
Abstract
Background:
Some investigations point to the beneficial effects of yoga in alleviating the motor and cognitive dysfunctions in multiple sclerosis (MS) patients by using varying combinations of physical, breathing, and meditative practices of yoga. There is a need for a validated yoga module with a holistic approach that can be used as a standardized protocol by researchers and therapists.
Purpose:
To develop and validate an integrated yoga module for practice in relapsing–remitting MS patients to improve their quality of life.
Methods:
We did a thorough review of the literature for the development of the yoga module. We formed an expert group with 24 experts and a neurologist and used two rounds of interactive Delphi method to combine their opinion to obtain content validity of the module through online structured questionnaire prepared for the purpose on a Google Form. We incorporated all suggestions obtained by the experts. The final module (60 min per session, twice a day, five days per week) included warm-up exercises, customized asanas, relaxation techniques, and OM meditation. Advice on yogic diet and discussion using yogic concepts for stress management also form a part of the holistic approach to yoga lifestyle modification.
Results:
Analysis divulged that 30 out of 39 practices exhibited a content validity ratio value greater than or equal to 0.42.
Conclusion:
The study has shown good content validity of the integrated yoga module. Future clinical studies are being planned to rule the feasibility and reliability of this module.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and degenerative disease of the central nervous system, with highly diverse fallouts. Four patterns of the disease are seen in MS.1, 2
Types of MS
Among the four patterns of MS, relapsing–remitting is the most common pattern (80%–90%) of MS cases. This type is marked by the sudden worsening of symptoms or the emergence of new symptoms referred to as an exacerbation, relapse, flare-up, or attack,1, 3 followed by a period of improvement (remission), where the recovery may be partial or complete. The exacerbation can vary from mild to extreme, lasting from a few days to several weeks. 2 In most of the individuals initially diagnosed with relapsing–remitting MS (RRMS), the condition will eventually lead to the next incremental phase called the secondary progressive phase of MS (SPMS). With or without occasional relapses, SPMS is characterized by a gradual deterioration of the condition and is generally assumed to result in the great degree of neurological impairment. The less common type of MS termed “primary progressive MS” accounts for about 10% of cases and is characterized by a gradual progression of the disease and a reduction in function from the beginning of the disease, with no acute exacerbations or remissions3, 4 in the progressive relapsing category of MS, where a gradual decline in neurological functions coupled with occasional exacerbations and worsening of MS symptoms is observed.
Symptoms of MS
The noticeable symptoms of MS in general include fatigue, imbalance, spasticity, chronic pain, cognitive disability, bladder and bowel dysfunction, impairment of vision and voice, depression, sensory disturbance, and weakened mobility. 5 It is estimated that up to 90% of individuals with MS experience impaired mobility, 75% to 95% experience fatigue, and over 85% experience chronic pain. 6 In most of the cases, high levels of stress, anxiety, and depression are recorded in people with MS, regardless of particular physical complaints. 7 It is seen that the experience and symptoms of each individual going through this ailment are unique and different. Symptoms can range from mild to severe physical and neurologic impairment. 6 There is no known cure for MS and no approved therapy that directly reduces the central nervous system’s damage or facilitates repair. 1
Stress and MS
It is believed that MS is associated with psychological stress. More stress levels may increase the risk of relapses and worsen the symptoms. 8 Several studies have reported a clear association between stress and MS,9, 10 while some other studies 11 contradict with it. The link between stress and MS may be attributed to patterns of patient’s stress, environment, social, psychological, and biological attributes11, 12; however, others failed to find this association or only found a quasi-significant relationship.13, 14 These incongruent results can be explained differentially in study design 15 as well as by the ambiguous way in which stress affects MS.
