
Abstract
Background:
Progressive neurological genetic diseases are not rare. They cause psychosocial damages to its victims. This article focuses on common psychosocial issues faced by those from the developing world.
Methods:
A multicentre observational survey of 246 patients from teaching hospitals in Sri Lanka. Participants were clinically and genetically confirmed by neurologists and the Interdisciplinary Centre for Innovation in Biotechnology and Neuroscience (ICIBN) respectively from 2014 to 2018. Convenience sample with random geographical distribution. Factors were equally weighted. ANOVA, Student’s t-test and chi-square analysis were used. Statistical Software R Statistics—version 3.5 and one-sample t-test with CI = 95% was used. This study meets the ethical guidelines of the local institutional review boards which are in compliance with the Helsinki Declaration.
Results:
Sample included 184 males and 62 females of 3–76 years with either Duchenne muscular dystrophy (n=121), spinocerebellar ataxia (n = 87) or Huntington disease (n = 38). Mean income of the affected is lower than the standard average monthly income (P ≤ .001). Consultation visits depend on the monthly income (CI 20421.074–34709.361; P ≤ .001).
Conclusion:
Poverty is inversely proportionate to the patients’ living conditions. As developing countries are financially challenged, it is a societal challenge to rebuild our values to enhance their living status.
Introduction
Being unwanted, unloved, uncared for, forgotten by everybody, I think that is a much greater hunger, a much greater poverty than the person who has nothing to eat. —Mother Teresa Poverty is the worst form of violence. —Mahatma Gandhi
Poverty is a major cause of ill health and a barrier to accessing healthcare when needed. Ill health, in turn, is a major cause of poverty. This is partly due to the costs of seeking healthcare, which include not only out-of-pocket spending on care but also transportation costs and any informal payments to providers. It is also due to the considerable loss of income associated with illness in developing countries, both of the breadwinner and family members who may be obliged to stop working or attending school to take care of an ill relative. In addition, poor families coping with illness might be forced to sell assets to cover medical expenses, borrow at high interest rates or become indebted to the community. 1
Genetic disorders can create a whole package of problems socially, economically for an affected family and to the society that will consume 5%–10% of the total health budget of a country for treatments. In Sri Lanka and India common monogenic and complex disorders including neurodegenerative disorders such as Duchenne muscular dystrophy, Huntington's disease, spinocerebellar ataxias2, 3, 13–19 and congenital disorders remain high with rising concern towards the necessity for a genetic testing service. Genetic testing in Sri Lanka is almost non-existent in government hospitals and only confined to a few centres in the private sector. The corresponding author has been successful in establishing the one and only free genetic testing service for selected neurodegenerative and neuromuscular disorders. To date, this service is able to provide genetic testing reports worth of few millions of Sri Lankan rupees.
Case 01
A wheelchair-bound teacher with a family history of spinocerebellar ataxia type 1 shared her story of a failed marriage. The disease onset was seen during her second pregnancy, upon which her husband had demanded for an abortion as he did not want any more ‘sick’ individuals in his family. After refusing to have abortion, she was harassed physically and mentally by the husband and the mother-in-law. Abortions are considered illegal in Sri Lanka. Due to depression she had attempted suicide by ingesting a toxic substance. Although she and the foetus had survived the incident, her husband forcefully took the guardianship of the first born. Hence, she had left the family to join her mother. Her mother was having multiple comorbidities, although she remains the only support system for the patient. Currently, all three live under a barely constructed house with a single room. Even if her first child does not even recognize her anymore and has no contacts with her, she is determined to give a better education to her second child and take him to the epitome of success.
Case 02
Two wheelchair-bound teenage boys presented with Duchenne muscular dystrophy. Their mother being a housewife and the father being a labourer hardly earn a living. Even with disabilities, the older sibling had won a gold medal from an all-island art competition. The parents yearn to fulfil their children’s needs to the best of their abilities even though that demands cutting down their fundamental needs including the money they spend on meals. Even with such effort, they only save enough to take their children to the leading children’s hospital annually, because the cost it takes to travel to the hospital with their two wheelchair bound children is greater than their monthly income.
