
Abstract
Sam Jones joined as the learning and development manager at Fortis Healthcare Limited in August, 2014. He finds himself in a bind when he observes that the people systems were lagging and unable to cope with the rapid organizational growth; affecting the delivery of service. Substantial setback was the ambiguity of training modules creating a hurdle for service excellence. Processes were vague and complex with duplication in training modules. Forty-two training modules were there across all units but being used with different names in different units, some of which had overlapping content under different module names leading to underutilization of time, money and human resources and lacking optimization. This particular case addresses the need of managing organizational change to restructure service excellence training. The case exposes the readers to the dilemma about how to implement the change process, how to convince the employees about the change that is required and in which direction to start with?
Introduction
In August 2014, Sam Jones joined as the learning and development manager at Fortis Healthcare Limited. The organization, after witnessing a phenomenal growth phase in the previous decade, which included acquisitions of several hospitals, wanted to progress to the integration and consolidation phase through service excellence. Although Fortis intended to be patient-centric, but due to the rapid growth, the people systems were lagging, affecting the delivery of service. The presence of multiple hospital units spread across various geographical locations, both national and international, and the complexity of services, added to the existing challenge of developing a standardized Fortis training curriculum to enhance service excellence in the organization. Fortis had always led the transformation in the healthcare industry by providing the most efficient medical equipment, infrastructure and medical talent to address the unmet needs of the country in the tertiary and quaternary healthcare segment. Considering the industry’s growth potential, the organization had positioned itself as a world-class healthcare provider committed to clinical excellence and compassionate patient care to deliver the most beneficial healthcare experience and outcomes. But, top leadership was then worried about the future of the organization, considering the geographical spread of it and the need for integration of processes across all units for a standardized delivery of service. They sensed a lack of integration and standardization amidst the processes of the organization. Customers seeking healthcare facilities may be satisfied or dissatisfied, depending on the kind of services evaluated on the basis of different hospital services, like attitude of doctors, promptness of service delivery, time spent advising, etc. (Kashif et. al., 2014). Hence, a proper integration of training modules is required to offer a standard with respect to the quality and customized with respect to the situation of services.
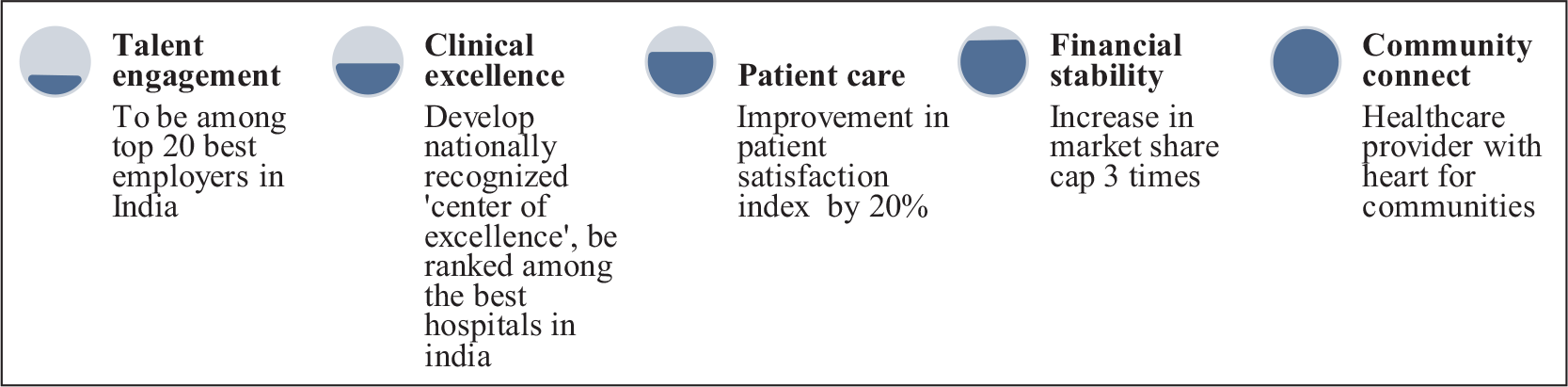
The top leadership team, before the joining of Jones, also realized the need to transform Fortis and proposed a 3-year strategy to be implemented from the second half of 2013. The 3-year business strategy, referred to as the ‘Lakshya’ (refer to Figure 1), emphasized the need to stop being just financially-oriented. The new approach focused equally on the other four pillars, namely clinical excellence, patient care, talent engagement and community connect programme, comprising five pillars of excellence overall.
