
Abstract
This article identifies change and learning within a complex ecosystem aiming for healthy ageing through action research. Learning, innovation and progress are all referred to as change. Reflecting on a surprisingly good outcome within a collaborative project between dental care and municipal healthcare, fearing that change and learning from a predetermined outcome could overshadow elements that enabled change, a theoretical flow approach was used as an entrance to perspectives of change and learning. Flow approach made it possible to sense movement, focusing on timing, attentionality and undergoing. A research question was formulated: What change and learning outcomes can be identified through the lens of a flow approach? By looking beyond the project, focusing on what enabled change, actions could be traced that might have been overlooked in the absence of a flow approach. Although oral health is important for health, interprofessional collaborative projects have, to our knowledge, never been explored using a flow approach. This article contributes to theory by broadening perspectives on change and learning. Long-term interprofessional collaboration became evident as an enabling factor when mapping the emergence of change through a flow approach aiming for healthy ageing.
Keywords
Introduction
Some say that today’s work life is constantly changing (Barnett, 2004; Billett, 2009), indicating a need for lifelong learning in work life (Edmondson & Saxberg, 2017). However, change, interprofessional learning and learning at work are often considered primarily as nouns, that is, a change, the process of interprofessional learning or an approach (Cacciattolo, 2015; Gellerstedt et al., 2015; Truong et al., 2022). Change and learning are also frequently studied in light of identified key actors (Long et al., 2019; Persson et al., 2022). In this article, learning, innovation and progress are referred to as flowing change. Through a flow approach, change and learning can be traced in a non-actor-centred, dynamic way (Baygi et al., 2021). Although it is said that people learn in interaction with others (Fenwick, 2006), a theoretical entry point including enabling opportunities for learning would seem important, to address the question of how. Theoretically, while not focusing solely on or downplaying certain key stakeholders or activity systems, we attempt to consider learning beyond them. A flow approach contributes to learning by taking account of dynamic aspects such as timing and by sensing opportunities for action, reinvention and rediscovery (Baygi et al., 2021; Hultin et al., 2021). Reflecting on the outcomes of a collaborative project between dental care and municipal healthcare, an overall research question was formulated: What change and learning outcomes can be identified through the lens of a flow approach?
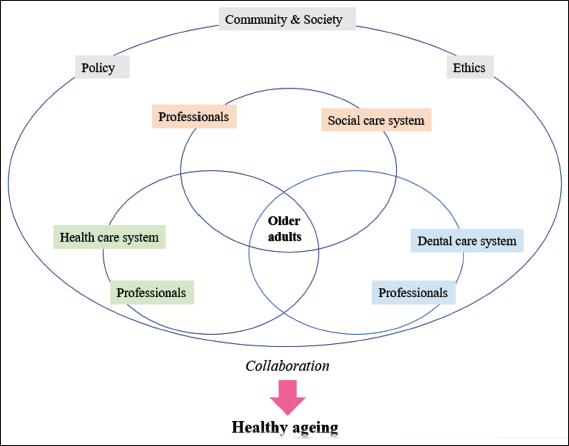
Demographically, an increasingly ageing population is suffering from multiple chronic diseases (United Nations, 2022; WHO, 2021). Various interprofessional approaches enable healthy ageing (WHO, 2021), with learning considered a prerequisite for change. How learning and change are defined, discussed and considered is therefore crucial. Today, as people age they retain more teeth and often have advanced oral prosthetics than previous generations (Norderyd et al., 2015), highlighting the need for collaboration between dental care and healthcare. However, despite oral health being part of general health, collaboration is rare due to differing financial systems, management structures, organisations, documentation systems, cultures and education (The National Board of Health and Welfare, 2019). Figure 1 is inspired by Batalden et al. (2016) and visualises an ecosystem of healthy ageing. It is concluded that actors engage in change and learning within an ecosystem to pursue different goals, from their varied perspectives (Wang, 2021). Engeström and Sannino (2011) described how contradictions are important for creating organisational change; bearing that in mind, much could be learned about change from studying collaboration during health care planning within the ecosystem of healthy ageing (Figure 1).