Comorbidity in MS
The most common comorbid conditions in patients with MS are disorders of the psyche rather than the physical health. 50% and 36% rates for depression and anxiety, respectively, have been reported in MS. Fatigue and pain may be more in MS patients with depression. Psychiatric comorbidities have been associated with disability progression. Anxiety and depression together may increase the risk or severity of various comorbidities, including hypertension, obesity, coronary artery disease, and diabetes, which may then secondarily have negative effects on MS. 16 A systematic review emphasized the fact that comorbidity is common in MS. In established MS cohorts, the most common associated comorbidities are depression (23.7%), anxiety (21.9%), hypertension (18.6%), hyperlipidemia (10.9%), and chronic lung disease (10.0%). However, much of the literature on which these figures are based is on studies conducted in North America and western Europe, and may not be generalizable to the global MS population. Very few well-designed population-based studies have assessed the incidence or prevalence of many autoimmune diseases, cancers, ischemic heart disease, and stroke among patients with MS. 17
Yoga in MS
Yoga, ancient Indian science, is used as an aid for physical, mental health, and, then, to spiritual well-being. Yoga, harmonizes mind–body interaction and comprises physical practices (asanas), breathing techniques (pranayama), and meditation and relaxation techniques. Various studies have demonstrated the benefits of yoga for health and clinical conditions, such as asthma, coronary artery disease, diabetes mellitus, pulmonary tuberculosis, epilepsy, fibromyalgia, and stroke.18–24
Review studies are available on the complimentary effects of yoga for MS.25, 26 The beneficial effects of yoga in patients with MS point to an improvement in body flexibility, balance, gait, and muscular strength, and reduction in anxiety and depression with cognition enhancement.27–29 Other benefits of yoga in MS patients include positive outcomes at physical and psychological aspects, such as the decrease in pain, fatigue, 27 and bladder dysfunction, 30 and improvement in peak expiratory flow, 31 attention, 32 anxiety and depression, 33 and cognition. 34
Need for the Study
Although these results point to the beneficial effects with no serious adverse events, the meta-analysis by Cramer et al 35 concluded that “there is no guideline for yoga as a routine intervention in patients with multiple sclerosis” because of the diversity of the yoga practices used in different studies and also that many of the studies were not methodologically sound. Thus, it is clear that there is a need for a validated yoga module with a holistic approach, which could be used as a standardized technique by researchers before planning a robust randomized controlled trial (RCT) for patients with MS. There are very few studies that have used integrated yoga modules (IYMs) that are meant to correct the disturbances at all five aspects (physical, bioenergy, mental, intellectual, and emotional) of the personality as described in the traditional yoga texts. The yoga practices are personalized depending on several factors, such as age, gender, severity and type of symptoms, and the type and stage of MS. The objective of this study was to check the content validity of an IYM to be introduced to patients with residual symptoms or signs of RRMS during the stable phase of remission of the disease. As these patients will be already stabilized on a standardized and internationally accepted conventional management protocol, the design of the study becomes more robust when we plan to look at the efficacy of the add-on IYM in randomized control studies. Here, we present the content validity of the module, which will go through a feasibility study before implementation in an RCT that has been planned.
Methods
The first step was to develop the module based on the conceptual basis of integrated yoga for health and the second step was the establishment of the expert committee and development of the Google Form. In the third step, we followed the modified Delphi 36 procedure for the validation of the module.
Step 1
In the first step of the development of the IYM, we included a review and compilation of literature from two classical yoga texts,37, 38 three contemporary yoga texts,39–41 and eight scientific publications on the application of yoga in MS. For compiling the scientific literature, some of the search engines that we used were PubMed, Google Scholar, and Medline. The indexing terms used were “yoga,” “multiple sclerosis,” “movement disorders,” “pranayama,” “meditation,” “hatha yoga,” “mindfulness,” and “lifestyle.” After a thorough review of the literature, including books and research papers, we filtered the content, and included experimental studies that used only yoga as therapy for MS,25,26,28,30–34 giving importance to the familiar and particular features described in each study. Based on this literature review, we prepared a preliminary module (IYM) comprising 39 practices.