Company and Industry Background
The Fortis Journey
Fortis Healthcare Limited is a leading, integrated healthcare delivery service provider, headquartered in India. It was established in 1996 with a vision to be a globally respected healthcare organization known for clinical excellence and distinctive patient care. Fortis Healthcare is the country’s fastest-growing healthcare group. The company operates its healthcare delivery, primarily in three different verticals, comprising hospitals, diagnostics and daycare specialty facilities in India and abroad. It has 36 healthcare facilities (refer to Table 1), located in four zones in India, for example, North, South, East and West, apart from operating in Dubai and Sri Lanka. It has most units in Delhi in the North zone apart from facilities in other zones in India, with 9,000 potential beds for admission of patients for treatment and observation across all units and 415 diagnostic centres (Fortis Healthcare Limited, 2020). Fortis healthcare facilities include multispecialty hospitals and super-specialty centres that provide comprehensive tertiary and quaternary healthcare, which are advanced levels of medicinal care, highly specialized and offered seldom by general healthcare providers. It has about 31 specialties, such as gastroenterology and hepatology sciences, neurology, plastic and reconstructive surgery, etc., and operates one of the most significant cardiac sciences, orthopedics and oncology programmes in India.
Fortis Hospital Units Spread Across India
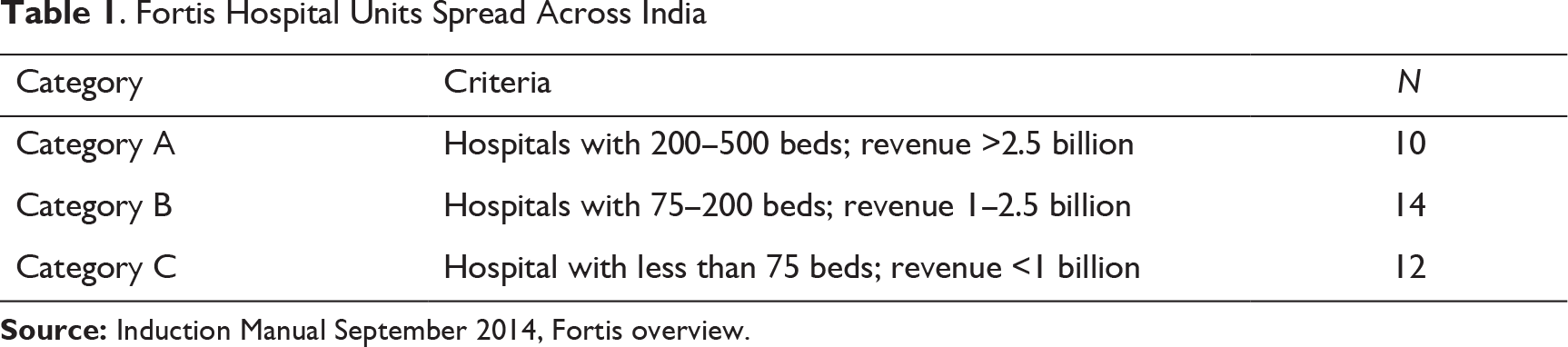
Fortis proliferated in India through acquisitions, greenfields, brownfields and management contracts, setting a fast pace for itself with the acquisitions of many hospitals in the previous decade. Malaysia’s IHH Healthcare Berhad has become the controlling shareholder of Fortis Healthcare Ltd by acquiring a 31.1 per cent stake in the company in November 2018 with ₹40 billion. 1 From a single hospital in 2001, Fortis healthcare has emerged as one of the largest organized healthcare delivery organizations in the country with an audited consolidated revenue from operations of ₹44.69 billion for the FY 2018–2019, and more than 15,000 employees. Fortis is still in the consolidation phase to exploit the existing resources and improve its operational efficiency. The organization focuses on providing value to all its patients; in other words, it provides the most efficient clinical solution with compassionate patient care (FHL Annual Report, 2018–2019). 2
Healthcare Industry: Where Does India Stand?
