
Abstract
The increasing pace of healthcare transformation places emphasis on how to enact it. However, there is a difference between healthcare commentators and policymakers regarding preferred change management practice; policy guidance is rooted in diagnostic practices, whereas commentators suggest that dialogic is a more appropriate practice for ensuring success. What is missing from this debate is evidence to inform whether commentators’ suggestions will increase the likelihood of successful transformation outcomes. This study presents a systematic review of change management practices and outcomes, identifying 10 papers that report on 292 cases of transformation. It finds broad support that dialogic increases the likelihood of successful transformation, providing supporting evidence for updating healthcare policy and practice.
1. Introduction
Healthcare is facing exponential growth in the range and complexity of patient conditions and treatment procedures, at the same time as strained finances and a global shortage of healthcare professionals (Jazieh and Kozlakidis, 2020; World Health Organization, 2022). The ability of healthcare organisations to adapt to these challenges is critical to the efficiency and quality of future service delivery (see Figueroa et al., 2019). Transformation, defined as marked changes in the nature of organising (as per French et al., 2005), is one available remedy, for instance by shifting cultures, adopting new technologies, or transitioning to better working models. However, when it comes to transformation in healthcare, the industry is seen to have an ‘implementation problem’ because achieving success, meaning that desired outcomes are realised, has become difficult (see Braithwaite et al., 2020; Grol and Wensing, 2020). Illustrating this challenge, Braithwaite et al.’s (2006) study of transformation programmes across 20 teaching hospitals found that these efforts resulted in little to no improvement in targeted quality and safety outcomes. With this context, the purpose of this review is to explore the question: how to enact successful transformation in healthcare?
Most Western health jurisdictions have established policy agencies tasked with developing and displaying guidance on a preferred change management practice for enacting transformation (Smith et al., 2012). Organisational change scholarship has been a traditional source of this guidance (see Harrison et al., 2021; National Health Service, 2022) yet, specifically in healthcare, there is a clear difference between commentators and policymakers regarding the type of practice that healthcare practitioners should employ (see Bevan and Fairman, 2014; Braithwaite et al., 2018; Dendere et al., 2021; Resnicow and Page, 2008). While there are many popular models and frameworks available, organisational change defines two overarching practices. One is a diagnostic practice (hereafter diagnostic), referring to ‘plan then do’ approaches, where leaders establish goals, develop plans and manage action top-down (i.e. Kotter, 1995; Stouten et al., 2018). Another is the dialogic practice (hereafter dialogic), which is a heterarchical collaboration between those involved, with emphasis placed on ‘learning as we go’ and the bottom-up emergence of new ideas and possibilities (i.e. Bushe and Marshak, 2015; Plowman et al., 2007). In healthcare, policymakers provide guidance based on diagnostic, whereas commentators suggest that dialogic is more likely to lead to success and thus better suited to the transformation that modern healthcare organisations must undertake. Guidance on diagnostic has been widely accepted by practitioners, with a recent review of 38 studies of healthcare transformation identifying that this top-down ‘plan then do’ practice is commonplace (see Harrison et al., 2021).
Given the evidence-based mind-set of healthcare policy, one omission from commentators’ calls for dialogic is evidence to inform the central tenet of their proposal, that dialogic is more suited to enabling success. Looking to the field of organisational change, evidence is light when it comes to examining the efficacy of these practices for enacting success (see Barends et al., 2014; Oreg and Berson, 2019; Stouten et al., 2018). Instead, as Stouten et al. (2018: 778) note, the ‘empirical literature tends to test fairly small segments of broader change phenomena’, such as leader behaviours or specific organisational conditions (for examples of such reviews, see Castiglione and Lavoie-Tremblay, 2021; O’Donovan et al., 2021; Wensing et al., 2006). The lack of data testing the efficacy of these two practices seems an oversight, especially given that the relevance of theory to practice is a prominent dimension of a theoretical contribution (as per Corley and Gioia, 2011).
The purpose of this review is to explore how diagnostic and dialogic influence successful transformation and thus provide evidence that can either support or deny commentators’ calls for dialogic. This specific interest regards to how these two practices enact transformation as it relates to organising, which differs with clinical transformation, relating to updating types and models of care and thus beyond the scope of this review. This review follows Aromataris and Munn (2020) in applying the Joanna Briggs Institute (JBI) process for qualitative systematic reviews, searching globally for studies of transformation across all industries that explore change management practices and their resulting influence on outcomes.
Identifying 10 papers that report on 292 cases of transformation, this review finds broad and consistent evidence that dialogic is associated with a far higher likelihood of success than diagnostic. However, it also finds that commentators’ calls for a pivot from diagnostic to dialogic need not be the case, instead the two practices can be co-applied. Furthermore, this review also identifies common leadership capabilities which were allied with successful application of dialogic. Together, these findings provide a broad evidence base supporting wider use of dialogic in healthcare.
2. Method
The design of this review is guided by three factors. First, since qualitative analysis is the commonly utilised approach for research into organisational transformation (see Oreg and Berson, 2019), this study follows the JBI taxonomy for qualitative evidence synthesis, a process that has previously been used for synthesising evidence to inform healthcare policy as well as reviewing findings on the theme of healthcare transformation (see Jantzen et al., 2017; Pearson et al., 2007). Second, it searches as wide as possible, across both healthcare and non-healthcare contexts, with the view to establish a robust evidence base. This broad selection is undertaken because the purpose of this review is to test the relative efficacy of these two practices regarding success, rather than testing the applicability of these practices in healthcare settings because such a link has already been established (see Bevan and Fairman, 2014; Bushe and Marshak, 2015; Gilpin-Jackson, 2013; National Health Service, 2022). Third, this review selects studies that explore multiple (N > 1) cases of transformation. This is because the single case literature is characterised by both a bias for publishing positive cases (see Oreg and Berson, 2019) and inconsistent replication of constructs between cases (as per Barends et al., 2014), making it difficult to advance the purpose of this review. Thus, the present review focusses on qualitative studies that compare change management practices and outcomes, between multiple cases, and across organisational change and healthcare transformation literature.
2.1. Search strategy
The data bases PsycINFO and Scopus were selected because of their respective coverage of organisational change and healthcare literature, and Google Scholar was also searched because of its wide indexing coverage. Database searches focused on the titles, abstracts and index terms, using the terms: transformation processes, organisational transformation, healthcare transformation, healthcare system transformation – also substituting change for transformation and using English spelling (i.e. organisation rather than organisation). The Google Scholar search used the same terms, with the top 100 returns considered. Also, given that a recent review of organisational change literature noted that limiting searches to top journals can be restrictive (see Oreg and Berson, 2019), two organisational change journals were also searched, The Journal of Applied Behavioral Science and Journal of Change Management. A full search strategy is detailed in Appendix 1. Non-peer reviewed studies did not form part of this review and were eliminated during the screening to ensure a high degree of methodological quality. This review was also limited to studies published in English with no restrictions on publication date given the relative novelty of the phenomena of interest. Following the search, 2986 items were loaded into Zotero 6.0.23 where duplicates were removed, yielding 2882 unique papers for screening.