Case 03
One family visit revealed a dependent woman in her 60s with Huntington disease, confined to bed in a secluded room without ventilation. This patient with urine incontinency was kept on a mattress that was soaked in urine, under which crawled maggots. Her adult son was waiting till his mother dies because the family no longer wanted to support her needs. Although financially stable, she was unable to live the final stage of her life with tender loving care.
Methodology
A multi-center observational survey was conducted on patients identified after through neurological examination at teaching hospitals in Sri Lanka from 2014 to 2018. Initially, 292 patients who were clinically diagnosed by consultant neurologists were referred for the genetic testing at ICIBN, University of Sri Jayewardenepura, Sri Lanka. This survey included 246 participants (males n = 184, females n = 62) of 3–76 years, who were genetically confirmed for Duchenne muscular dystrophy (n = 121, age range 2–18, mean age: 9 years), spinocerebellar ataxia (n = 87, age range 21–73, mean age: 44 years) and Huntington disease (n = 38, age range 25–59, mean age: 45 years). Written informed consents were obtained from every participant where applicable. For incompetent patients, surrogate consent was taken. Clinical data and sociodemographic information were collected using standard questionnaire and clinical batteries. This study meets the ethical guidelines of the local institutional review boards which are in compliance with the Helsinki Declaration. All factors were equally weighted. ANOVA, Student’s t-test and chi-square analysis techniques were used as the statistical tests. Statistical Software R Statistics—version 3.5 was used with extension packages. Analysis was done using one-sample t-test with confidence interval of 95%.
Results
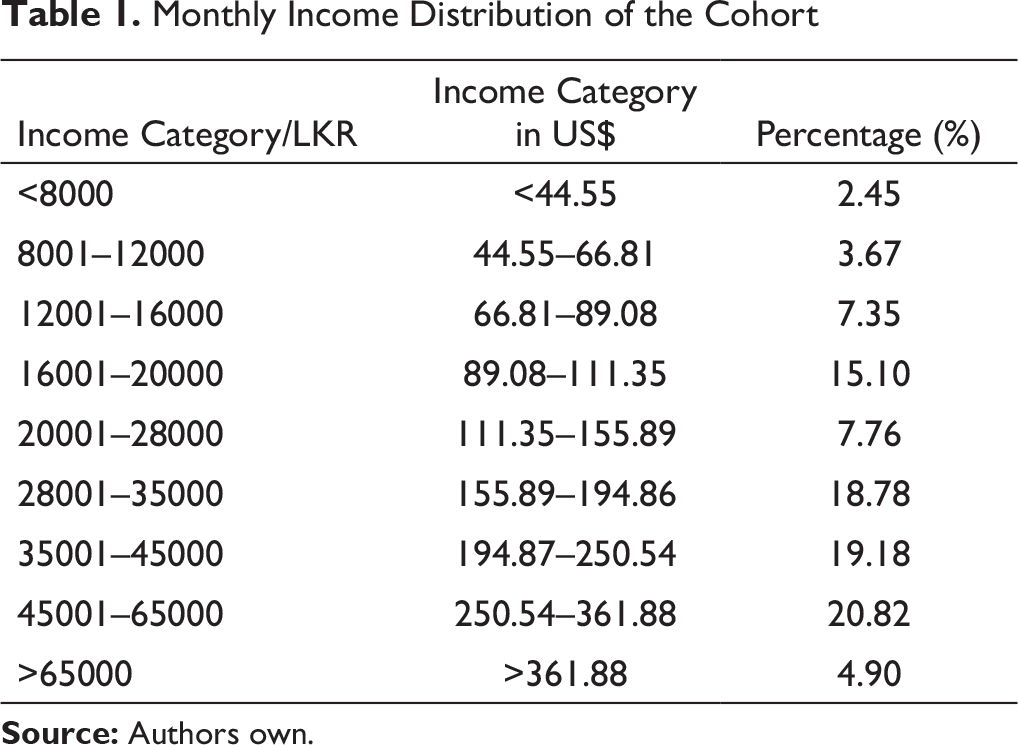
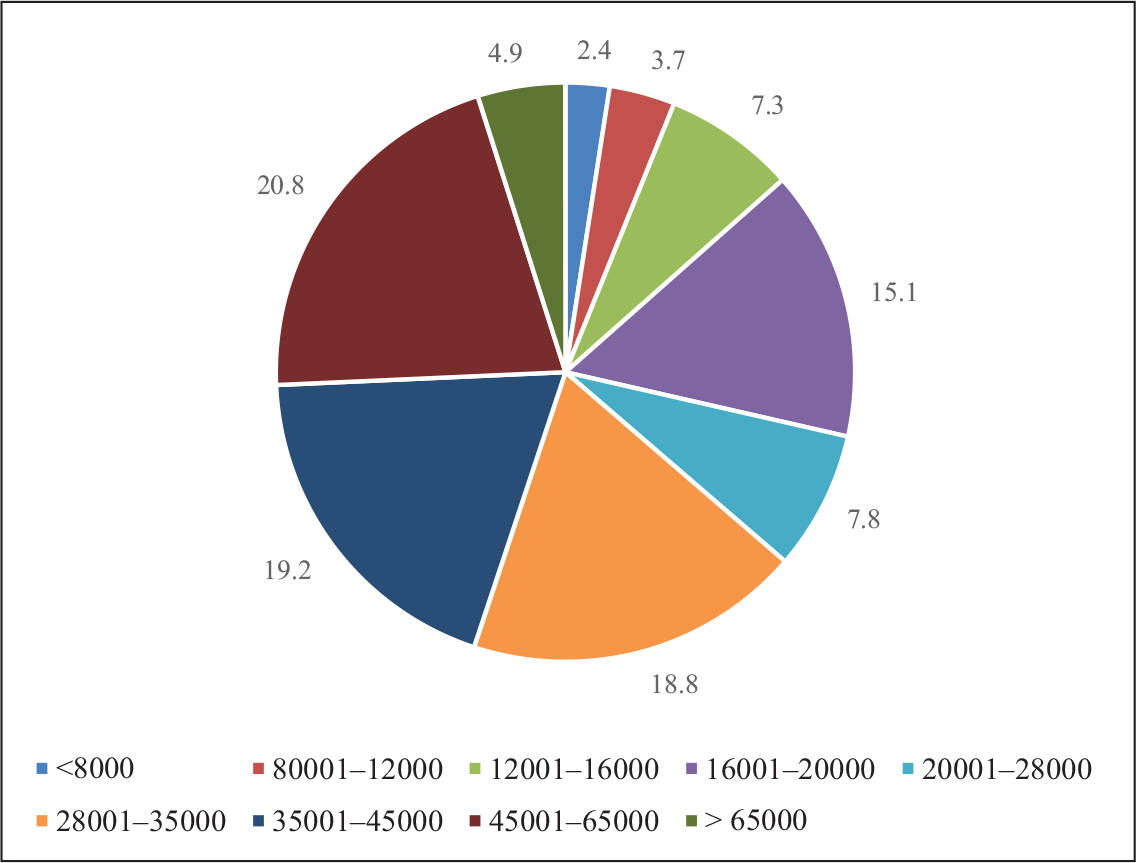
Monthly Income Distribution of the Cohort
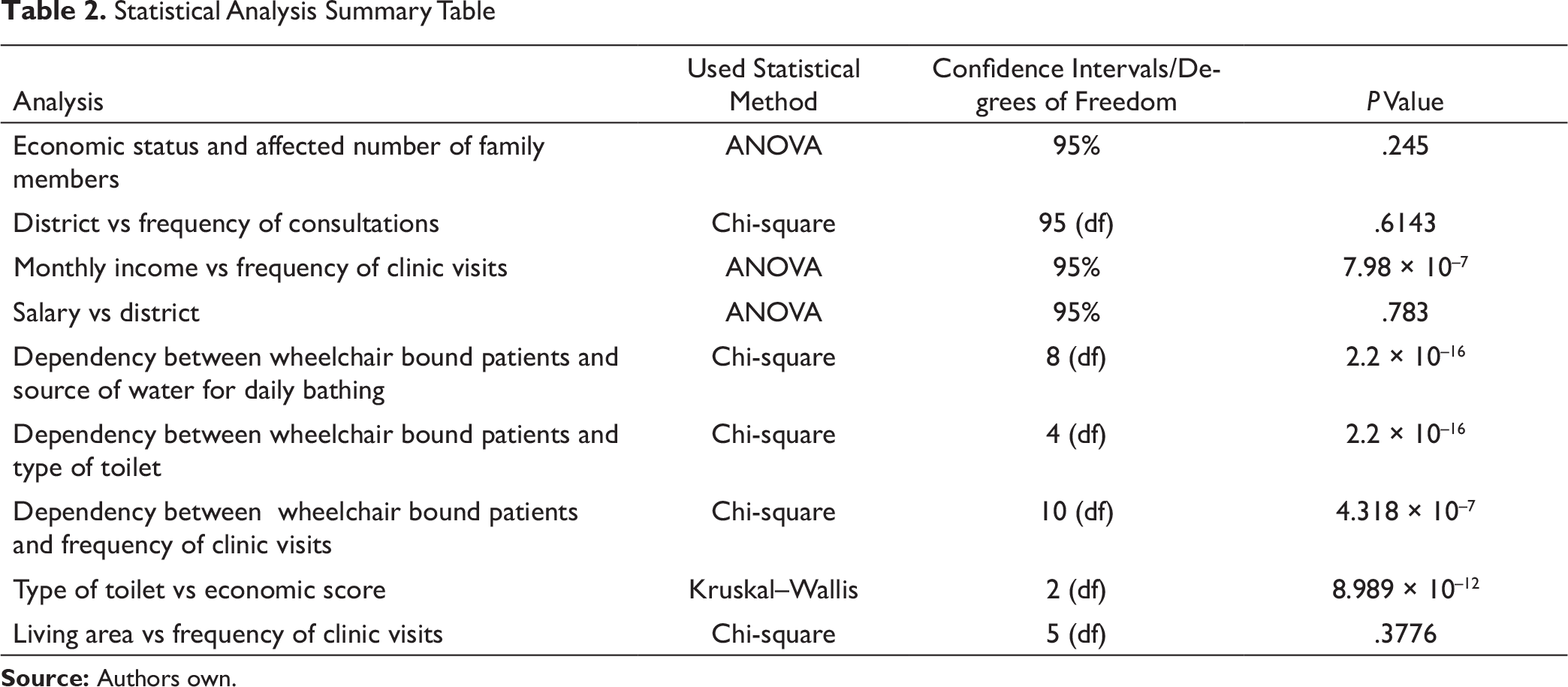
Statistical Analysis Summary Table
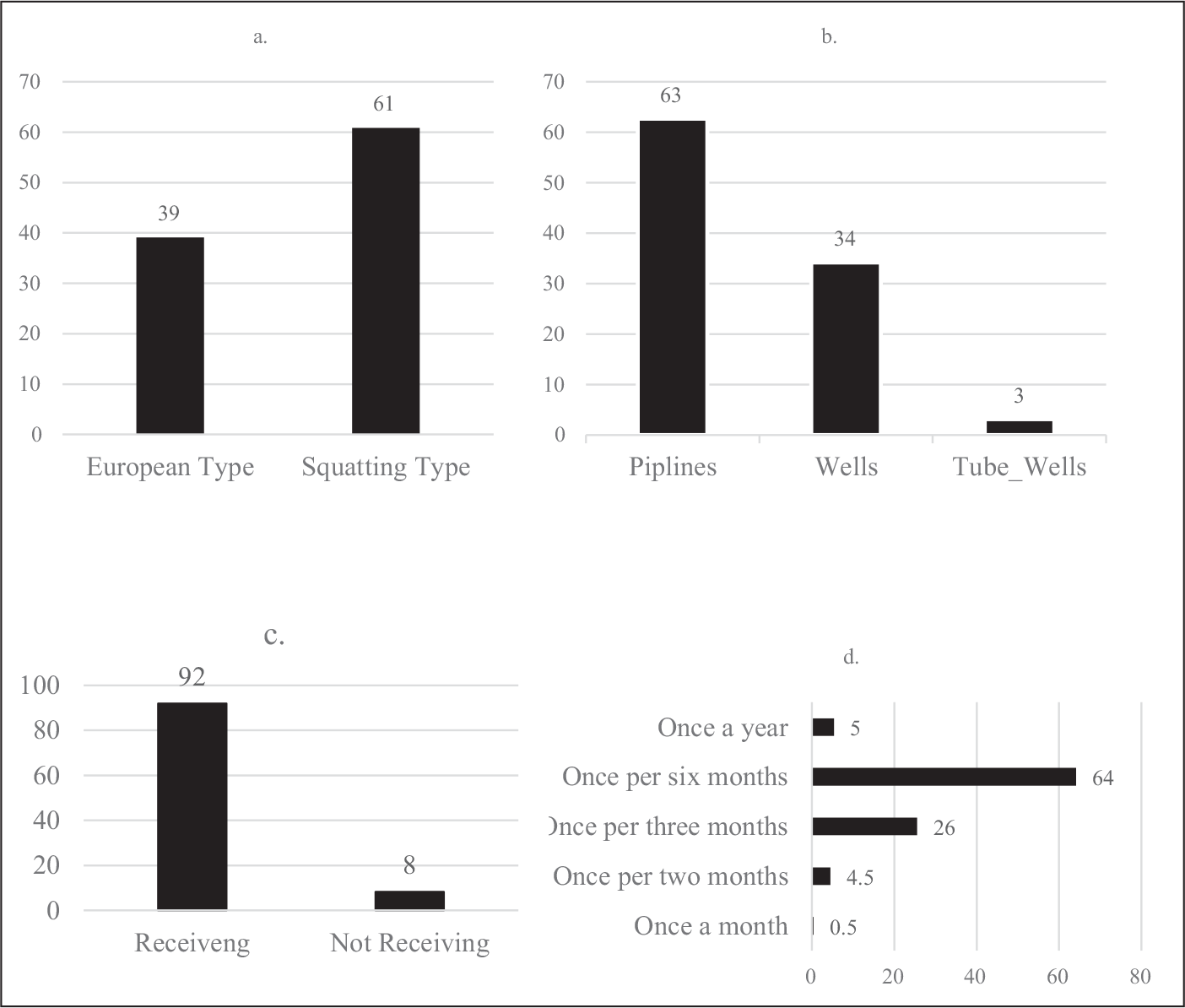
In the analysed population, 61% of patients use squatting type toilets (Figure 2a), 63% of patients use pipelines as the water source (Figure 2b), 92% receive neurology consultations (Figure 2c), while 64% of the cohort consult a neurologist once in every 6 months (Figure 2d).
Discussion