Healthcare services comprise hospitals—both government and private—medical tourism, medical devices and equipment, outsourced medical services, clinical trials, telemedicine and health insurance. In the past decade, it has become one of the contributors to India’s growing economy, in terms of revenue and employment. The Indian healthcare sector already constitutes 65 per cent of the overall market. It is growing at a rapid pace due to its expanding services, including the highly specialized treatments and increasing investments in this area by public and private players. The healthcare market can increase threefold to ₹8.6 trillion, by 2022, foresees India Brand Equity Foundation (IBEF), established by the Department of Commerce, Ministry of Commerce and Industry, Government of India (GoI) (India Brand Equity Foundation [IBEF], 2018). World’s most massive government-funded healthcare scheme, Ayushman Bharat, was launched by the Indian government on 23 September 2018, confirming the policy support of the government in this sector as shared by IBEF.
Medical tourism is another sector where Fortis is a big player among some other private healthcare facilities. Indian medical tourism market is growing at the rate of 18 per cent year on year and is expected to reach US$9 billion by 2020. It is commonly referred to as the traveling of people to another country with the purpose of obtaining medical treatment. India, a well-educated, English-speaking nation that offers quality private hospitals and medical facilities at a relatively lower cost, is a cost-effective proposition (Onicra Credit Rating Agency of India Limited, 2019). It is noteworthy to mention that considering the generous increased spending on the healthcare sector by the GoI as a percentage of GDP, it has a promising future.
Nonetheless, the expectations of the people are increasing and preferences are changing with respect to the services provided by the healthcare facilities, thereby increasing complexity and competition. The government’s expenditure on the health sector has grown from 1.2 per cent in 2014 to 1.4 per cent in 2018. The GoI has plans to increase public health spending to 2.5 per cent of the country’s GDP by 2025. The public healthcare system comprises limited secondary and tertiary healthcare centres and mostly concentrates its spending on providing primary health services in rural areas. The private healthcare sector offers the majority of secondary, tertiary and quaternary care, based primarily in metropolises or Tier I and II cities (IBEF, 2018). People also are now more aware of the advantages of health insurance; direct premium income underwritten by health insurance grew to ₹248.6401 billion in the financial year 2020 and up by 18.2 per cent from 2019. 3
Factors like a large and growing population of approximately 1.3 billion, growing at the rate of 17.6 per cent in the 2001–2011 decade (Table 1 of Provisional Population Tables: India; Census, 2011), 4 and a booming economy of US$1.72 trillion, have enabled the sector to grow at a considerably higher rate (Frost & Sullivan, 2020). Apart from these, rapid urbanization, which has expanded the middle class, and an increase in lifestyle diseases and awareness levels among mass are also responsible for the healthcare sector growth.
All said, the healthcare sector presently has challenges concerning infrastructure, availability of adequate investment and skilled staff. India initiated its health reform journey in the previous decade and required momentum to overcome the difficulties. The continual increase in diseases on a large scale, evolving population demands rapid changes (Chahal et al., 2016; Chatterjee, 2014; Gudwani et al., 2012; Kashif et al., 2014). The government is critical in this transformational journey, supported by the private players.
Challenges Faced by Fortis: A Brief
Building a sustainable patient-centric organization was imperative and, therefore, Jones had the choice to either quickly address the training need by employing an expert third-party training organization or build internal capabilities and restructure and standardize the service excellence trainings. Besides, Jones had to understand how to regulate without impinging on unit autonomy, which the perceived notion was of the respective units, and also enhancing the quality of content and delivery. Changes in the organizational environment have also generated never-ending competitive pressures on the organization to continuously redesign itself for commercial creativity, in order to survive and prosper (Chatterjee, 2014). In addition, the challenges due to globalization, privatization and liberalization, increased competition and technological advances have forced the management to introduce novel and innovative human resources (HR) and other management practices (Chahal et al., 2016).