2.2. Study selection
For these articles, the titles and abstracts were then screened independently by two reviewers (one the primary author) and assessed against the set inclusion criteria, which were (1) qualitative analysis, (2) articles where studied cases were greater than one, (3) case selection was unbiased towards successful (or unsuccessful) outcomes, (4) emphasis was placed on the practice, process, or methodology that enabled transformation and (5) where transformation outcomes were reported. Following screening, the two reviewers met and discussed their selected studies, at this stage agreement between the two reviewers was 73%. Disagreements were resolved through discussion and consensus was reached on 38 papers that represented the selection criteria before moving forward.
2.3. Data extraction and synthesis
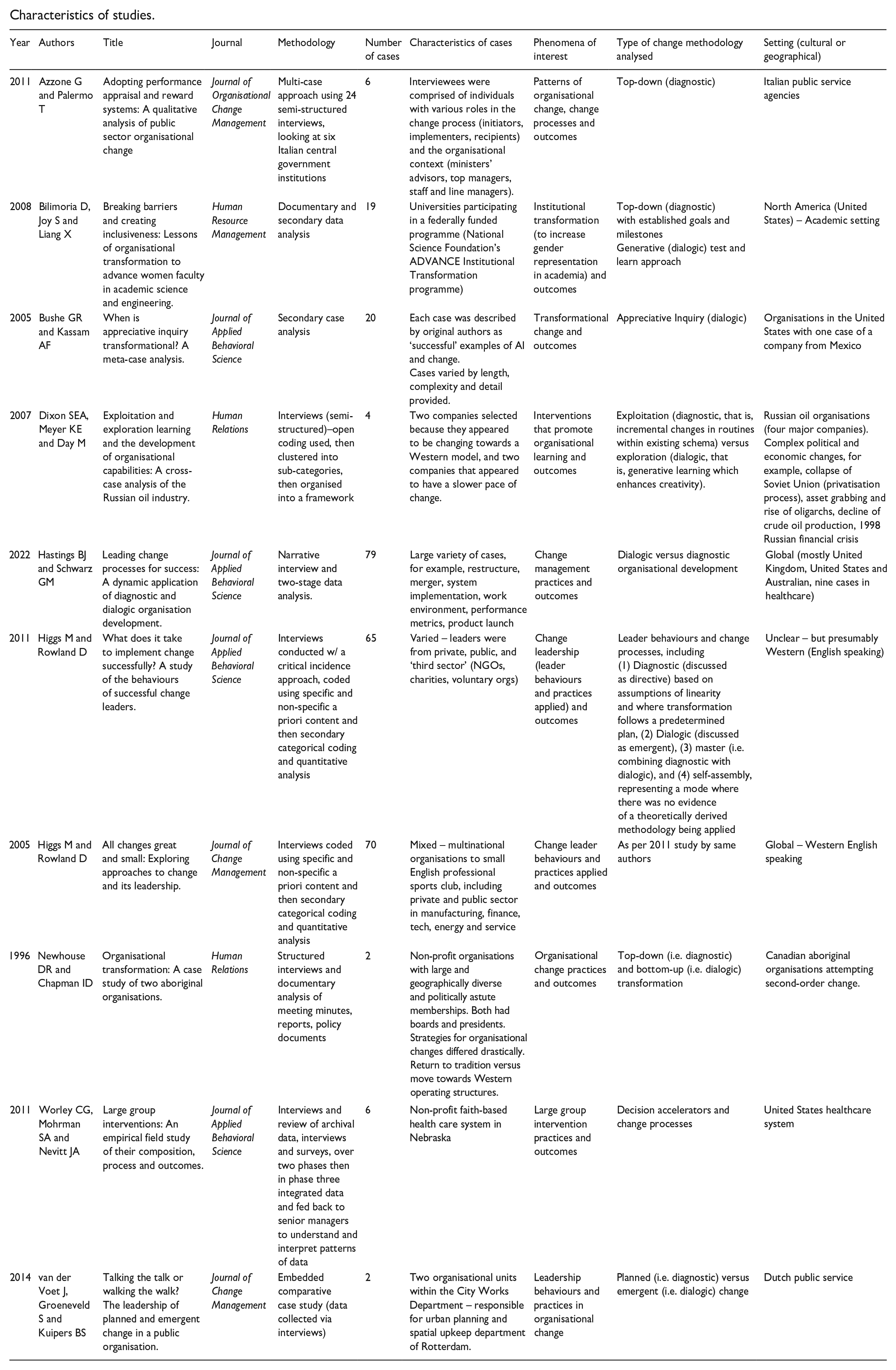
For these 38 papers, full articles were retrieved by both reviewers. Data were then extracted included using the JBI data extraction tool, appropriate for this study given that this tool guides the extraction of qualitative data on standard and specific themes. Standard criteria included year of publication, author, title, research method, number of cases studies, characteristics of cases studies, phenomena of interest, type of change methodology and study setting – for examples, please see Appendix 3. In addition, specific extraction themes were identified that directly related to the research questions, including how diagnostic and dialogic related to outcomes and how leaders of successful change interacted with their followers.
Findings related to change management practices and transformation outcomes were correlated between researchers. What differed between papers was the terminology used to describe the methodology. For example, van der Voet et al. (2014) utilised planned versus emergent practices, Higgs and Rowland (2005, 2011) used directive and emergent, and Newhouse and Chapman (1996) described dictatorial and interpretive. For the synthesis of findings below, analysis drew upon Bushe and Marshak’s (2015) integrative summary of change management practices, which interprets planned, directive and dictatorial to represent diagnostic processes, and both emergent and interpretive represent dialogic processes. This summary builds on prior work that bifurcates change management practices into similar themes (as per Burnes, 2004; Bushe and Marshak, 2009; Weick and Quinn, 1999) and represents a commonly utilised nomenclature in the field of organisation development (see Bartunek and Jones, 2017; Burnes, 2017).