Although progressive neurological genetic diseases are not rare in the world, including developing countries, they cause grave psychosocial damages to its victims.4–6 Throughout the world 7.6 million children are born annually with a severe genetic disorder or birth defect, out of which nearly 95% of them are from the developing countries. The prevalence and burden of genetic disorders, birth defects and common complex diseases are generally higher in developing countries.7, 8 The aforementioned cases illustrate the common psychosocial issues displayed in this cohort.
At a time where the inherited disease community remains as a highly neglected cluster within Sri Lanka, ICIBN-USJ being the only centre in the state sector provides free neurogenetic testing service facilitating the vision emphasized by the World Health Organization in terms of ‘harnessing the genomic knowledge and have it contribute to health equity, especially among developing nations’. However, 5,000– 10,000 LKR (27–54 USD) is spent on chemicals and consumables per test, where the cost is mainly covered by funding obtained by the principal investigator through international and local funding agencies. Thus, the authors request from the philanthropists and nongovernmental organizations to facilitate free molecular diagnostic services in developing countries.
The ongoing research and free molecular diagnostic service at ICIBN-USJ has resulted in the establishment of a unique national biobank. Our goal is to foster the research and educational aspirations of the inherited disease community through international collaboration in research leading to double doctoral degrees in human resource development, clinical trials and patient registries, advancing the search for new/modifier genes, founder effects, admixtures and pharmacogenetic effects utilizing this national biobank with the following assets as at May 2020:
DNA bank with associated sociodemographic and clinical data from
Over 2,000 patients, with the following breakdown: Stroke—500, Parkinson’s disease (PD)—370, and controls—500. Genetically diagnosed/genetically negative for common mutation patients in the following numbers: Duchenne muscular dystrophy—178/27, spinal muscular atrophy—24/11, limb-girdle muscular dystrophy—1/15, Huntington’s disease—39/38, spinocerebellar ataxia—69/127, myotonic dystrophy—4/2. ‘Brain Bank’ with 76 autopsy brain samples from ageing individuals, with immunohistochemical stains for neuropathological markers associated with dementia-related disorders and genotyping data on candidate genes for stroke. Serum and urine samples from patients with DMD, SCA and HD.