Older adults with frailty have an increased risk of poor oral health (Hakeem et al., 2019). Poor oral health is, for example, correlated to cardiovascular disease (Kelly et al., 2013), respiratory disease (Azarpazhooh & Leakeames, 2006), malnutrition (Van Lancker et al., 2012) and diabetes (Kudiyirickal & Pappachan, 2015). Suffering from poor oral health also affects life by causing pain and reduced well-being (Kandelman et al., 2008). Diminished cognitive and/or physical abilities often lead to decreased ability to maintain oral hygiene and to a risk of losing previous regular dental care contacts (Grönbeck-Lindén et al., 2016). With increasing risk of oral disease in a period of life when many lose access to regular dental care, oral health should be considered in arenas other than dental care organisation, such as municipal healthcare organisation (Andersson et al., 2017; Ek et al., 2018). However, few studies examine interprofessional collaborations between dental care and healthcare professionals in practice, approaching the interventions from a non-predetermined way. This article identifies changes during oral health care planning, illustrating this with the narrative of a municipal organisation launching overall strategic work with the goal of increasing the number of oral health assessments of older adults using the Revised Oral Assessment Guide (ROAG) on older adults within municipal healthcare. Simultaneously, a collaborative project was being launched between public dental care and the municipal organisation (Persson et al., 2022). In sum, a whole pattern of change warranted attention so it could be understood and described.
Theoretical Framework
A Flow Approach
To describe dynamic aspects and contribute to theory regarding collaborative, interprofessional change, a theoretical flow approach inspired by Baygi et al. (2021) was used.
A project can be reduced to project meetings in which a static process map shows how the project has been evolving, often from the perspective of predetermined stakeholders (Baygi et al., 2021). This reduces the project to a static matter. The flow perspective could allow consideration of dynamic aspects of learning and change, including various dimensions in describing how change emerges. The flow approach enables us to describe change in a moving, flowing way (Baygi et al., 2021). From views of change and learning flow theory could offer a way to identify learning that cannot be predicted, underlining the dynamic aspects of learning. One striking example of how the flow approach contributes to learning theory is through the lens of Schön (1987). When approaching learning, Schön (1987) described humans acting and learning from what comes to them, that is, reflecting-in-action, developing both theory and practice. The flow approach can decentralise our entrance to workplace learning, focusing not on the actors or their surroundings, but rather on learning as the changing flow of action (Hultin et al., 2021). Consider surfing the ocean waves: Changes happening when learning to surf the waves are complex to describe, and major concerns such as ocean currents and wind must be considered (Baygi et al., 2021).
From a flow perspective, actions could be regarded as flowing lines, continuously needing to be acted upon and learned from (Baygi et al., 2021). These flowing lines can connect and give rise to change, just like waves, and are characterised through three dimensions: Timing, attentionality and undergoing. By timing, one can approach how things emerge and evolve, in an ongoing process, from different times and places, making it possible to activate particular learning elsewhere and at other times.
Attentionality comes from the word attention, indicating that flow does not refer solely to human-actor–centric activity. When surfing, numerous circumstances need attention, and we can react to these with more or less intention. Attentionality highlights how things emerge from events (e.g., walking, talking and listening) (Hultin et al., 2021). What are sensed as meaningful possibilities to be responded to are sensed through attentionality (Introna, 2018). Undergoing highlights the importance of becoming through rediscovering and reinventing, entering the possibilities of flow (Hultin et al., 2021).
Material and Methods
Empirical Setting
From 2018 to 2021, a collaborative project in a municipality in western Sweden aimed to support healthy ageing from an oral health perspective (Persson et al., 2022). The municipality, with about 110,000 residents (20 per cent aged 65+) had an organisation of about 2,600 professionals, including registered nurses, nursing assistants, case managers and the head of operations. Also, three local head nurses work full time strategically to ensure compliance with healthcare legislation (SFS 2017:3010). Two dental hygienists from public dental care were hired within the project part-time to work at a strategic level within the municipal organisation and with the local head nurses.
In 2018, the municipal healthcare organisation relaunched the Senior Alert quality register to enhance preventive healthcare. The goal was to screen 90 per cent of those aged 65+ in municipal healthcare. From 2019 to 2021, a process leader and head of operations communicated results quarterly and held biannual meetings with managers to discuss outcomes and create action plans when needed.