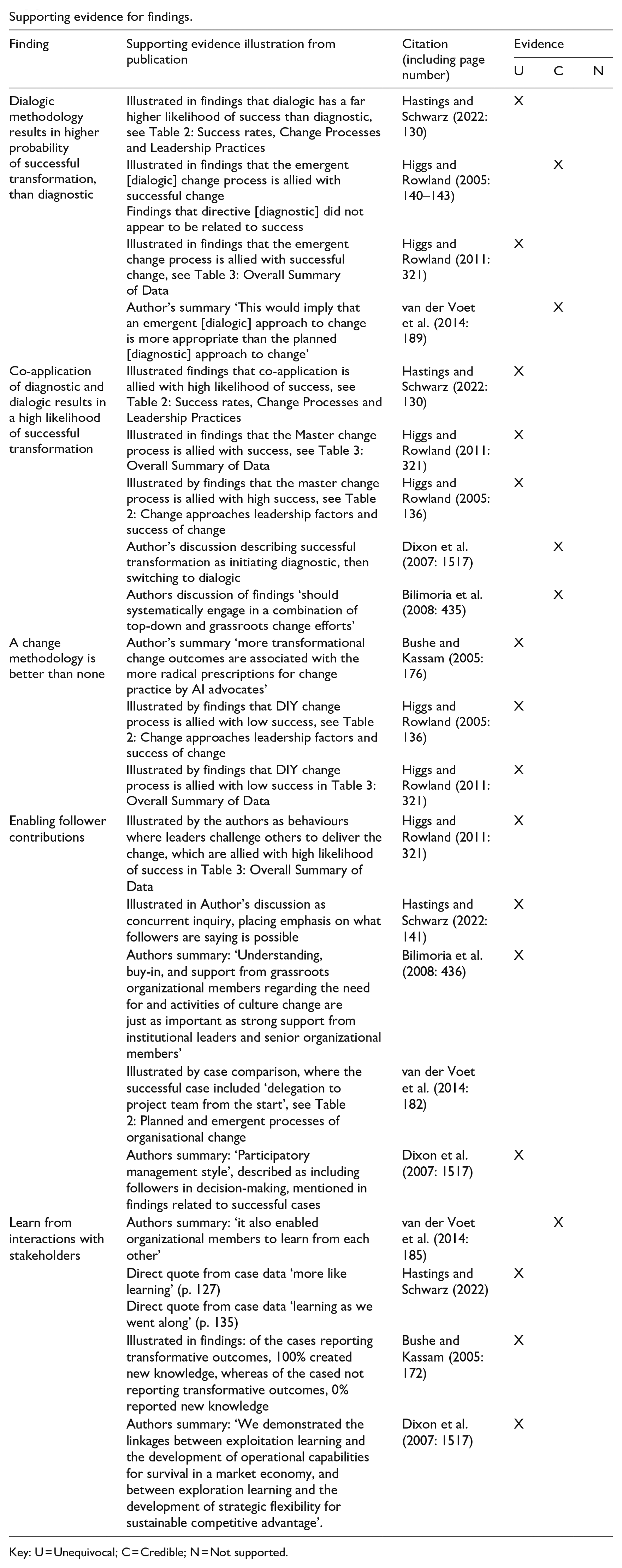
Findings related to how leaders interacted with followers were pooled using JBI SUMARI with the meta-aggregation approach. This approach involved both reviewers separately summarising the key findings of each paper related to this theme and assigning an independent level of credibility to individual findings – unequivocal, credible, or unsupported – then compared between reviewers and mutually agreed findings assembled into similar themes. For instance, several papers described the significance of the theme of stakeholder engagement, here individual paper findings were aggregated into a set of statements on this theme, where these findings were represented unequivocally in two or more studies they were included in the results, together with a fuller explanation in the published output.
3. Results
From the initial 2882 articles, 38 were fully assessed. Of this set, a further 22 were excluded because, on full review of these papers, the study inclusion criteria were not deemed to have been met. The remaining 16 articles were analysed for methodological quality and data extraction, where six studies were ruled out as they did not pass the quality appraisal. Overall, this analysis resulted in a final total of 10 papers, representing 292 cases of transformation for qualitative synthesis. The characteristics of these studies are illustrated in Appendix 3.
3.1. Assessment of methodological quality
The methodological quality of these reviewed papers was assessed versus the 10 criteria of JBI evidence synthesis, as presented in Table 1. Regarding congruency between research objectives and methodology and methods, all papers contextualised the researcher culturally or theoretically, were conducted ethically as far as was assessable, and conclusions or interpretations of their data flowed logically from the analysis of their results. For the criteria of influence of the researcher on the research and vice versa, both reviewers agreed that this was not applicable for the Bilimoria et al.’s (2008) and Bushe and Kassam’s (2005) papers because they were secondary case analysis. These two studies were included because the authors represented the findings of studied cases transparently and, where possible, with direct quotations. Another paper where the researcher’s perspective was not applicable was Worley et al.’s (2011) study, but was included because of the strict criteria and structure required for the implementation and analysis of large group interventions.
Critical appraisal results for included studies.