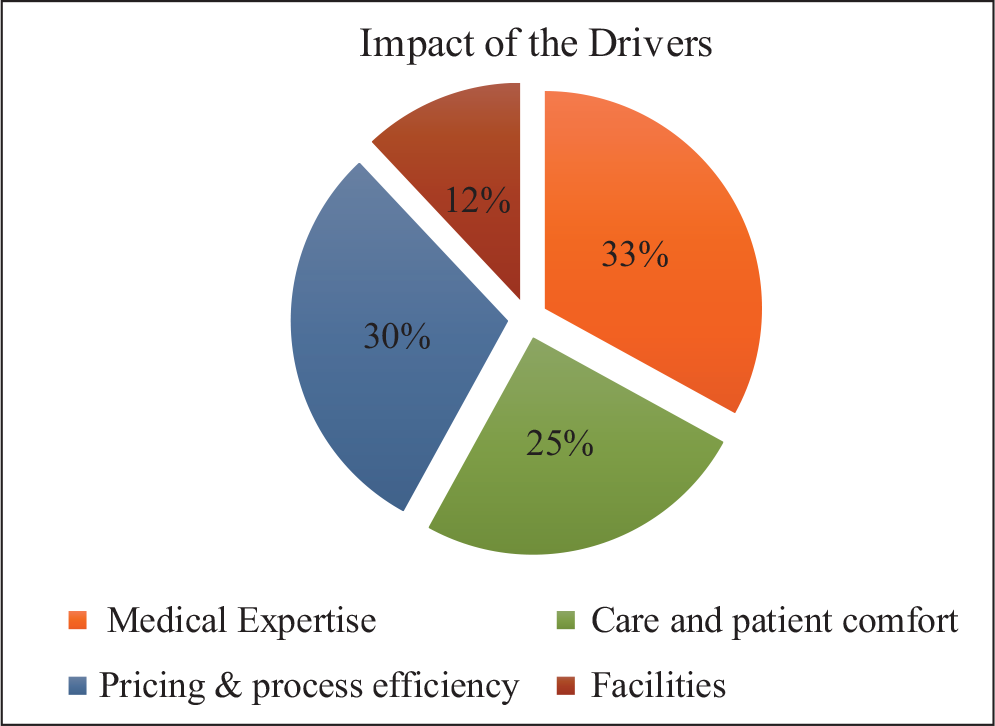
To assess the current status of each of the four pillars of the ‘Lakshya’ strategy, external industry-based survey and feedback tools were leveraged. In addition, establishing various lead indicators and process parameters to assess the progress were used. Several customer responses were collected, and surveys were conducted by Fortis management, which strongly suggested the need to strengthen patient care (25%), one of the key three pillars of ‘Lakshya’ (refer to Figure 2). In Figure 2, the pie chart shows the impact of the drivers on the overall patient experience. A profound observation by Jones revealed that service excellence was identified as a differentiating factor. Although improvement in processes and systems were being initiated to deliver efficient patient care, no systematic service training was being conducted to enhance employee capabilities for delivering superior patient care. The training organization was divided into two regions with little or no coordination among the entities. When Jones contacted the various hospital units to understand the status of the service excellence aspect of training, the lack of focus on training activities was apparent. Sporadic attempts in the past had been made to provide training in the domains of patient care and customer service. Most of the attempts were on a case-to-case basis or delivered in an ad-hoc manner. Finally, an effort was made in early 2014 to standardize the existing modules. For example, all hospital unit trainers were called at a location by the training managers for 2 days, which proved to be an insufficient amount of time to discuss and agree on the training programmes. In addition, earlier in the second half of 2013, a review session highlighted that numerous versions of training content were in circulation in each of the hospital units; no perceptible binding force centrally or otherwise existed to take the training agenda forward in a systematic and structured manner. The business did not have an integrated learning organization and no management information system (MIS) on training since April 2012.
In a nutshell, the main challenges faced by Fortis Healthcare Limited in 2014 were a comprehensive integration of the processes of the organization, training and engagement plan to help incorporate smooth and homogenous training, utilization and optimization of the resources to the best of their capacity. The different heads which needed attention were (a) need for evolving training, HR strategy and structure, (b) overlapping and ambiguous training content and design, (c) implementation of a uniform and standardized curriculum across Fortis units, (d) conflicting job roles, (e) trainer capabilities and resources and (f) working in virtual teams.