Senior Alert, a Swedish quality register, is used in nursing healthcare among people ≥65 years old (Senior Alert, 2022). The purpose of Senior Alert is to improve the health and care of older adults by systematically screening, registering and taking actions in five risk areas, that is, malnutrition, falls, pressure ulcers, bladder dysfunction and oral health, and by following up after rehabilitation efforts (Senior Alert, 2022). The assessments are conducted by nursing staff when older adults enrol in long-term care, home healthcare or regional healthcare. After that, the assessments are conducted on an ongoing basis at least once a year.
Risk assessments in Senior Alert use evidence-based tools like the ROAG, known for its validity and reliability (Andersson et al., 2002; Everaars et al., 2020). ROAG aims to reduce oral ill-health and integrate aspects of oral health into nursing care, enhancing the overall health of older adults. ROAG offers preventive action recommendations when risk for poor oral health is found and advises contacting caregivers for severe issues. A Swedish study (Bellander et al., 2021a) found that half of older adults in 2016 had at least one ROAG assessment in Senior Alert. However, a follow-up study (Bellander et al., 2021b) highlighted assessment shortcomings, suggesting a need for structured training and better collaboration between nursing and dental care. These findings indicate a knowledge gap regarding ROAG within nursing care and a potential need for ROAG courses to be refined and more integrated into nursing.
Insider/Outsider Research Team Approach
This study describes interprofessional change from and learning between 2018 and 2021, with action research making it possible to capture the inherent movement (Avison et al., 1999). Within the research group, an insider/outsider research team-approach (Louis & Bartunek, 1992) was used. This has many positive outcomes, for example, the insiders can help the outsiders get more involved in organisational matters, and the outsiders can help the insiders develop a more distanced approach. Emphasising the notion of timing (Baygi et al., 2021), the ‘insider/outsider’ research approach was considered appropriate. Being solely on the ‘outside’ as a researcher can make it difficult to capture the effects of timing and the journey that insiders have experienced, sensing timing within practice (Bourdieu, 2000). Throughout the research process, these perspectives gave rise to a thorough understanding of the project, complementing and facilitating one another. In order to describe change enabled through collaboration, the research group considered meta-learning gained from not focusing on one static issue, for example, a new ROAG course, fearing that this could obscure the dynamic dimensions of learning. The possibility of missing important pieces of overall change was discussed continuously. Two of the authors (JPK and ABA) are considered ‘insiders’, being dental hygienists and closely involved in the collaborative project (JPK and ABA). One researcher is regarded as ‘in between’, having great experience of research in gerodontology and also being involved in the collaborative project (CH). Two of the authors participated as ‘outsiders’, contributing experience of work-integrated learning (AS) and organisational change (SPK) (Kylén et al., 2004). They were detached from the collaborative project and municipal organisation.
Data Collection
To answer the overall research question, ‘What change and learning outcomes can be identified through the lens of a flow approach?’, a mixed-method approach was used. This is considered an appropriate method for exploring a phenomenon for which neither qualitative nor quantitative data are sufficient to answer the research question (Venkatesh et al., 2013). Table 1 summarises the data collection.
Summary of the Data Collection Including Stakeholders.
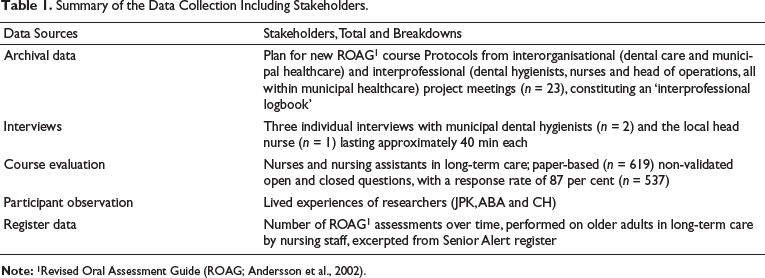
The emergence of change was documented through 23 interorganisational and interprofessional meetings, considered an ‘interprofessional logbook’, covering December 2018 to December 2021. These protocols mainly described collaboration, evaluation and transformation issues. Additional data included three in-depth interviews with two municipal dental hygienists and one local head nurse, conducted in early 2020 by JPK (interviewed local head nurse) and SPK (interviewed dental hygienists), each lasting about 40 min and transcribed verbatim. From 2019 to 2021, staff from 37 of 44 long-term care units (84 per cent) participated in a new ROAG course. Afterwards, nursing staff completed a short evaluation with three closed and three open questions, rating the course from 1 (very poor) to 6 (very good). Researchers JPK, ABA and CH used their lived experiences when writing the narrative of the results.
