight. We have checked the statistical significance through chi-square test. For odds ratio calculation, we did ordinal regression, with physical activity as response, and known–unknown diabetes, obese–normal, age <40 and >40 as predictors.
Results
Of the 2,40,000 people approached, 2,33,805 responded (nonresponse rate of 3%) from 29 out of 35 states and UTs except small remote states/UTs (Daman and Diu, Dadra, Sikkim, Nagaland, and Lakshadweep). There were 99% respondents from the north zone, 99% from northwest (Jammu and Kashmir), 99% from central, 99% from east, 99% from northeast, 98% from south, and 98% from west. Of these, 50.6% were females and 49.4% were males. The mean age was 41.37 ± 13.4 years. The study population constituted participants from both rural (45.8%) and urban (54%) areas. The mean BMI was 24.7 ± 4.6 kg/m 2 .
Patterns of Physical Inactivity (Overall and Zone-Wise) in India
Zone-Wise Distribution of Physical Activity in India (n = 2,33,805)
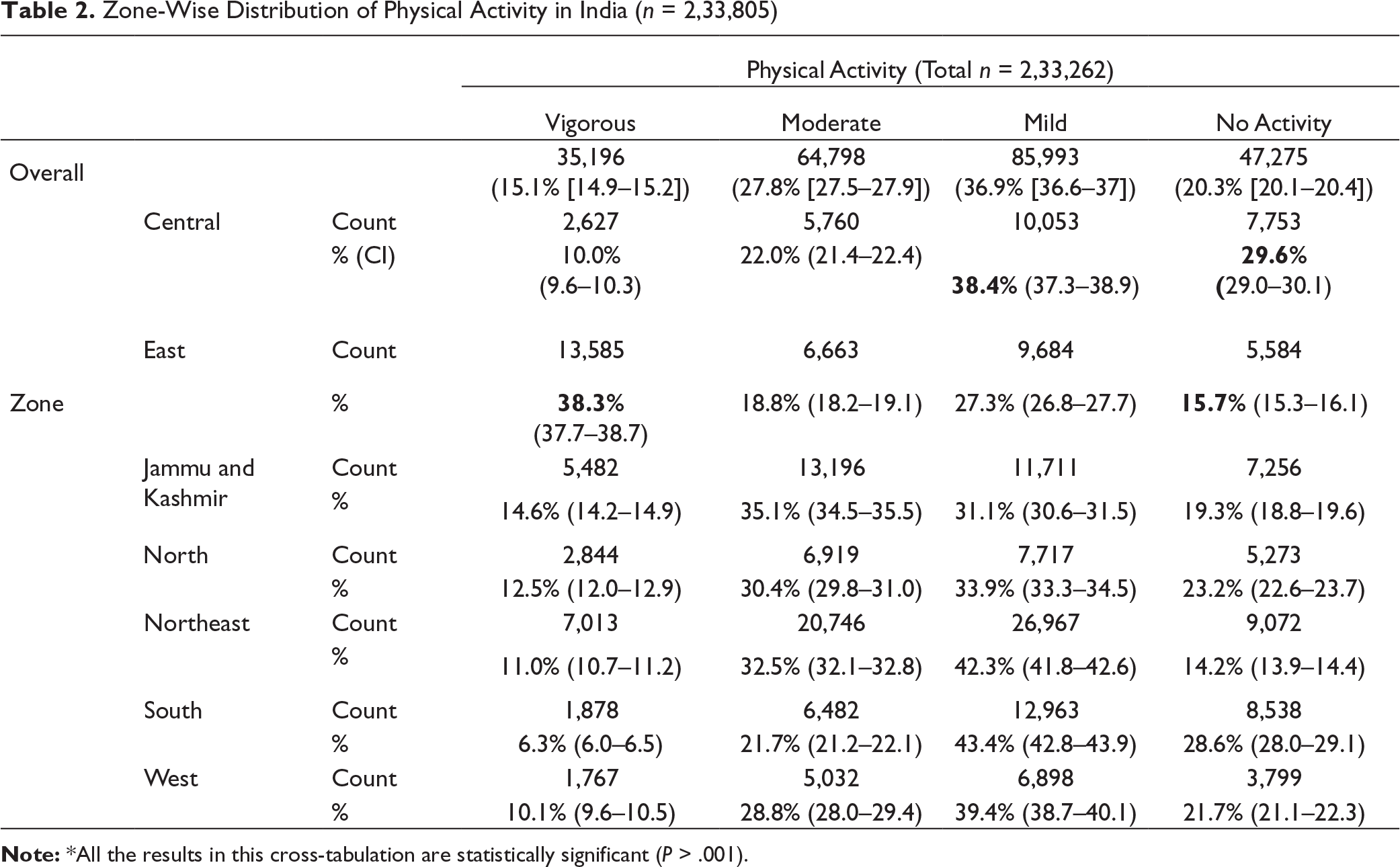
The zone-wise physical inactivity pattern was 29.6% (95% CI [29, 30.1]) in the central zone, 28.6% (95% CI [28, 29.1]) in south, 23.2% (95% CI [22.6, 23.7]) in north, 21.7% (95% CI [21.1, 22.3]) in west, 19.3% (95% CI [18.8, 19.6]) in Jammu and Kashmir, 15.7% (95% CI [15.3, 16.1]) in east, and 14.2% (95% CI [13.9, 14.4]) in northwest (Table 2). Therefore, the central and south zones had a higher proportion of individuals belonging to the no activity category, while the northwest zone had a fewer people in the same category.