Challenges Faced by Fortis: Elaborated
Need for Evolving Training and Human Resource Strategy and Structure
Unit Trainer Key Result Areas (KRA)
Overlapping and Ambiguous Training Content and Design
Most of the training modules were based on PowerPoint presentations, with no facilitator guide; the objectives, or specific flow of the programme, were not clearly articulated. Some of the modules were being used with different names in different units, whereas some of the content were duplicated from or reused in various modules. The modules were not standardized, and no uniformity prevailed concerning One Fortis. Since all the units worked independently and in silos, bringing everyone on a uniform platform was a challenge. In other words, a review of the existing training for service excellence highlighted that the modules were not structured, and each unit was autonomous, and that the training content or delivery was not standardized, structured or uniform.
Moreover, the unit trainers had no symbiotic relationships. Getting a core team to work on improving the service training culture was a challenge. In addition to the problems of functioning, the top leadership and many major stakeholders regarded training as having no credibility, giving less importance to a proper training module, which multiplied the adverse impacts on service behaviours. A total of 42 training modules were there across all units but being used with different names in different units, some of which had overlapping content under different module names. In contrast, few others had different content with the same module name. This overlapping of material was of concern because it hindered the optimization of the resources (financial and HR) and was redundant for some trainees, who already had that training under a different module name. Similarly, the same module name but different content across units was no less ambiguous. Trainees expected training in some particular areas, but, due to the ambiguity in training module name, got trained in something else, which was not even relevant to his/her area of expertise and fail to add any value to the service.
Implementation of a Uniform and Standardized Curriculum Across Fortis Units
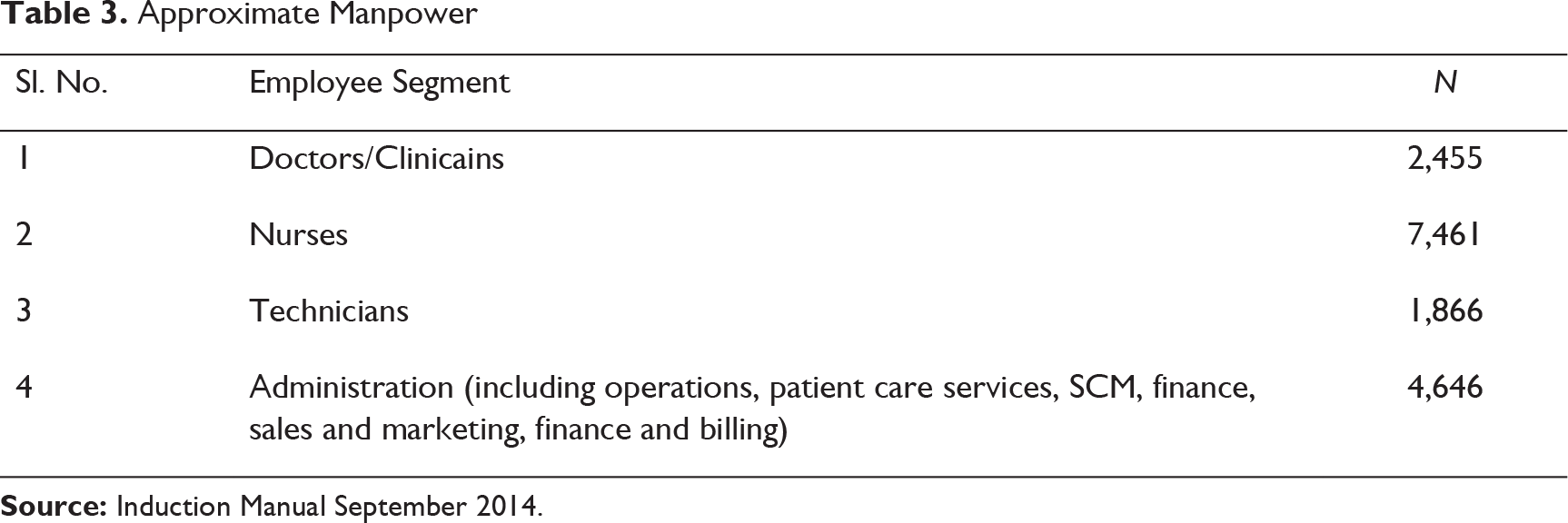
Approximate Manpower
Conflicting Job Roles
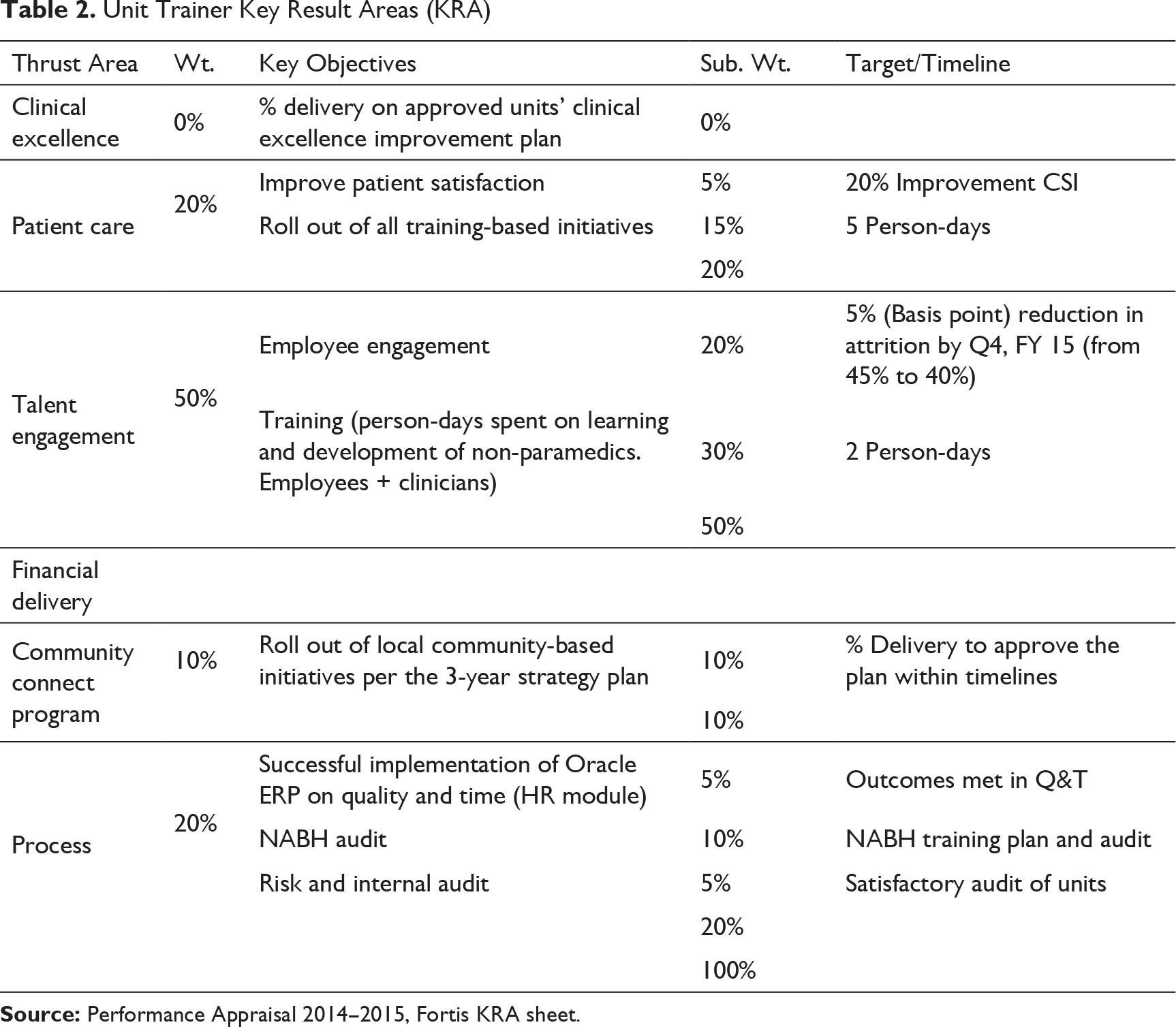
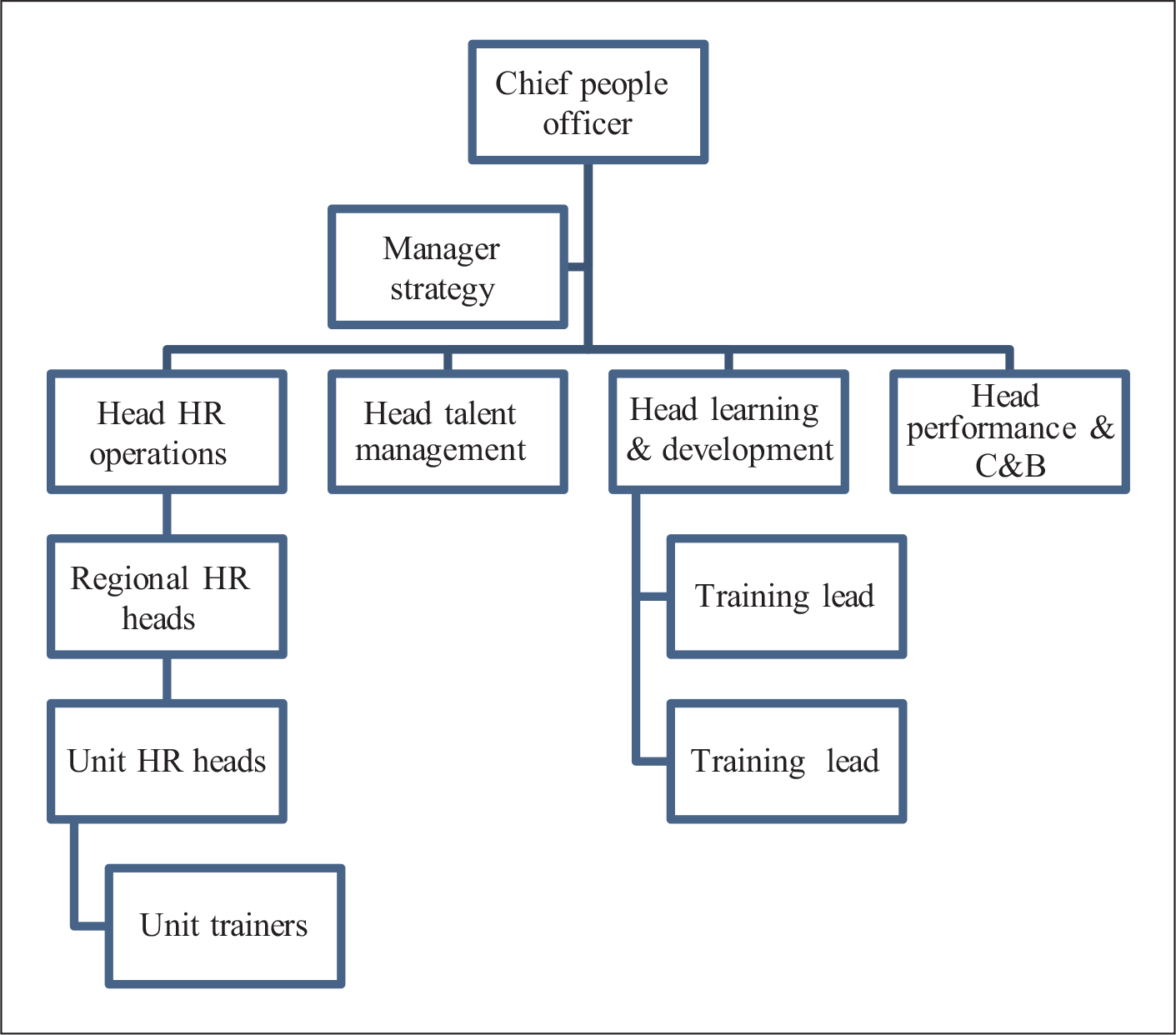
The unit trainers reported to the unit HR (refer to Figure 3). The lack of focus on training was reflected in the annual goal-setting—KRA sheets of the unit trainers (refer to Table 2). As the emphasis on training continually decreased, the unit trainers were drawn into various HR engagement initiatives to optimize the resources. However, in doing so, the organization lost its focus in training that was still existing. Since the unit trainers possessed adequate public speaking ability and interpersonal skills, they were made to participate in many HR events. Their responsibilities included approximately 50 per cent of training and 50 per cent of other HR activities (refer to Table 2). The non-training activities, very clearly specified in the KRA sheets, included employee engagement (20%), National Accreditation Board for Hospitals and Healthcare Providers (NABH), risk audits (20%), etc., and initiatives in the community connect programme (10%). An analysis of the KRA sheets revealed that only 50 per cent of weightage is attributed to the ‘specialist trainer role’. These conflicting responsibilities required attention and time to identify needs, conceptualize programmes and facilitate programmes after gap analysis. During most of 2014, the role of unit trainers shifted from being purely a training specialist to a more of an HR generalist role.