Data Analysis
Qualitative content analysis contributed to the overall analytical structure (Graneheim & Lundman, 2004). All qualitative data were processed and read several times. A tentative analysis was conducted by JPK and ABA and then discussed and revised within the research group. The analytical process started with an inductive approach, using the data to gain a theoretical understanding (Elo & Kyngäs, 2008; Graneheim et al., 2017; Krippendorf, 2013). In using flow theory to understand the outcomes of workplace learning, the theory gradually came to form a basis for the continued analysis, and the analytical process steadily moved towards a deductive approach. The Statistical Package for the Social Sciences (SPSS version 25, IBM) was used when analysing the quantitative data (i.e., the course evaluation forms and number of oral assessments registered in Senior Alert). Quantitative data from the course evaluation and the Senior Alert register data were presented in frequencies, per cents, medians, means and standard deviations. The quantitative data added colour and perspective to the qualitative analysis, and eventually all data were included in a qualitative content analysis with a deductive approach. In sum, starting with diverse data (Table 1) and a mixed quantitative/qualitative approach, a deductive, integrated mixed-method approach eventually yielded meaningful results, based on the overall research question. As a result, the initial concrete content analysis and the quantitative analysis became intertwined, abstracted and integrated into five major themes strongly inspired by a flow approach (Baygi et al., 2021). Representative quotations and statistics are presented in the next section.
Results
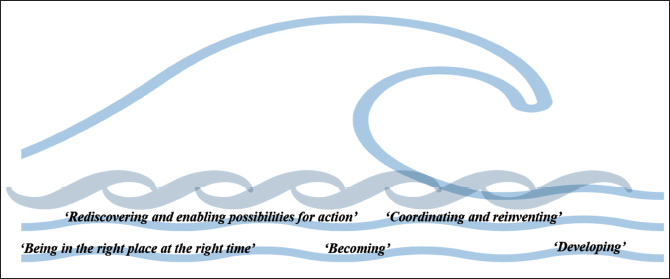
To convey what was contributing to change aiming towards healthy ageing, the results will be presented as a storyline, to be approached in terms of dynamic, flowing waves, emerging from and influencing one another. The five themes identified in the results are depicted in Figure 2: ‘Being in the right place at the right time’, ‘Developing’, ‘Becoming’, ‘Rediscovering and enabling possibilities for action’ and ‘Coordinating and reinventing’. Each theme is dependent on and intertwined with several others, adding revised perspectives, depth and colour to one another.
Five Major Themes Mapping the Emergence of Change and Learning Through Collaboration, Representing the Results.
One identified change outcome is a major, 10-fold increase in the number of ROAG assessments from 2018 to 2021: In 2018, 224 ROAG assessments were performed by nursing staff on frail older adults in the municipal organisation, whereas in 2021, 2127 such assessments were performed. Integrating a flow approach when describing the journey of change and learning makes it possible to capture the emergence of different aspects contributing to this 10-fold increase.
Being in the Right Place at the Right Time
A 4-year collaborative project between municipal healthcare and dental care began in October 2018 (Persson et al., 2022). Before its launch, the municipal healthcare organisation had set goals, relaunched Senior Alert and aimed to offer ROAG assessments to older adults in long-term care, thereby identifying a need for improved ROAG training for staff.
The collaborative project aimed to support the municipal organisation’s ROAG work and contribute to its goals through assisting with courses of the nursing staff. The project manager (JPK) attended a standardised, theoretical two hour ROAG course in another municipality to learn how to conduct ROAG training. The course, designed for long-term care nursing assistants, was theoretical, lacked interaction and follow-up due to organisational differences. This experience inspired the project manager, the municipal dental hygienists and the local head nurses within the collaborative project to develop and test a new ROAG course based on partnership with municipal healthcare and dental care, aligning with ongoing Senior Alert and ROAG efforts.