The people from south (43.4%, 95% CI [42.8, 43.9]) and northeast (42.3%, 95% CI [41.8, 42.6]) had more representation in the mild activity category than the east zone people (27.3%, 95% CI [26.8, 27.7]). The people from the east zone were more (38.3%, 95% CI [37.7, 38.7]) in the vigorous activity category, as compared to those from the south zone (6.3%, 95% CI [6, 6.5]). When the zones were compared for minimum WHO recommended physical activity, then the east zone showed a higher proportion of people (51.7%) meeting the recommendation, whereas the south zone had a lesser proportion of people (28%) meeting the recommendation (Table 2).
Physical Activity Pattern in Relation to Age, Gender, Area, Diabetic Status, and BMI
Table 3 shows the association of physical activity with age, gender, area, and BMI. The prevalence of physical activity in India was analyzed. People over 40 years of age were more in the no activity (23.8% vs. 17.2%) or mild activity (39.6% vs. 34.5%) category, as compared to those under 40 years.
Gender, Area, and BMI-Wise Distribution of Physical Activity in India
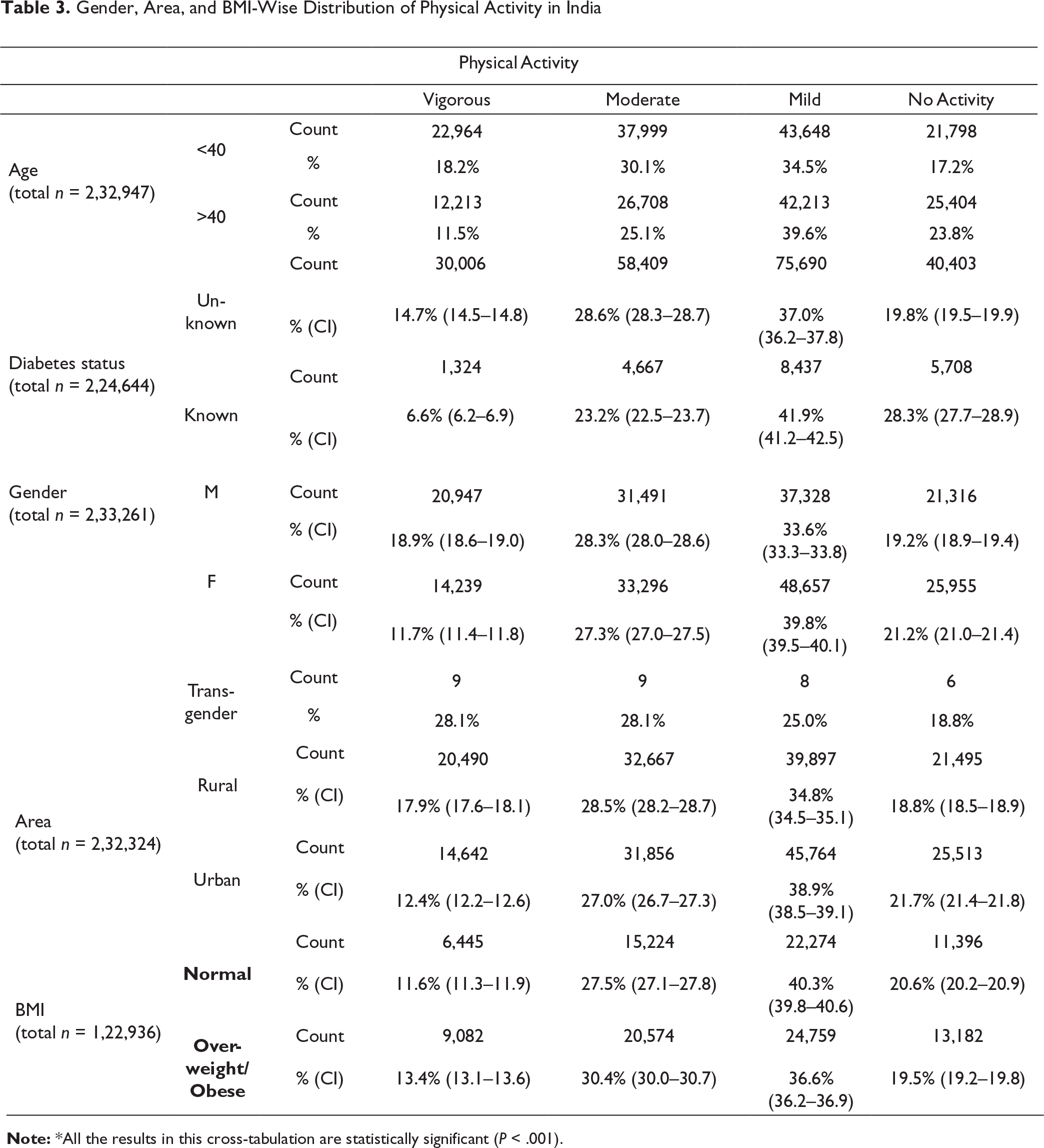
However, people with age less than 40 years were more in the moderate (30.1% vs. 25.1%) or vigorous activity (18.2% vs. 11.5%) category. When compared for WHO recommended physical activity, there were a higher proportion of people with age <40 years meeting the recommendation, in comparison to the older group (48.3% vs. 36.6%).
In our study, females were more in the mild (39.8%, 95% CI [39.5, 40.1] vs. 33.6%, 95% CI [33.3, 33.8]) and no activity (21.2%, 95% CI [21.0, 21.4] vs. 19.2%, 95% CI [21.0, 21.4]) category, as compared to the male population. In contrast, the males (18.9%, 95% CI [18.6, 19.0] vs. 11.7%, 95% CI [11.4, 11.8]) were more in the vigorous activity category, as compared to females.
Our findings showed that the urban population was found to be more represented in the category of mild (38.9%, 95% CI [38.5, 39.1] vs. 34.8%, 95% CI [34.5, 35.1]) and no activity (21.7%, 95% CI [21.4, 21.8] vs. 18.8%, 95% CI [18.5, 18.9]), as compared to the rural population. However, the rural population was found to be represented more in the vigorous activity group (17.9%, 95% CI [17.6, 18.1] vs. 12.4%, 95% CI [12.2, 12.6]), as compared to the urban people.