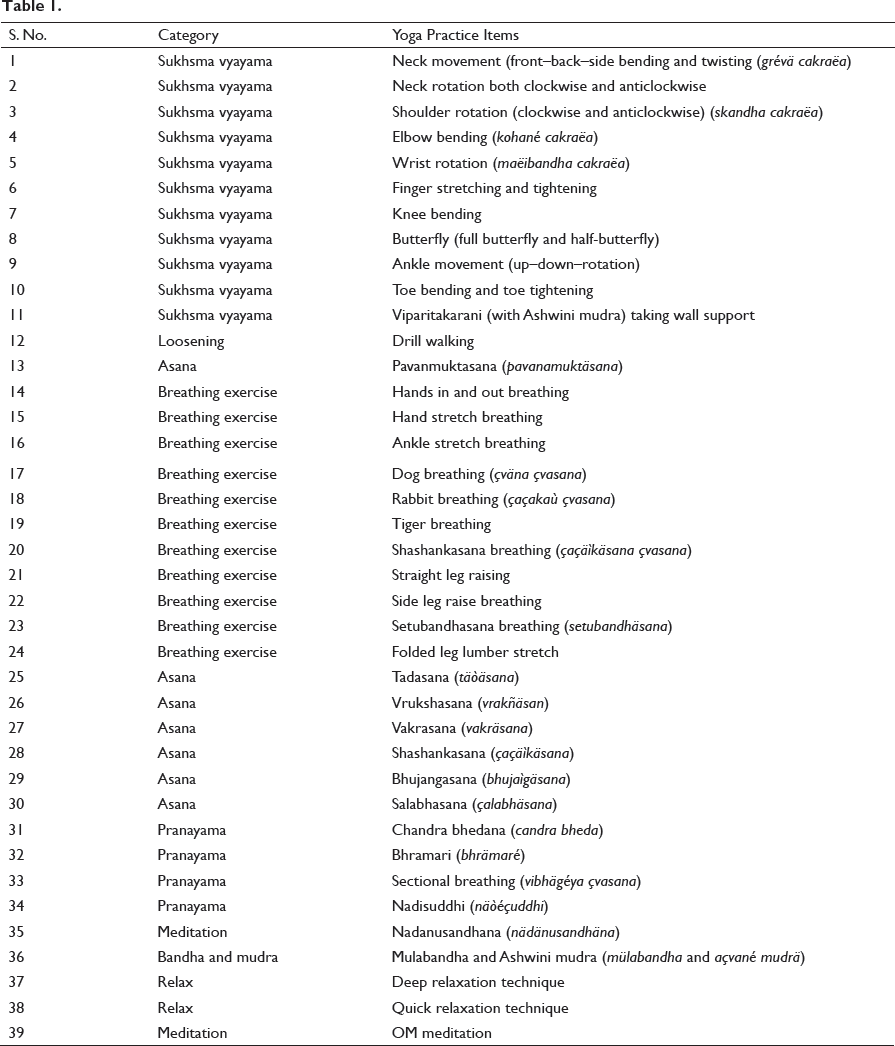
Purpose of IYM
Based on the nature of the disease, it appears that yoga for patients with RRMS has to be planned to offer improvement in a holistic way, not only for its physical and cognitive benefits (flexibility, gait, balance, muscle strength, and cognition)27–29 but mainly for stress management for prevention of progression of the disease 8 and help in better survival with improved quality of life. The module of selected yoga practices submitted for validation to the committee for practice during the scheduled hour included āsana, prānāyāma, relaxation technique, and meditation (Table 1). We also planned to add on aspects of yogic advice for patients and their caregivers using concepts from Bhakti Yoga, Jnana Yoga, and Karma Yoga that cater to a notional correction to accept life. 42 These include discussions on sleep, hygiene, rest, diet, exercise for weight management, daily activities, abstinence from addictive substances, and stress management, all based on yoga.
Contents of IYM for Validation
Step 2. Expert Committee
Figure 1. The Experience of the Expert Members Between 3 and 40 Years with a Median of 10 Years (Inter-Quartile Range: 15.4 Years) and Most of Them had PhD (Yoga) as a Qualification.