Developing
A tentative course plan was formulated by the project manager from dental care, who developed it iteratively through discussion with professionals in the municipal organisation and the dental care organisation. A new ROAG course was to include both the nursing and dental care perspectives. Moreover, a gap was identified: No instruments for oral examinations were available for conducting ROAG assessments. Leading staff the municipal organisation decided to equip all units with electric torches and mouth mirrors for nursing staff conducting ROAG assessments. This initiative was deemed crucial for promoting oral health care planning within the municipal healthcare system. One local head nurse described the situation:
Yes, that’s how I remember it was before then. Back then we didn’t have the kit [i.e., mouth mirror and electric torch] that was needed. So that’s something that has developed over time. (Local head nurse)
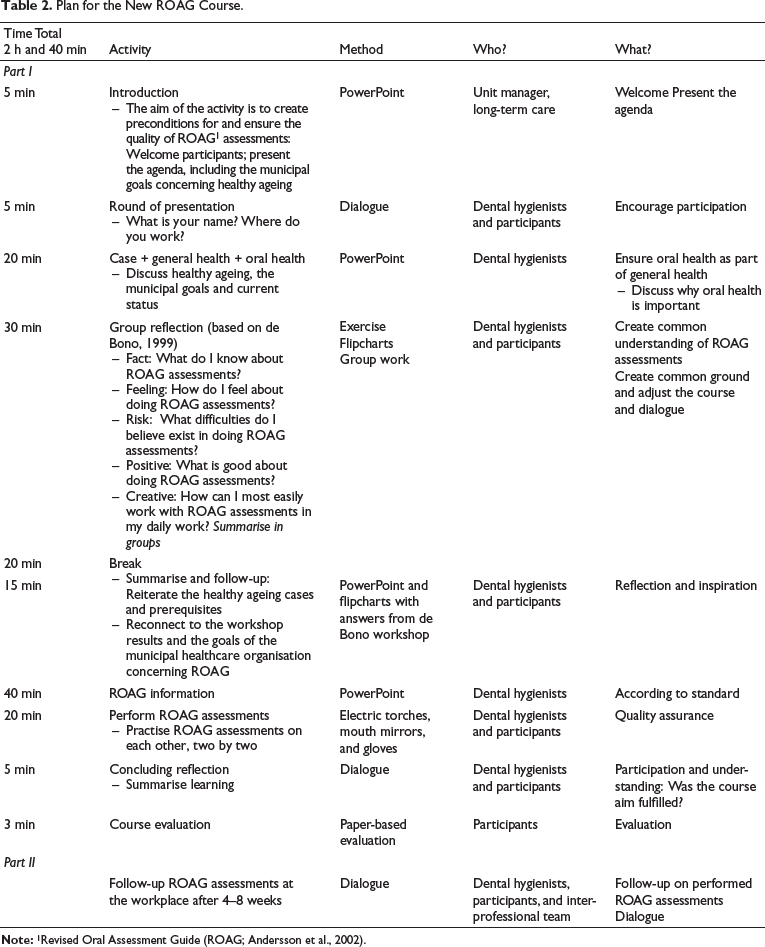
The first new ROAG course took place in February 2019 with seven nurses attending. After the course, the nurses highlighted the need for more guidance on post-assessment actions. This feedback was considered, and the planned follow-up was deemed essential to ensure a shared understanding of these aspects. Table 2 presents a plan for a new ROAG course.
Plan for the New ROAG Course.
Becoming
To enable change, different professionals needed to reflect on how they could contribute to the ‘becoming’ of integrating oral health perspective within processes of overall health care.
The structured reflection based on de Bono (1999) was included because reflection is considered crucial for learning. As seen in Table 1 the course included a practical part, which was discussed throughout the project. Answers to open-ended questions from the evaluation repeatedly fostered discussion. Some nursing staff requested more time to practise the ROAG assessments. Other nursing staff considered practising ROAG assessments to be too intimate, and instead proposed using a dummy:
Get a dummy for the practical part. … I would never let anyone else dig around in my mouth: it fills you with anxiety and feels like a violation. But I do understand why you want us to do it. (Nursing assistant A)
The practical part was also considered from the perspective of improving participants’ understanding of how it feels to have someone performing oral assessments. Rediscovering and approaching oral health issues in new ways seemed to be important dimensions for professional learning. Several quotations conveyed similar reflections:
Go ahead and try getting examined… – then you’ll know how the users feel. (Nursing assistant B)
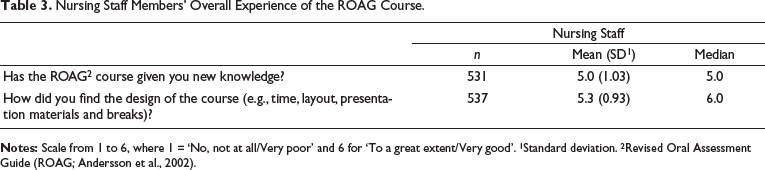
The importance of testing, feeling and reflecting was significant for ROAG course participants, given the strong integrity and ethical concerns associated with oral health. Course evaluations revealed that nursing staff valued the new knowledge and overall structure of the course (Table 3). From 2019 to 2021, 619 nursing staff participated in ROAG courses within the collaborative project.