Interestingly, people who were aware of being diabetic were more in the category of no activity (28.3%, 95% CI [27.7, 28.9] vs. 19.8%, 95% CI [19.5, 19.9]) and mild activity (41.9%, 95% CI [36.2, 37.8] vs. 37.0%, 95% CI [36.2, 37.8]) when compared with those unaware of their diabetic status. When compared for WHO recommended physical activity, there were a less proportion of the known diabetic individuals meeting the recommendation (29.8% vs. 43.3%), as compared to the unknown diabetic individuals.
In case of people with normal BMI, a slightly higher proportion were in the no activity (20.6%, 95% CI [20.2, 20.9] vs. 19.5%, 95% CI [19.2, 19.8]) and mild activity category (40.3%, 95% CI [39.8, 40.6] vs. 36.6%, 95% CI [36.2, 36.9]), as compared to the obese people. However, the obese people were more in the vigorous (13.4%, 95% CI [13.1, 13.6] vs. 11.6%, 95% CI [11.3, 11.9]) and moderate activity category (30.4%, 95% CI [30, 30.7] vs. 27.5%, 95% CI [27.1, 27.8]), as compared to the people with normal BMI.
Predictive Relationship Between Demography and Physical Activity Status (Ordinal Regression)
Predictive Relationship Between Demography and Physical Activity Status
Discussion
This is the first ever largest comprehensive randomized pan-India cluster sample parallel survey on the patterns of physical activity in India. Our analysis of the data from 2,33,805 participants shows that a large proportion of the Indian population were physically inactive (20%) or mildly active (37%), respectively. This study further investigated the demographic relationship with the physical activity intensity and found that the urban population was more inactive (22%) or mildly active (39%) when compared with the rural population. Thus, only 40% of the urban population had met the recommended intensity of physical activity. A previous study conducted by Indian Council of Medical Research had also shown that the urban population was more physically inactive than the rural population. 21 However, because of the current larger sample size and random representation from both rural and urban areas of India, our findings are more representative of the physical activity status.