Poverty and Heath
As these diseases are often not recognized, prevention through proper guidance is not anticipated leading to a high cost to the affected individual, their families and the healthcare sector.7, 8 Typically, nearly 50% of medical expenses in low-income nations are derived from out-of-pocket payments, compared to 30% in middle-income nations and 14% in high-income nations. 9
According to the data collected through the survey it was evident that the frequency of neurological consultations depends on the monthly income of the affected family (P ≤ .001). It should be noted that even among our cohort, 16% (DMD, n =12; SCA, n = 19; HD, n = 08) was already wheelchair-bound. The minimum mean distance the patients have to travel to reach the closest regional hospital ranged between 40 km and 50 km. However, being a Third World country the public transport system in Sri Lanka is poor. With disease progression, patients find it cumbersome to use ordinary infrastructure because most public places, even the transport system or ordinary schools, lack facilities for the disabled. This issue is not given priority due to financial constraints. Consequently, patients find it difficult to reach out for medical care. This scenario is highlighted in Case 02 where the cost it takes to travel to the hospital with wheelchair-bound children is greater than their monthly income.
There was a significant association between wheelchair-bound patients and the frequency of clinic visits (P ≤ .000). Monthly income and the frequency of visits as well as wheelchair-bound patients and the frequency of their clinic visits are significantly associated with each other (Table 2).
According to Sri Lankan census in 2016, the average household income in rural and urban areas are 58,137 LKR (323.67 USD) and 88,692 LKR (493.79 USD), respectively. 10 The mean household income of an affected family is 30,531 LKR (169.98 USD) and 34,494 LKR (192.04 USD) in rural and urban areas, respectively (P ≤ .000). According to Table 1 around 60% of the affected have a monthly income that ranges between 28,000 LKR (155.89 USD) and 65,000 LKR (361.88 USD) (Table 1). One reason for this is when one member is suffering from a progressive disease, another adult in the family has to invest all of that individual’s time caring for the patient.
Caregivers tend to go from one doctor to another and from one treatment modality to another because of poor understanding about the disease and its management. Upon failure of this ‘doctor-shopping’ phenomenon, caregivers tend to give up on the patients resulting in confinement of the patient as shown in Case 03.
Although these diseases do not have a permanent cure, 55% of the considered sample leaned towards traditional medicine. Only 7% of those who received Ayurveda treatment had experienced improvement in the signs and symptoms of disease, while 47% of those who received traditional medicine reported satisfaction. Therefore, it is important to explore these medical modalities. If these positive methods are supported through evidence, a holistic approach can be implemented in handling these patients which would prevent patients from withholding treatment entirely.
Dependency between wheelchair-bound patients and source of water appears to be significant. These patients mostly use pipelines as the water source for bathing according to chi-square test results (P ≤ .001; CI: 5.50731). Type of toilets and the economic score and wheelchair-bound patients and the type of toilet used are significantly associated with each other (Table 2). They use European type of toilets according to chi-square test (P ≤ .001; CI: 9.48779). The Kruskal—Wallis test for the economic score and the type of toilets showed a significant association (P ≤ .001; chi-squared = 29.267; df = 4). The greater the patient is affected economically, the lesser the standard of the toilets. Most wheelchair-bound patients have squatting type toilets. Though most basic needs are covered in majority of the study sample despite their economic status, the attention towards utilizing European type toilets is limited (Table 2). Enlightening caregivers about improving the quality of life of patients even with small changes in the household is crucial.
Since the free health system is maintained in Sri Lanka, the medical insurance services are not well-established with low- and middle-income families to which most of our patients with neurogenetic disorders belong. Moreover, the established medical insurance policies in Sri Lanka hardly cover the expenses incurred at Out Patient Department tests, thus promoting indoor insurance covers.