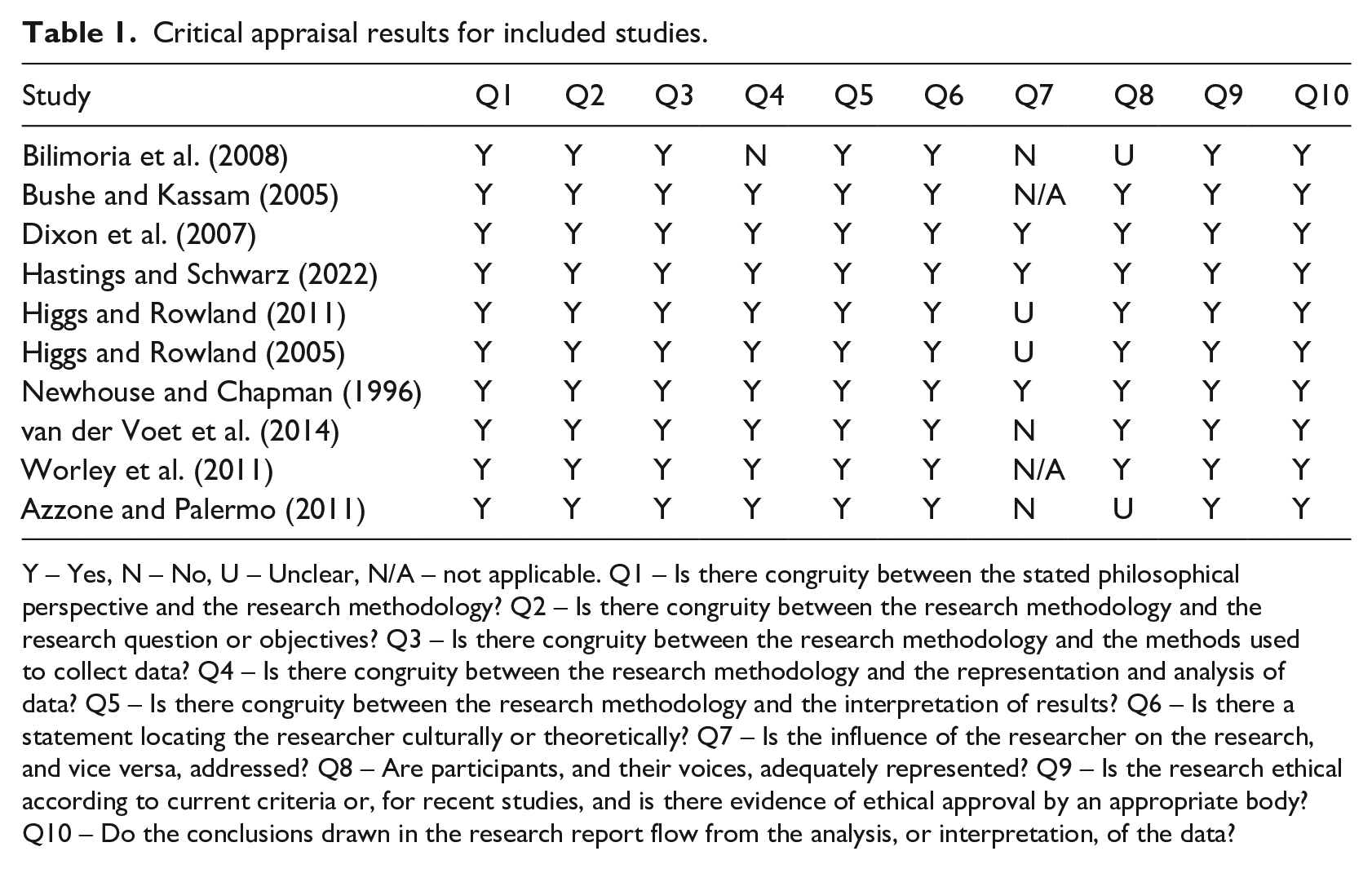
Y – Yes, N – No, U – Unclear, N/A – not applicable. Q1 – Is there congruity between the stated philosophical perspective and the research methodology? Q2 – Is there congruity between the research methodology and the research question or objectives? Q3 – Is there congruity between the research methodology and the methods used to collect data? Q4 – Is there congruity between the research methodology and the representation and analysis of data? Q5 – Is there congruity between the research methodology and the interpretation of results? Q6 – Is there a statement locating the researcher culturally or theoretically? Q7 – Is the influence of the researcher on the research, and vice versa, addressed? Q8 – Are participants, and their voices, adequately represented? Q9 – Is the research ethical according to current criteria or, for recent studies, and is there evidence of ethical approval by an appropriate body? Q10 – Do the conclusions drawn in the research report flow from the analysis, or interpretation, of the data?
Across the Higgs and Rowland (2005, 2011) articles, as well as the studies from Azzone and Palermo (2011) and van der Voet et al. (2014) papers, these authors did not address whether their influence had an impact on findings. These studies were still chosen for inclusion in this review because they presented multiple direct quotations from organisational actors to illuminate evidence which was logically related to findings, also interpretations of data was aligned with a stated philosophical perspective and methodology.
3.2. Characteristics of included articles
Reviewed studies represent 292 individual cases of transformation. All 10 studies evaluated change management practices and transformation outcomes, although the stated phenomena of interest utilised various terminology such as institutional transformation (Bilimoria et al., 2008), transformational change (Bushe and Kassam, 2005) or organisational learning (Dixon et al., 2007). Healthcare specific cases were explored by Worley et al. (2011) who studied six healthcare systems and Hastings and Schwarz’s (2022) study of nine cases from healthcare. Included studies were predominantly set in North America or other English-speaking Western countries (e.g. Australia and the United Kingdom), with the exceptions of four studies: Bushe and Kassam (2005) included one case of a Mexican company in their paper, Dixon et al. (2007) studied four Russian oil organisations, van der Voet et al. (2014) analysed two cases from the Dutch public service, and Hastings and Schwarz (2022) included two cases from South America. Separately, a unique cultural consideration was presented by Newhouse and Chapman (1996) who studied two Canadian Aboriginal organisations. Multiple levels of participants and cases were included, this ranged from departments within an organisation (van der Voet et al., 2014; Worley et al., 2011), to entire organisations or institutions (Azzone and Palermo, 2011; Bilimoria et al., 2008; Bushe and Kassam, 2005; Dixon et al., 2007; Newhouse and Chapman, 1996), with some studies mixing these two contexts (Hastings and Schwarz, 2022; Higgs and Rowland, 2005, 2011).
4. Findings
Findings indicate that the choice of change management practice and how leaders engage with followers when following these practices are important differentiators between success and failure. Due to the nature of reviewed studies, some presented as qualitative summaries and others represented with quantitative summaries of qualitative themes, meta-analysis was not possible. In what follows, aggregated findings are presented in qualitative form, with the evidence supporting these findings available in Appendix 4.
4.1. Considering the basis for change management advice
One fundamental consideration for policymakers and practitioners is whether there is any benefit in following a change management practice. Three studies explored this theme, comparing the use of an established change practice with a ‘do it yourself’ (DIY) approach. All three studies identified that following a practice resulted in more successful outcomes than DIY. For instance, both Higgs and Rowland (2005, 2011) studies identified DIY, whereby those tasked with change were assessed as not following a methodology, instead inventing their own approach to transformation. Across both papers, this absence of an adhered to practice led to a low probability of successful outcomes. Furthermore, Bushe and Kassam (2005) study of 20 cases of dialogic transformation, identified that the faithfulness of practitioners to theory was also a factor that influenced outcomes, with higher adherence to established change practices corresponding to more transformative outcomes. The authors concluded that, ‘more transformational change outcomes are associated with the more radical prescriptions for change practice’ (Bushe and Kassam, 2005: 176). Specifically, one of the factors that underpinned this finding was that dialogic principles should be applied wholeheartedly, rather than superficially.
4.2. Considering change management practices and outcomes
Findings highlight that the type of change management practice had considerable influence on the outcome of transformation. The difference in outcomes between these two practices was not small, instead, as Newhouse and Chapman (1996: 1004) summarised ‘our interest in examining the process of change of these two organisations was stimulated by the sharp contrast in outcomes’. Overall, across the cases identified in this review, dialogic trumped diagnostic, with application of dialogic consistently allied with more successful outcomes.