Figure depicting Experience of the Experts in Yoga Teaching / Yoga Therapy.
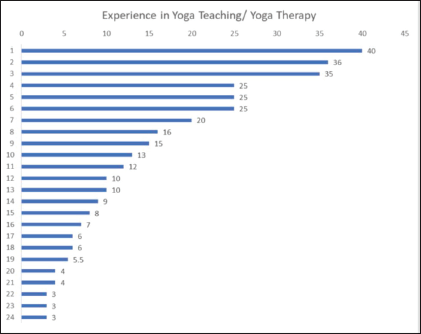
We had approached 24 yoga therapy experts (Figure 1): 17 males and 7 females, and written consent obtained from them to participate in the Delphi rounds online discussion. The experts (internal experts, 5 and external experts, 19) included a neurologist (having postgraduate degree in neurology) with the knowledge of yoga, medical professionals with MBBS degree and PG degree in yoga therapy, medical professionals in alternative systems of medicine with PG degree in yoga therapy, yoga clinicians with MD (yoga therapy) and/or PhD in yoga, and yoga therapists with PG degree and experience in treating neurological patients with a minimum of 3 years of experience as a yoga therapist. Figure 1 shows the experience of experts, ranging from 3 to 40 years.
Step 3: Procedure for Validation by Experts
We prepared the module as a Google Form for obtaining the opinion of the experts online. Following is the link to the Google Form:
In the first Delphi round, we asked the experts to tick on three choices (nonessential, useful but nonessential, and essential) for each item. We asked them to mark the practices that do not contribute in improving any symptoms or patient’s quality of life with MS as “nonessential,” the practices that would help in improving general well-being and stress reduction as “useful but not essential,” and those practices that have a direct effect specifically on MS symptoms as “essential.” At the bottom of the form, we provided a box for their comments and suggestions for any add-on practices.
After receiving the answers from all experts, we modified the list of practices after incorporating all changes and sent to all experts before planning the second round Delphi interactive session on teleconference mode. During this final interactive session, all the experts gave their consensus to include the essential aspect of advice for a healthy lifestyle using yogic concepts, which were not put up in the Google Form for scoring. Compilation of all inputs and the statistical analysis led to the final module of IYM for RRMS patients during remission.
Statistical Analysis
We computed the content validity ratio (CVR) from the total scale based on the feedback given by the experts. As per Lawshe’s formula, if more than 50% of the experts indicate that an item is essential, then that item is considered to have good content validity.48 According to Lawshe’s formula, CVR = (Ne − N/2)/(N/2), where Ne is the total number of experts indicating “essential” for each item and N is the total number of experts (Table 2).
From our sample of 24 experts, we have arrived the CVR for our yoga module as ≥ 0.42, which was considered satisfactory. The mean CVR for the items indicates the overall test of content validity. Internal consistency of the responses of experts was analyzed through Cronbach’s α.
Result
Flowchart for the Development of a Yoga Module
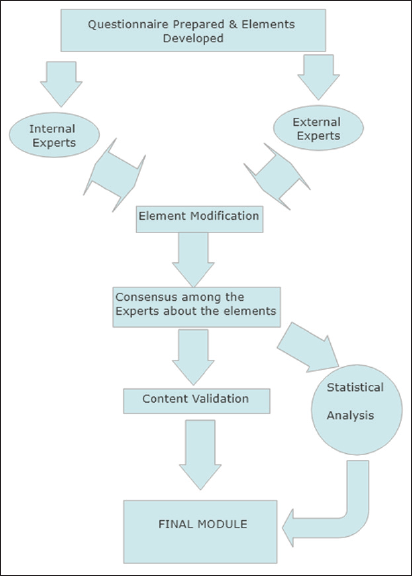
Figure 2 gives the details of the flowchart providing the steps for the development of the yoga module.