Mobile clinics have been conducted by ICIBN-USJ around the country based on selected government hospitals for better availability, including the Northern Province (Jaffna Teaching Hospital), which was abandoned for nearly 30 years due to a civil war. Jaffna in the Northern Province is home to many consanguineous families. With the recent testing conducted there, new clusters of patients with clinical heterogeneity were identified. However, post-trauma stress of war that may have influenced these diseases was not systematically studied in these war-torn areas.
Tradition and Health
Before colonization, Sri Lankan tradition revolved around the concept of ‘religion and village’. The bond the villagers had for one another was exquisite. The superhuman qualities such as compassion, kindness and humanity were seen in the locals. The religious leaders acted as mediators between conflict groups and as a source of comfort in addressing mental turmoil. However, with globalization these qualities have dissolved, building high parapet ‘emotional’ walls in the community.
Although Sri Lanka is a multi-religious country, where many gloriously claim to be fully devoted, the core qualities of each religion have evaporated with time. Religious centres rarely function as a resource centre for the needy because of the busy lifestyle of the community. We believe it is the obligation of those centres to address the concerns of the villagers in a more fruitful manner so that everyone gets the due benefit. Not only can they function as a place that adds tranquillity to the minds of the affected, but they can also work at the initial level where fundamental human needs are addressed. We believe that if this support had been there, patients would seldom attempt suicide or deliberate self-harm.
According to Sri Lankan penal code, therapeutic abortions are only allowed when the mother’s life is at risk. 11 As noted in Case 01, abortions are desired and performed illegally and silently in the country. Victims tend to hide these progressive neuro-degenerative genetic diseases due to stigma and once known, the patient is segregated from the society. Hence, instead of due to these reasons patients remain underdiagnosed.
Parents suffer when a child is diagnosed with a genetic disease. Mothers show constant self-blame and experience pressure from their in-laws because they are branded as the root cause for the disease. Parents express fear of having more children. Due to lack of communication with the medical practitioners, they fail to find out about the alternative ways such as adaptation, surrogating and donor sampling methods. However, lack of availability and affordability also play a key role in limiting these options even when known.
Enhancing the qualities of humankind should be addressed from the primary education level where the children are taught to accept differences, share with the needed and be non-judgmental. Even though Sri Lanka has a total adult literacy rate of 91.2%, 12 these psychological aspects of the community remain unaddressed. This is indirectly the failure of emotional intelligence of the country as well.
Conclusion
Poverty is invariably increased in the affected people. As a developing country, addressing the fundamental needs of the affected is financially inconvenient. Instead of waiting till the governing bodies implement the needful, there are major changes we can adopt as a society to help those in need and reduce the stigma. It is a societal challenge to rebuild our deep-rooted traditional values to form a better community.
Footnotes
Acknowledgements
We are grateful to the patients and their family members for taking part in the study. Our thanks to Ms. M.K.D.K Attanayake and Mr. Yoonus Imran of Interdisciplinary Centre for Innovation in Biotechnology and Neuroscience, University of Sri Jayewardenepura, Sri Lanka for providing support.
Authors Contributions
N. S., N. W., L. G., P. D. are Research Assistants at the Interdisciplinary Centre for Innovation in Biotechnology and Neuroscience, University of Sri Jayewardenepura, Nugegoda, Sri Lanka and have co-written the final manuscript. I. G. is the statistician who contributed in co-writing the statistical analysis. Acquisition, analysis, or interpretation of data were done by I. G., L. G., and N. W.
P. R., D. S., H. G., A. D., S. S. are Consultant Neurologists and contributed in clinical aspect of the patients. A. A., K. S., A. D. provide academic guidance for the PhD students in Molecular Diagnostics. R. D. S. is the principal investigator and has developed the manuscript from its inception to the final version.
Declaration of Conflicting Interests
Ethical Statement
The study was approved by the Ethical Committee of Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka which is in compliance with the Helsinki Declaration (Ethics no 34/14 and 449/09).
Funding
This research was funded by World Class University Grant Project at University of Sri Jayewardenepura, Sri Lanka under Grant WCUP/PhD/19, WCUP/PhD/19B and Ministry of Primary Industries , Sri Lanka -SP/CIN/2016/02.