Four of the 10 studies compared diagnostic and dialogic practices with transformation outcomes, representing 216 cases of transformation, confirming that these two practices were allied with starkly contrasting likelihoods of success. For instance, Hastings and Schwarz (2022) studied 79 instances of transformation including nine cases from healthcare, with data gathered from semi-structured narrative interviews and outcomes classified as either successful or not successful. From this data set, the authors identified seven cases that solely used dialogic methodology with successful outcomes in 86% of cases. In contrast, in 49 cases diagnostic was applied solely, with successful outcomes reported in only 9% of these cases.
Separately, Higgs and Rowland (2011), studied 65 cases of change. This mixed methods study identified four types of change methodology: (1) directive (or diagnostic, as per Bushe and Marshak, 2015) based on assumptions of linearity and where transformation follows a predetermined plan, (2) emergent (or dialogic, as per Bushe and Marshak, 2015), (3) master (i.e. combining diagnostic with dialogic) and (4) self-assembly, representing DIY. In their results, Higgs and Rowland (2011) identified 11 cases with emergent (dialogic) methodology, where success was reported in 63% of cases, contrasting with seven cases of directive (diagnostic), with 28% reported successfully.
An earlier and separate study by Higgs and Rowland (2005), using the same classification of change management practices, presented a study of 70 cases of transformation across seven organisations, with data gathered from informants involved in the transformation. The authors categorised outcomes in terms of magnitude of change, while controlling the type of transformation (long term and short term), noting that ‘an emergent [dialogic] approach to change appeared to be more successful than any of the other three change approaches in most contexts’ (p. 143) and ‘particularly important to success in contexts of high-magnitude change’ (p. 140). Their quantitative analysis showed that emergent change accounted for 32% of the variance in success. In contrast, this article also identified that the diagnostic approach was negatively, although not significantly, correlated with success, leading the authors to state that this diagnostic ‘approach to change does not appear to be related to success in any context’ (p. 140). In addition, a comparative study of two organisational units within the Dutch public sector also reported a similar difference in outcomes (see van der Voet et al., 2014). Here, the successful case used dialogic to facilitate conversational structures that resulted in positive outcomes. In contrast, the unit that applied diagnostic was categorised as unsuccessful.
4.3. Considering modes of application of change management practices
While the application of dialogic alone was allied with a higher likelihood of success, when compared to diagnostic, five studies also identified that co-application of these two practices also yielded success. This finding is supported by Hastings and Schwarz (2022), who identified 17 cases that commenced as diagnostic then switched to dialogic, with success reported in 92% of these cases. Also, Higgs and Rowland (2011) identified 36 cases of co-application, reporting success in 72% of cases (contrasting to 28% success for diagnostic).
Furthermore, Higgs and Rowland (2011: 328) found that master (diagnostic and dialogic) was allied with higher success than diagnostic, summarising that ‘approaches to change that operate within a framework that posits change as a complex phenomenon [i.e. Master and Emergent] are more successful than approaches that adopt a more linear and sequential viewpoint [i.e. Directive and Self-assembly]’. The other study by Higgs and Rowland (2005) also identified that the master approach achieved successful transformation outcomes – with a likelihood of success comparable to solely-dialogic. This finding was also discussed by Dixon et al. (2007), who noted that successful cases used diagnostic methodology to give transformation structure, then iterated between diagnostic and dialogic. This phenomenon was also noted by (Bilimoria et al., 2008: 435) who suggested that future transformations ‘should systematically engage in a combination of top-down and grassroots change efforts’.
4.4. Considering how leaders engaged with followers
Seven studies explored the nature of the leader-follower interaction through the lens of stakeholder engagement. For instance, Worley et al. (2011), who studied large group interventions across six healthcare systems in Nebraska, contextualised that getting the whole system in the room was an important enabler of successful transformation. Common to six of these studies was emphasis on followers, as Bilimoria et al. (2008) explained, ‘understanding, buy-in, and support from grassroots organisational members regarding the need for and activities of culture change are just as important as strong support from institutional leaders and senior organisational members’. This broad study set enabled exploration of the interaction between leader-follower interactions, resulting in two findings related to how leaders engaged with followers that were allied with success. What studies also explored were cases where this engagement was absent, with a corresponding negative association with transformation outcomes.
4.4.1 Enabling follower contributions
Facilitating success was more nuanced than the process of engagement with followers. As van der Voet et al. (2014: 185) explained, ‘more emphasis on participation does not automatically lead to the anticipated results’. What also mattered was constructing transformation in a way that followers contributed to the change effort. This study described the importance of delegation of decisions from leaders to followers – such engagement enabled contributions from employees regarding the transformation, which made desired changes more concrete and relevant. Supporting this finding, Hastings and Schwarz (2022) identified that leaders who incorporated the bottom-up contributions of followers, highlighting that leaders who made an effort to understand their issues, then acted on those issues typically led successful transformations. What was interesting about these findings is that the alterations to prior plans were relatively minor, such as small adjustments to deadlines. Also, Dixon et al. (2007) showed that organisational learning followed from a participatory management style that encouraged participants to contribute their own innovations and take risks.
In addition, Higgs and Rowland (2011) described the importance of being follower-centric. This study compared leader-centric behaviours, where decision-making was enacted top-down, and follower-centric behaviours, where leaders challenge others to deliver the change, finding support that the latter was allied with successful transformation. Separately, Worley et al. (2011) identified that the relative degree of representation between follower groups was identified as a factor that differentiated success from failure, where engagements with a higher than representative number of physicians were negatively related to outcomes, whereas engagement that included higher community representation was positively correlated with outcomes.
4.4.2 Learn as we go
Four studies identified a link between learning and transformation outcomes, specifically how those tasked with enabling transformation learned from their interactions with stakeholders, as well as enabling followers to learn from each other. In one of these studies, van der Voet et al. (2014: 185) identified that decision-making concentrated on top management only served to reinforce existing ways of organising, whereas decision-making completed collaboratively with followers promoted learning and, crucially, positive transformation. Framing change as a learning journey was evident in two cases studied by Hastings and Schwarz (2022), where case data described transformation as ‘more like learning’ (p. 127) and ‘learning as we went along’ (p. 135). Contrastingly, this same study characterised several failed cases where learning did not occur because leaders avoided listening to the issues and concerns raised by participants of change, preferring to stick to pre-defined plans.
Furthermore, Dixon et al. (2007) identified two types of learning, exploration learning that was focused on the acquisition and assimilation of new knowledge and exploitation learning focused on understanding more effective and efficient operating procedures. Exploration learning was identified as an outcome of dialogic and allied with the successful outcomes. Finally, Bushe and Kassam (2005: 172) identified a 100% correlation between cases where new knowledge was created and more transformative outcomes, contrastingly of the less transformative outcomes, no cases reported that new knowledge was created.