Diabetic people need intensive adherence to the physical activity regimen for good glycemic control and preventing diabetic complications. Therefore, diabetics are expected to be educated and motivated to comply with regular physical activity, and thus the current study sought to analyze the intensity of physical activity between known and unknown diabetic individuals. Surprisingly, 28% and 42% of people who were aware of being diabetic fall into no activity and mild activity category, respectively. Thus, only 30% of the Indian population met the WHO recommended physical activity intensity, posing a greater risk of poor glycemic control and increasing complications. We did not explore the factors responsible for the poor physical activity status in this group, and thus future studies on knowledge, attitude, and practice among these categories of population would provide additional insights.
The need to remain physically active becomes more pronounced with advancing age because of the risk of chronic illness. We found that people over 40 years of age are more likely to be inactive or mildly active when compared with people below 40 years, posing a greater risk of developing chronic illness.
In our study population, females were found to be more inactive or mildly active than males. In fact, approximately half of the male population studied had performed moderate- to vigorous-intensity activity. Previous studies had also reported a higher level of physical activity in males as compared to females.24–26 Several barriers might be contributory to lower physical activity among females, such as the lack of time, awareness, motivation, and access to safe roads, unfavorable sociocultural norms, household responsibilities, and the lack of social support and facilities (e.g., park, footpath). 27 Tripathy et al. had described that urban males reported higher physical activity levels, whereas rural females were engaged more in vigorous activity, which closely resembles our study where males were more active. 28
Our findings showed that the central (30%) and south zones (29%) had the highest prevalence of physical inactivity while the northwest zone (14%) had the lowest prevalence. The south zone also had the highest prevalence (43%) of mildly inactive people. Thus, only 28% of the south Indian population met the WHO recommendation, making this zone most vulnerable to chronic illness. The higher physical inactivity in the south zone could be related to their sedentary occupation. 29
Over the past decade, several studies conducted in developed countries have reported a higher
prevalence of physical inactivity. For example, a higher prevalence of physical inactivity was reported in the USA (49.4%) and Sweden (31%).21, 30 On the other hand, an Indian study also reported a higher prevalence (50%) of physical inactivity in four regions of the country. 31 The findings of our study show a lower prevalence of physical inactivity across all states when compared with the previous reports. The difference could be because of the fact that the earlier study was undertaken in three states only with a comparatively lower sample size (14,227) 32 than ours (2,33,805), and thus it may have overestimated the actual prevalence. Another study analyzing the global trends in insufficient physical activity revealed the global age-standardized prevalence in 2016 to be 27.5% with the lowest levels seen in East and Southeast Asia (17.6%). This suggests that India has a higher prevalence of physical inactivity than the regional average. 6 The current trends in the prevalence threaten the current global target of 15% reduction in the prevalence of suboptimal physical activity. 7
A systematic review showed that physical activity can reduce the premature mortality and prevent at least 25 chronic conditions. 32 Pedersen reported that high-intensity physical training provides the additional disease protection, improves cardiorespiratory fitness, promotes longevity, and slows down aging. 33 In contrast, Warburton and Bredin described a curvilinear relationship between physical activity and health outcomes, which explains that the observed benefits can be accrued even with mild intensity of activity. 32 For example, studies have showed that physical activity can protect against both the early and late development of age-related macular degeneration (AMD), which is a leading cause of blindness. 34 However, several studies found the increased risk of developing AMD in the Indian population due to genetic predisposition, which may further increase in the background of physical inactivity.35–40
A growing body of evidence suggests that physical activity is a gene modulator inducing structural and functional brain changes, which in turn benefits cognitive abilities and protects against neurodegenerative disorders. It is also important to understand the underlying pathophysiology of cognitive impairment in physically inactive patients, so that genetically susceptible groups of patients could be pharmacologically targeted. Several studies have investigated dementia, Alzheimer’s disease, and neurodegenerative disorders in preclinical testing and provided new insights for a clinical translation and developing new drug targets.41–43
The WHO recommends 150 min of moderate aerobic activity or 75 min of vigorous-intensity activity weekly to prevent inactivity-linked NCDs. According to our study, 57% of the Indian population do not meet the minimum WHO recommendations. India has an estimated population of 1.38 billion, which is equivalent to 17.7% of the total global population. 36 Thus, the current suboptimal adherence to recommended levels of physical activity can potentially risk a greater proportion of the Indian population to develop or exacerbate different NCDs.