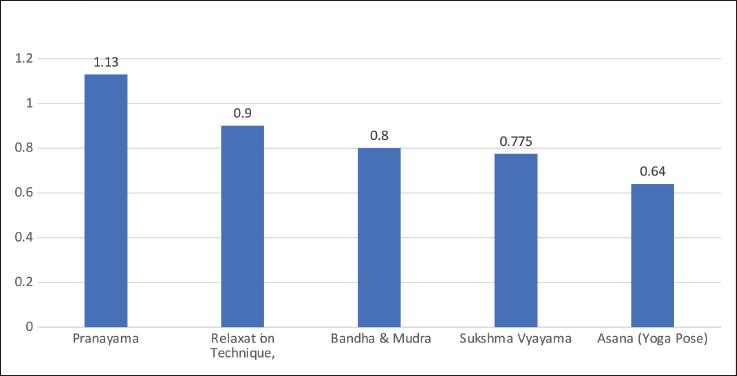
Depicts the average CVR values in different elements of the yoga practices, which are part of the development of the yoga module.
Content Validity Ratio (CVR) calculation
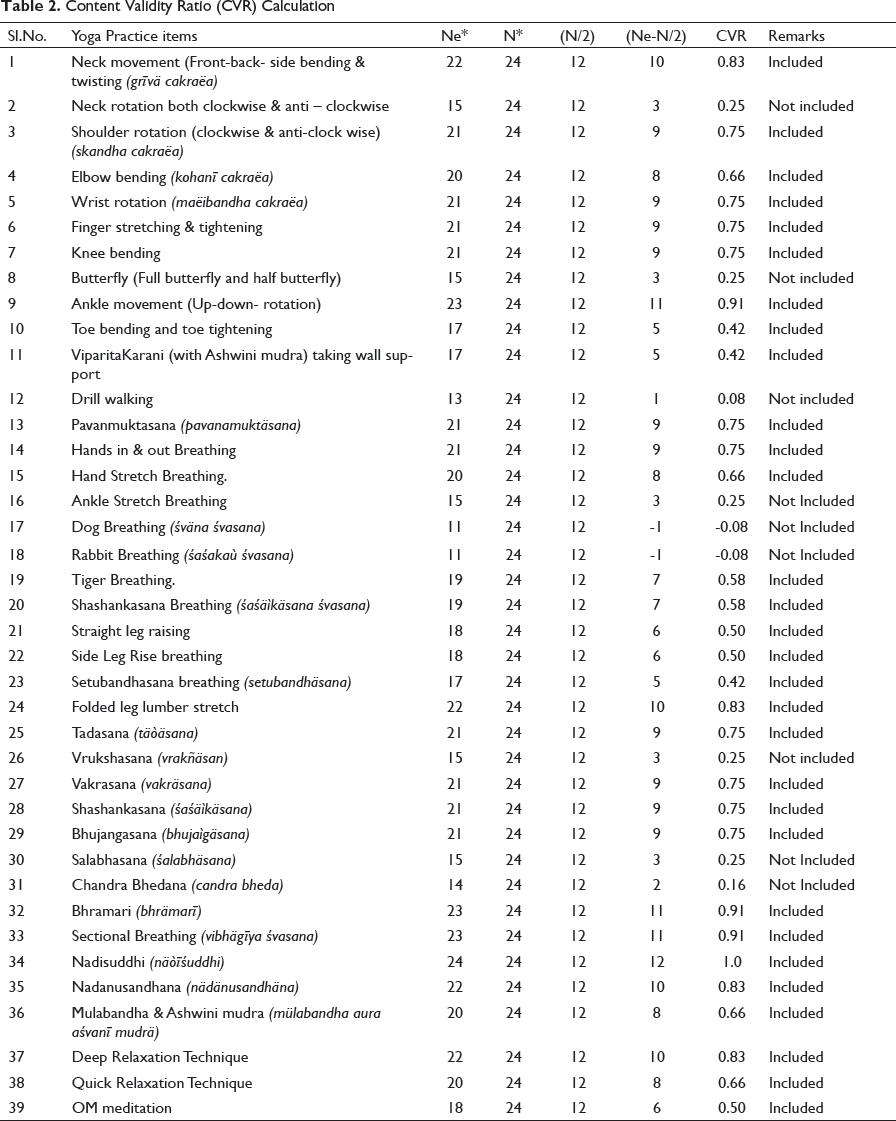
Out of 39 practices, 30 practices had a CVR ratio ≥ 0.42, which indicated high content validity in the above Table 2. All the practices (applicable cases as per Table 2) can also be practiced by adopting a sitting position in a chair under the supervision of a trained yoga professional. Overall CVR of all practices is 0.69.