4.5. Summary of findings
This review finds that applying a change practice is better than DIY. It also finds that dialogic is far more successful across a variety of contexts when contrasted with diagnostic. However, dialogic need not be applied solely, it can be co-applied with diagnostic for a high likelihood of success. This review also highlights aspects of leadership that should be expressly considered when embarking on transformation. One finding was that those tasked with enacting change should take particular care to ensure that stakeholders contribute to decision-making during the transformation process. Also, studies identified that leaders should approach transformation with a view to establishing a learning environment, rather than reinforcing previous ways of thinking.
5. Discussion
Presently, transformation in healthcare operates within a paradigm of diagnostic. Given the sharp contrast in outcomes between diagnostic and dialogic identified in this review, these findings point to an opportunity for healthcare to step outside of contemporary thinking and embrace dialogic. Indeed, it is possible that the adoption of dialogic will help healthcare ameliorate its ‘implementation problem’. However, findings also show that consideration of dialogic is more nuanced than the direct pivot from diagnostic to dialogic that commentators propose, specifically the two practices can be co-applied, and consideration should also be given to the capability of leaders to enact dialogic. With these findings as a basis, this review provides consideration for healthcare policy guidance on change management practices, implications for healthcare practitioners and considerations for organisational change scholarship.
5.1. Policy implications
Policymakers should be made aware of this evidence that supports dialogic. Breaking out of the diagnostic paradigm and embracing dialogic will require policymakers to take the lead. While it is possible to argue that healthcare practitioners are free to explore available change management practices, for instance by applying dialogic on their own initiative, the reality is that healthcare seems to be an industry that follows the prevailing guidance (see Harrison et al., 2021). Thus, without clear permission to experiment with dialogic from policymakers, it is hard to see how this practice will become more widely utilised. The alternate path is to continue with diagnostic guidance and accept the evidence in this review that this practice is associated with a low likelihood of success.
Organisational change scholarship has embraced dialogic. Why healthcare has remained tied to diagnostic is unknown, perhaps it is the ‘plan then do’ approach of diagnostic that resonates with the evidence-based and planned approach of researching disease, identifying cures, and designing appropriate models of care. While diagnostic may be a relevant practice for medical research settings, transformation impacts the nature of organising, which in healthcare is complex, involving many interacting agents and components (see Burton et al., 2018; Resnicow and Page, 2008). Over the years, organisational change researchers have taken time to explore why reductionist ‘plan then do’ approaches were inadequate for transformation within complex organisational contexts (see Burnes, 2005; Bushe and Marshak, 2009), what has emerged from this research is the dialogic practice, drawing from understandings of how complex systems interact. Until now, what has been missing from this discussion is a wide scale review of the evidence that compares the efficacy of diagnostic and dialogic. Perhaps, given the evidence-based mind-set of healthcare policy, this lack of empirical evidence has held back policymakers from embracing commentators’ calls for dialogic. Hopefully, the evidence presented in this review piques interest among policymakers for exploring dialogic.
An argument against an immediate extension of healthcare policy guidance to dialogic is the relatively smaller number of healthcare-focused cases identified in this review. While the idea that ‘healthcare is different’ may be a factor that moderates the direct translation of these findings into healthcare contexts, policymakers should take note of three factors that support consideration of dialogic. First, the stark contrast in outcomes between diagnostic and dialogic. Here, it is not a case where one practice was found to be slightly better than the other, instead research reviewed in this article shows that the difference in achieving success can be as low as one in three attempts with diagnostic and as high as four out of five with dialogic (see Hastings and Schwarz, 2022; Higgs and Rowland, 2005; 2011). Given the combination of transformation challenges and limited resources within healthcare, the magnitude of this difference in outcomes warrants attention. Second, recent studies in healthcare have also pointed to the benefits of dialogic. There is an emerging evidence base in healthcare that has identified how elements of dialogic-based practice, specifically the bottom-up engagement with stakeholders, has contributed to positive outcomes. Examples include greater innovation in clinical care (e.g. better testing, embracing of telehealth, better engagement; see Uhl-Bien, 2021), wider scale adoption of innovation (see Choi et al., 2024), improved sustainability of interventions (see Harrison et al., 2021), and better experience of employees with change (see Nilsen et al., 2020). These findings mean that this review does not stand on its own and considering this present study alongside these examples places these findings within a broader and richer narrative that supports embracing dialogic. Third, present diagnostic-focussed guidance may limit the possibility of more evidence being attained. Given the propensity for healthcare practitioners to follow present guidance on diagnostic, policymakers must recognise that their guidance is integral to practice and that if they wish to understand more about the efficacy of dialogic in healthcare settings, they must first encourage experimentation with it.
When it comes to updating guidance on change management practices, transitioning to dialogic is more nuanced than the direct pivot from diagnostic to dialogic that commentators propose (see Bevan and Fairman, 2014; Braithwaite et al., 2018). The finding that a high likelihood of success can be achieved by co-applying diagnostic and dialogic change practices means that updating policy guidance need not be an ‘out with the old and in with the new’ approach. Instead, guidance for dialogic can be given alongside, and in extension of, present diagnostic-focussed guidance. Updating guidance should also include leadership capabilities for change, specifically encouraging engaging stakeholders and fostering a learning environment. As van der Voet et al. (2014) identified, leadership decision-making that concentrated on top management only served to reinforce existing ways of working, whereas decision-making that engaged stakeholders promoted learning and, crucially, led to positive transformation. Healthcare is known for its traditional top-down to leadership, however the concept of bottom-up engagement is gaining traction, especially since the Covid pandemic (see Helm-Murtagh and Erwin, 2024). Together, findings of this review provide helpful context for the update of policy guidance to include dialogic, alongside present explanations of diagnostic, together with descriptions of leadership capabilities that promote positive stakeholder engagement during transformation.
5.2. Practical implications
Practitioners should be made aware that there is an alternate practice to the available policy guidance. Against a backdrop that healthcare has an ‘implementation problem’, it may be difficult for practitioners to fathom that something as simple as a choice between change management practices is what matters. Indeed, a problem-centred narrative is a form of passive resistance to change because it frames transformation as a waste of time and effort (see Smollan, 2011). The findings of this review add empirical evidence to shift this debate from ‘implementation problem’ to ‘how change is conducted matters’, providing hope and confidence that required transformations can be achieved.
An important finding for practitioners is how these two practices can be co-applied, meaning that dialogic can be viewed as additive to existing knowledge on change management practices, rather than a replacement. Illustrations are available detailing how these two practices work together (see Bushe and Marshak, 2009; Bushe and Marshak, 2015) and one of the papers explored in this review offers a conceptual model for practitioners describing the choice points that precede a switch between them (Hastings and Schwarz, 2022). It is also important to note that two of the papers studied in this review identified successful cases of dialogic transformation in healthcare (see Hastings and Schwarz, 2022; Worley et al., 2011). Practitioners should take note of this evidence for contexts when they need to convince others of the efficacy of proposing dialogic.