Trainer Capabilities and Resources
The unit managers shifted their priority gradually from the training of human resources in various functional departments to general HR functions. Most of the teams, specialized in imparting training skills, were leveraged for other HR activities, usually for engagement and fun at work events; this was a logical progression because of the teams’ ability to communicate effectively. At least 50 per cent of the time was spent in non-training activities. With no structured expectations on training or functional inputs provided to the trainers, their ability to deliver and facilitate programmes became secondary. The recruitment drives to replace those trainers who had left the organization were leaning more towards incumbents with a general HR background than those with a training background. Most of them were doubling up as HR managers instead of being actively engaged in the design and delivery of training. The skill of designing was a specific development area but was given the least attention. In terms of training delivery, most of the trainers were proficient in lecture-based delivery only, and learning by doing was almost absent in the training modules.
MIS or report and review of the training conducted was practically never provided to the senior management team. Learning and development dashboards had not been created or reported since April 2012. This indicated that the lack of leadership and training was not discussed as a business agenda during leadership reviews. Training had become extremely isolated in its working, and the lack of communication on training agenda by unit trainers and training managers added to its isolation from the stakeholders. Even the HR heads and functional heads at hospital units neither focused on training agenda nor placed any demands or requirements towards enhancing capabilities of employees through structured training initiatives. Moreover, the business was struggling with the challenge of resource availability and, therefore, releasing the employees for training purposes was difficult. In addition, training was viewed as an HR agenda rather than business agenda by the organization.
Working in Virtual Teams
Another issue that was observed by Jones in the organization was the lack of capability or willingness to work and manage teams virtually. The world was moving towards an Information Technology (IT)-enabled collaborative teamwork. Still, Jones witnessed that the employees of Fortis Healthcare were usually comfortable interacting in person with each other and only within their respective hospitals. Fortis did not have a culture of working in or managing virtual teams, and all the trainers were located in their respective units. Since they reported to their respective HR heads and facility directors, the need to collaborate or exchange ideas across units was scarce. To create a One Fortis service excellence training curriculum (i.e., to influence or have different units work together on a common agenda) was a challenge.
Future Plan of Action Focused on Pillars of Service Excellence
In 2014, Fortis conducted several brand and customer feedback surveys that indicated the need for providing superior patient care to the patients and emotional support to their family members, where Fortis lacked the training to the frontline employees. Besides, medical expertise and clinical solutions could not be neglected at any cost. An overhauling of service excellence was the need of the hour to stay in the competition. The organization felt the need to focus on standardized services and grooming within the organization, which was very irregular until 2013. In 2013, the senior management team proposed a 3-year strategy and planned to implement them gradually from 2014, which emphasized the need to focus on pillars of standardized training on talent engagement, clinical excellence, patient care, community connect programmes and financial stability. In the subsequent months, detailed plans were developed for each of these areas and incorporated into the respective KRA (refer to Table 2) sheets by June 2014. Still, the 3-year strategy became the focus only after November 2014, due to the lack of proper process and communication across levels, explaining the why and how of this strategy change. Jones could feel that an undercurrent of resistance was flowing, which could take a bad shape suddenly and jeopardize the plan of change.
Management Dilemma
Jones had to select an approach to restructure, standardize and enhance the quality of the service excellence training curriculum. Implementation of the process of change concerned how to convince employees ‘why’ the change is required and reduce resistance. The change would be a humongous task, given the size and complexity of the organization and its services. Jones was confused about how to implement the change process and in which direction to start with? Will any particular model help bring about the change? Another dilemma that concerned Jones was how to stimulate the employees to chase the new goals? Some action strategies had to be followed to carry out the changes smoothly and effectively and, most importantly, as early as possible. The new strategy would be effective from 2015 and is expected to be entirely implemented by 2018. Jones was apprehensive if the strategy would work as planned.
Footnotes
Acknowledgement
The authors are grateful to the anonymous referees of the journal for their extremely useful suggestions to improve the quality of the article. The usual disclaimers apply.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.