The rising morbidity and mortality of NCDs have partly been associated with a rising prevalence of physical inactivity. The demographic shift and changed lifestyle have contributed partly to the rising epidemic of NCDs. 28 In addition to modern lifestyle behaviors contributing to physical inactivity and sedentary lifestyle, physical distancing and quarantine measures have further aggravated the current state of physical inactivity. Thus, our findings are relevant to the current COVID-19 pandemic so as to map out the current state of physical activity levels and establish exercise programs, considering the current public health recommendations of physical distancing and hygiene. For example, people can be more active by avoiding sitting for longer periods, taking short movements, online exercise sessions, wearable sensors, and home exercises, such as yoga, stair climbing, and rope jumping. Studies have investigated the effect of yoga on communicable diseases 44 as well as the effect of other physical exercises. For instance, the meditation or exercise for preventing acute respiratory infection-1 (MEPARI-1) trial, investigating the effect of mindfulness-based stress reduction training or sustained moderate-intensity exercises, found significant reductions in acute respiratory illness, which suggests the potential role of yoga during the COVID-19 pandemic. 45
In addition to increasing morbidity and premature mortality, insufficient physical activity can substantially impose an economic burden on health systems and society. It was estimated globally in 2013 that the inactivity had cost $54 billion in direct health care with 1% to 3% national health expenditures attributable to it.7, 46 The economic burden substantially impacts health systems in developing countries like India where the health care system is overburdened, and most people pay health care costs from their pockets.
The WHO has recommended four strategic objectives requiring an active society with active people and active environment and systems, achievable through 20 policy actions. 7 Our nationwide study can serve as an important template for appropriate policy adoptions and optimal resource allocations. India should make a concerted effort with the WHO global action plan by adopting robust national policies at a large scale to encourage using nonmotorized transportation. However, this will require a provision of safe walking and cycling infrastructure, improving safety in roads, and expanding the scope for physical activity in different settings, such as public place and in workplaces.47
Limitations
There are some limitations to this study. Social desirability and recall bias in the study participants because of a self-reporting questionnaire might have led to over- or under-reporting of physical activity levels. The NMB program was discontinued in Kerala because of the illness of the key trained field researcher; however, this may not impact the nationwide prevalence because of it being a small state. However, a state-wise subanalysis may not yield the pattern of the physical activity in Kerala. As our study recruited participants over 18 years of age, the findings are not representative of the population below 18 years. The study did not analyze the physical activity pattern based on individuals’ existing comorbid conditions. At the time of carrying out this study, the implications of this study on the COVID-19 pandemic were not foreseeable; therefore, the current state of physical activity, because of lockdown policies and social distancing, may not be completely understood based on our study findings.
Conclusion
Our current study shows the most updated data on the current prevalence estimates of the patterns of physical activity in India. The results show that 20% and 37% of the population in India are not active or mildly active, respectively, and thus 57% of the population has failed to comply with the WHO regimen for physical activity. The current estimates indicate that a larger population of India is at risk of developing NCDs including DM. In addition, the existing state of physical inactivity intensified by current lockdown policies because of COVID-19 also pose a greater risk of severe illness from the disease. This can be improved by promoting home-based exercises, such as yoga. Thus, India and the world need to adopt effective national policies and planning in concert with WHO strategic objectives. This will help to meet the global target for the reduction of insufficient physical activity, and thus will contribute to reducing the national and global burden of the rapid rise of NCDs and COVID-19 on the health systems and in turn reducing associated mortality and morbidity.
Footnotes
Author Contribution
VP–writing the original draft of the manuscript, editing, compiling, submission of the manuscript; RN–
conceptualization of the manuscript, methodology, and validation; AA–concept of the manuscript; SP–data analysis; AS–data collection; HRN–conceptualization of the project.
Acknowledgment
We acknowledge the support of CCRYN, MOHFW, and IYA for manpower, cost of investigations, and overall project implementation, respectively.
Declaration of Conflicting Interests
Funding
This study was funded by IYA, Central Council for Research in Yoga and Naturopathy (CCRYN), Ministry of AYUSH, Ministry of Health and Family Welfare, Government of India (grant no: F.No. 16-63/2016-17/CCRYN/RES/Y&D/MCT/Dated: 15.12.2016).