5.3. Extending the practical utility of organisational change theory
Organisational change scholarship has been a traditional source of guidance for healthcare policymakers. However, while care has been taken in this field to decode and describe two contrasting practices of transformation, an important omission has been data to inform which one is more successful. Considering that Kurt Lewin’s maxim, ‘there is nothing as practical as a good theory’, it seems that the mistake here is that while change management practices have been codified following deep observations of practice (e.g.: Hiatt, 2006; Kanter et al., 1992; Kotter, 1996; Lewin, 1947), they have not subsequently been tested to confirm their efficacy when applied to practice. Indeed, as has been noted, change scholarship has overlooked empirical evidence that tests the relevance of these theories to practice (see Oreg and Berson, 2019; Stouten et al., 2018). With this context, the results of this review provide important data that extend the practical utility of change management practices. With this context, these findings also have implications beyond healthcare, indeed the ‘implementation problem’ narrative spans many industries (see Jarrell, 2017; Schwarz et al., 2021). Here, findings provide a bright spot of hope that a low probability of success need not always be the case.
5.4. Limitations
One limitation is the limited number of cases that report on dialogic from healthcare settings. Relevant studies may also have been missed because this review included only those studies with listed search terms in the databases employed. Another potential limitation is publication bias, since the 1950s, scholars have noted that systematic reviews based only on published studies are subject to the file drawer problem, referring to the underrepresentation of studies with negative or relatively small effects, potentially skewing the outcome of this review. Since publication bias primarily affects the outcome (effect size) of studies available for inclusion, its influence on findings is likely limited. The same applies to the decision to restrict this systematic review to English-language studies.
5.5. Future research
Extending present guidance to include dialogic will not be easy, and prior examples illustrate that navigating a path of updating policy requires consideration of more than evidence alone. As Brownson et al. (2009) explain, attention should be given to (1) content, the identification of specific policy elements that are likely to be effective; (2) process, approaches that enhance the likelihood of policy adoption; and (3) outcomes, the potential impact of policy. With this context and given the small number of healthcare studies identified in this review; creating opportunities to study dialogic in healthcare is an immediate priority. Furthermore, scholarship could also explore a broader view of the likely outcomes of a policy shift to dialogic. One possible focus is staff wellbeing, especially since ‘burnout’ is the most commonly cited reason why an increasing number of doctors and nurses are resigning (Cornish et al., 2021; Sheather and Slattery, 2021). Future scholarship could also explore the barriers of adopting dialogic, with a view to facilitating wider and quicker uptake.
6. Conclusion
The evidence gathered in this review suggests that for healthcare agencies tasked with providing guidance on change management practices, consideration of dialogic will bring forward a helpful tool that enables healthcare to meet the transformational challenges of today and tomorrow. Embracing dialogic should be complementary to existing approaches, allowing healthcare to build from its existing knowledge of diagnostic. Furthermore, attention should also be given to two leadership capabilities – engaging stakeholders and promoting a learning environment – that support the application of dialogic for success.
Key practical and research implications
Footnotes
Appendix 1
Appendix 2
Appendix 3
Characteristics of studies.
| Year | Authors | Title | Journal | Methodology | Number of cases | Characteristics of cases | Phenomena of interest | Type of change methodology analysed | Setting (cultural or geographical) |
|---|---|---|---|---|---|---|---|---|---|
| 2011 | Azzone G and Palermo T | Adopting performance appraisal and reward systems: A qualitative analysis of public sector organisational change | Journal of Organisational Change Management | Multi-case approach using 24 semi-structured interviews, looking at six Italian central government institutions | 6 | Interviewees were comprised of individuals with various roles in the change process (initiators, implementers, recipients) and the organisational context (ministers’ advisors, top managers, staff and line managers). | Patterns of organisational change, change processes and outcomes | Top-down (diagnostic) | Italian public service agencies |
| 2008 | Bilimoria D, Joy S and Liang X | Breaking barriers and creating inclusiveness: Lessons of organisational transformation to advance women faculty in academic science and engineering. | Human Resource Management | Documentary and secondary data analysis | 19 | Universities participating in a federally funded programme (National Science Foundation’s ADVANCE Institutional Transformation programme) | Institutional transformation (to increase gender representation in academia) and outcomes | Top-down (diagnostic) with established goals and milestones Generative (dialogic) test and learn approach |
North America (United States) – Academic setting |
| 2005 | Bushe GR and Kassam AF | When is appreciative inquiry transformational? A meta-case analysis. | Journal of Applied Behavioral Science | Secondary case analysis | 20 | Each case was described by original authors as ‘successful’ examples of AI and change. Cases varied by length, complexity and detail provided. |
Transformational change and outcomes | Appreciative Inquiry (dialogic) | Organisations in the United States with one case of a company from Mexico |
| 2007 | Dixon SEA, Meyer KE and Day M | Exploitation and exploration learning and the development of organisational capabilities: A cross-case analysis of the Russian oil industry. | Human Relations | Interviews (semi-structured)–open coding used, then clustered into sub-categories, then organised into a framework | 4 | Two companies selected because they appeared to be changing towards a Western model, and two companies that appeared to have a slower pace of change. | Interventions that promote organisational learning and outcomes | Exploitation (diagnostic, that is, incremental changes in routines within existing schema) versus exploration (dialogic, that is, generative learning which enhances creativity). | Russian oil organisations (four major companies). Complex political and economic changes, for example, collapse of Soviet Union (privatisation process), asset grabbing and rise of oligarchs, decline of crude oil production, 1998 Russian financial crisis |
| 2022 | Hastings BJ and Schwarz GM | Leading change processes for success: A dynamic application of diagnostic and dialogic organisation development. | Journal of Applied Behavioral Science | Narrative interview and two-stage data analysis. | 79 | Large variety of cases, for example, restructure, merger, system implementation, work environment, performance metrics, product launch | Change management practices and outcomes | Dialogic versus diagnostic organisational development | Global (mostly United Kingdom, United States and Australian, nine cases in healthcare) |