Discussion
The present study was planned for the development of an add-on yoga module for patients with RRMS to be used during remission. We preferred loosening practices, asanas, breathing practices, few postures, relaxation and meditation appropriated from classical yoga texts, and previous research findings. Twenty-four qualified experts, who fulfilled the study criteria, validated this module. Of the 39 practices subjected to validation, 30 had a CVR score of ≥ 0.42 and were included in the final validated yoga module.
Three steps involved here are: (a) development of the yoga module for MS, (b) expert validation using Delphi rounds, and (c) analysis of CVR. In the first step, the IYM was compiled based on the literature review of traditional textual references and recent research publications. However, recent Hatha Yoga texts43, 44 have increasingly emphasized the use of different yogic practices for improving health. The second step included two Delphi rounds for validation of the items on a three-point scale followed by an interactive “online” session. The third step was the analysis of CVR.
Of these, 30 practices (CVR ≥ 0.42) were included in the validated yoga module (Table 2). The remaining nine practices (CVR < 0.42), namely neck rotation (0.3), butterfly (0.3), drill walking (0.1), ankle stretch breathing (0.3), dog breathing (svana svasana – 0.1), rabbit breathing (sasakah svasana – 0.1), vraksasana (0.3), salabhasana (0.3), and chandrabheda pranayama (0.2), were opined as “not essential.” As these practices were slightly challenging for patients with MS, most experts did not consider them as “essential” for MS therapy. Thus, the final CVR satisfied the minimum value, as per Lawshe’s CVR formulae. Also, the intraclass coefficient for all yoga practices was found to be 0.7, concluding that the overall opinion of all the 24 experts for the recommendation of the practices for IYM was in unison.
Similar to any other exercise protocol, an optimal yoga module consists of modes (types), frequencies, intensities, durations, and progression. Determining the appropriate mode depends upon patient preference and safety issues associated with the stage of MS or other conditions. The frequency, intensity, and duration are specific to the type of practice (activity) and should be customized according to the patient’s ability to safely perform the practice (activity). The loosening practices (Sukshma vyayama) included in this module helped in loosening the joints and reducing the stiffness or spasticity, which consequently helps in easy mobility. All relaxation techniques help in reducing stress and anxiety by calming down the mind.
In the proposed IYM practices (as per Table 2), emphasis is on loosening exercises (Sukshma vyayama), breathing practices (Pranayama), asanas, mudras, relaxation, and meditation. Also, interactive lectures on scriptural concepts of a healthy lifestyle with regular timely bowel movements, sleep, wholesome vegetarian diet, and stress management through Jnana Yoga, Bhakti Yoga, and Karma Yoga contributed to the integrative approach. Comparing the practices developed in this article with those of the practices from another study, 45 common practices in both of them are Viparitakarani with wall support, Tadasana, Vrukshasana (vrakñäsan), and relaxation technique. We omitted nine practices in the IYM because of their CVR values being less than 0.42 from the previous Table 2. Figure 3 depicts the average CVR values in different elements of the yoga practices, which are part of the development of the yoga module.
The Conceptual Basis of IYM
The Swami Vivekananda Yoga Anusandhana Samsthana (S-VYASA)—Integrated Approach to Yoga Therapy (IAYT), developed and used in earlier studies, is based on the Pancha Kosha 46 principle. IAYT emphasizes the application of a judicious blend of yoga practices at the physical, vital energy (Prana), mental, emotional, and intellectual levels as therapeutic practices. 47 It slows down (definition of yoga in Yoga Vasistha) the wreathe of the uncontrolled speed of the rewinding thoughts during the negative violent surges of emotional responses to the chronic demanding situations (physical, social, and psychological) these patients go through. All yoga techniques help in offering deep relaxation/rest at the body level, calm down the mind, and correct the imbalances. The concept recommended in the traditional texts, such as “successive stimulations followed by progressive relaxation” and “mastery over the modifications of the mind” (definition of yoga by Patanjali) and harmonize the disruptions at each of the five levels (definition of yoga in Bhagavad Gita), is the basis of IYM.
Five aspects of personality (Pancha Kosha and the practices).
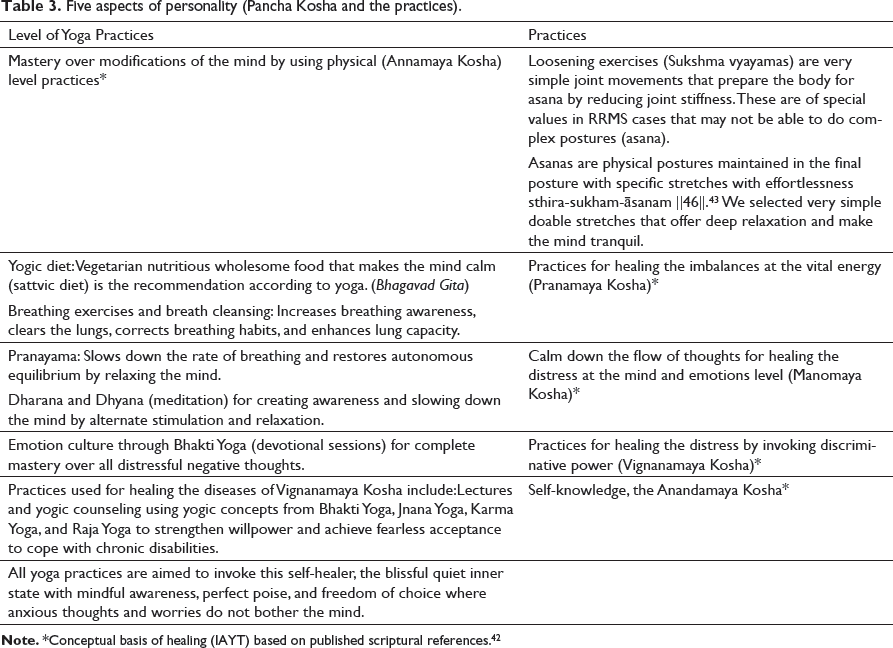
When compared to the practices from other studies (refer to the supplementary information), as stress is the cause for MS, an intervention focusing on the mind through Prana is more appropriate. The supplementary information provides the pictures of the IYM practices and the frequency to be adopted by the subject depending exclusively on the age, ability, prevailing health condition, and the advice of the neurophysician, under the guidance of a trained yoga teacher.
Limitations of the Study
This module is an attempt to develop content validity by obtaining the opinion of experts who have been working with patients suffering from MS. Its feasibility and reliability studies are necessary to establish its acceptability and safety.
Conclusion
The yoga module developed for RRMS has good acceptable range of content validity. Future studies must determine the feasibility through pilot studies and the efficacy of the IYM with larger samples for longer periods to establish scientific credibility of the module, which is being planned. There is a need to develop such modules for patients during their exacerbations and for more rapidly progressive type of MS.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Content Validity of an Integrated Yoga Module for Practice During Remission in Relapsing–Remitting Multiple Sclerosis Patients by Sreedhar Palukuru, Suchitra S. Patil, R. Nagarathna, Amit Singh and K. S. Nibedita, in Annals of Neurosciences
Footnotes
Acknowledgment
The author acknowledges the contribution of all the experts and thanks to each one of them for their valuable feedback for the IYM and the others for their comments on the preliminary versions of this manuscript.
Ethical Statement
Ethical clearance was obtained by the Ethics Committee of S-VYASA, Bangalore.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.