| 2011 | Higgs M and Rowland D | What does it take to implement change successfully? A study of the behaviours of successful change leaders. | Journal of Applied Behavioral Science | Interviews conducted w/ a critical incidence approach, coded using specific and non-specific a priori content and then secondary categorical coding and quantitative analysis | 65 | Varied – leaders were from private, public, and ‘third sector’ (NGOs, charities, voluntary orgs) | Change leadership (leader behaviours and practices applied) and outcomes | Leader behaviours and change processes, including (1) Diagnostic (discussed as directive) based on assumptions of linearity and where transformation follows a predetermined plan, (2) Dialogic (discussed as emergent), (3) master (i.e. combining diagnostic with dialogic), and (4) self-assembly, representing a mode where there was no evidence of a theoretically derived methodology being applied |
Unclear – but presumably Western (English speaking) |
| 2005 | Higgs M and Rowland D | All changes great and small: Exploring approaches to change and its leadership. | Journal of Change Management | Interviews coded using specific and non-specific a priori content and then secondary categorical coding and quantitative analysis | 70 | Mixed – multinational organisations to small English professional sports club, including private and public sector in manufacturing, finance, tech, energy and service | Change leader behaviours and practices applied and outcomes | As per 2011 study by same authors | Global – Western English speaking |
| 1996 | Newhouse DR and Chapman ID | Organisational transformation: A case study of two aboriginal organisations. | Human Relations | Structured interviews and documentary analysis of meeting minutes, reports, policy documents | 2 | Non-profit organisations with large and geographically diverse and politically astute memberships. Both had boards and presidents. Strategies for organisational changes differed drastically. Return to tradition versus move towards Western operating structures. | Organisational change practices and outcomes | Top-down (i.e. diagnostic) and bottom-up (i.e. dialogic) transformation | Canadian aboriginal organisations attempting second-order change. |
| 2011 | Worley CG, Mohrman SA and Nevitt JA | Large group interventions: An empirical field study of their composition, process and outcomes. | Journal of Applied Behavioral Science | Interviews and review of archival data, interviews and surveys, over two phases then in phase three integrated data and fed back to senior managers to understand and interpret patterns of data | 6 | Non-profit faith-based health care system in Nebraska | Large group intervention practices and outcomes | Decision accelerators and change processes | United States healthcare system |
| 2014 | van der Voet J, Groeneveld S and Kuipers BS | Talking the talk or walking the walk? The leadership of planned and emergent change in a public organisation. | Journal of Change Management | Embedded comparative case study (data collected via interviews) | 2 | Two organisational units within the City Works Department – responsible for urban planning and spatial upkeep department of Rotterdam. | Leadership behaviours and practices in organisational change | Planned (i.e. diagnostic) versus emergent (i.e. dialogic) change | Dutch public service |
Appendix 4
Supporting evidence for findings.
| Finding | Supporting evidence illustration from publication | Citation (including page number) | Evidence | ||
|---|---|---|---|---|---|
| U | C | N | |||
| Dialogic methodology results in higher probability of successful transformation, than diagnostic | Illustrated in findings that dialogic has a far higher likelihood of success than diagnostic, see Table 2: Success rates, Change Processes and Leadership Practices | Hastings and Schwarz (2022: 130) | X | ||
| Illustrated in findings that the emergent [dialogic] change process is allied with successful change |
Higgs and Rowland (2005: 140–143) | X | |||
| Illustrated in findings that the emergent change process is allied with successful change, see Table 3: Overall Summary of Data | Higgs and Rowland (2011: 321) | X | |||
| Author’s summary ‘This would imply that an emergent [dialogic] approach to change is more appropriate than the planned [diagnostic] approach to change’ | van der Voet et al. (2014: 189) | X | |||
| Co-application of diagnostic and dialogic results in a high likelihood of successful transformation | Illustrated findings that co-application is allied with high likelihood of success, see Table 2: Success rates, Change Processes and Leadership Practices | Hastings and Schwarz (2022: 130) | X | ||
| Illustrated in findings that the Master change process is allied with success, see Table 3: Overall Summary of Data | Higgs and Rowland (2011: 321) | X | |||
| Illustrated by findings that the master change process is allied with high success, see Table 2: Change approaches leadership factors and success of change | Higgs and Rowland (2005: 136) | X | |||
| Author’s discussion describing successful transformation as initiating diagnostic, then switching to dialogic | Dixon et al. (2007: 1517) | X | |||
| Authors discussion of findings ‘should systematically engage in a combination of top-down and grassroots change efforts’ | Bilimoria et al. (2008: 435) | X | |||
| A change methodology is better than none | Author’s summary ‘more transformational change outcomes are associated with the more radical prescriptions for change practice by AI advocates’ | Bushe and Kassam (2005: 176) | X | ||
| Illustrated by findings that DIY change process is allied with low success, see Table 2: Change approaches leadership factors and success of change | Higgs and Rowland (2005: 136) | X | |||
| Illustrated by findings that DIY change process is allied with low success in Table 3: Overall Summary of Data | Higgs and Rowland (2011: 321) | X | |||
| Enabling follower contributions | Illustrated by the authors as behaviours where leaders challenge others to deliver the change, which are allied with high likelihood of success in Table 3: Overall Summary of Data | Higgs and Rowland (2011: 321) | X | ||
| Illustrated in Author’s discussion as concurrent inquiry, placing emphasis on what followers are saying is possible | Hastings and Schwarz (2022: 141) | X | |||
| Authors summary: ‘Understanding, buy-in, and support from grassroots organizational members regarding the need for and activities of culture change are just as important as strong support from institutional leaders and senior organizational members’ | Bilimoria et al. (2008: 436) | X | |||
| Illustrated by case comparison, where the successful case included ‘delegation to project team from the start’, see Table 2: Planned and emergent processes of organisational change | van der Voet et al. (2014: 182) | ||||
| Authors summary: ‘Participatory management style’, described as including followers in decision-making, mentioned in findings related to successful cases | Dixon et al. (2007: 1517) | X | |||
| Learn from interactions with stakeholders | Authors summary: ‘it also enabled organizational members to learn from each other’ | van der Voet et al. (2014: 185) | X | ||
| Direct quote from case data ‘more like learning’ (p. 127) |
Hastings and Schwarz (2022) | X | |||
| Illustrated in findings: of the cases reporting transformative outcomes, 100% created new knowledge, whereas of the cased not reporting transformative outcomes, 0% reported new knowledge | Bushe and Kassam (2005: 172) | X | |||
| Authors summary: ‘We demonstrated the linkages between exploitation learning and the development of operational capabilities for survival in a market economy, and between exploration learning and the development of strategic flexibility for sustainable competitive advantage’. | Dixon et al. (2007: 1517) | X | |||
Key: U = Unequivocal; C = Credible; N = Not supported.
Acknowledgements
The author would like to acknowledge the constructive comments provided during the review process by the editorial and reviewing team.
Final transcript accepted 26 November 2024 by Andrew Jackson (Editor-in-Chief ).
Funding
The author received no financial support for the research, authorship and/or publication of this article.