Nursing Staff Members’ Overall Experience of the ROAG Course.
Rediscovering and Enabling Possibilities for Action
After the ROAG course, the municipal dental hygienists attended follow-up team meetings at workplaces. These meetings involved interprofessional teams, including nurses, physiotherapists and nursing assistants, to discuss ROAG assessments. One dental hygienist noted that these follow-up meetings allowed her to monitor learning progress effectively.
We were able to come back again and take part in the various team meetings, and so we followed up on how things had gone. … I found that I had seen changes since the training session. (Municipal Dental hygienist)
The follow-up meetings became a form of ongoing evaluation, in which ROAG assessments and outcomes were revisited and, for example, recommended actions were noted and discussed—among other health issues.
Coordinating and Reinventing
While new ROAG courses were conducted, 23 interprofessional and interorganisational meetings monitored the overall collaborative project, including ROAG training and implementation. These dialogues enabled professionals to identify opportunities for action and change, such as developing oral health care planning for frail older adults in homecare. Initially, the dental hygienists were unfamiliar with staff roles and logistics, but municipal coordinators ensured courses were fully booked and appropriately staffed. During the Covid-19 pandemic, coordination was crucial, adapting ROAG training to online formats or smaller in-person sessions. Collaborative meetings facilitated planning for additional training, such as palliative oral care.
Discussion
Results Discussion
In a sense, collaboration and movement have been ‘guiding stars’ of the results presented here. By viewing change and learning from a flow perspective, enabling factors emerged when describing a 10-fold increase in the number of ROAG assessments. Describing change regarding ROAG assessments as a 10-fold increase is correct, although representing only a snapshot of the outcome. It does not capture the movement, the emergent collaborative coordination, the development of the new course, the ongoing quality assurance (including mouth mirrors, electric torches and follow-up) and dialogue aids used when discussing oral health. None of these elements was predetermined but emerged as important for change and learning when sensing opportunities for action through the interprofessional collaborative project. Adding a flow approach and tracing change and learning along actions made it possible to describe the story of change.
Timing
The results indicated that collaboration between different professionals can lead to shared actions to promote oral health care planning, as shown by the increased number of ROAG assessments and improved quality in terms of the use of correct instruments (e.g., mouth mirrors and electric torches). Baygi et al. (2021) emphasised the notion of timing, rather than time, when considering change. The collaborative project was established at a productive time. Timing was important when considering how the municipal organisation had formulated the goal of enabling healthy ageing, which included a desire to increase work with ROAG assessments.
Casting light on certain predetermined outcomes based on chronological time could overshadow other outcomes, emerging over time. For example, focusing solely on the increased number of ROAG assessments might have concealed the enabling factors in the surroundings, such as interprofessional collaboration. One of the dental hygienists concluded from attending follow-up interprofessional team meetings in long-term care, after the initial ROAG course, that she sensed how learning had happened. Exactly when it happened was unclear, but she did sense change and learning.
Attentionality
Viewing the ROAG course as a dynamic issue, along with the de Bono workshop, follow-ups and evaluations, highlighted the complexity of integrating oral health outside dental clinics. The collaborative project provided a continuous learning base (Persson et al., 2022). ROAG courses were discussed at municipal team meetings, with assessments reported, analysed and communicated to long-term care managers. This was likely crucial for change, given the complex division of oral health responsibilities among dental care, social care and healthcare (The National Board of Health and Welfare, 2019).
Engeström and Sannino (2010) used the ‘horizon’ metaphor when describing learning. Learning as a horizon—that is, something dynamic that tends to shift and change with movement—is a suitable metaphor when encountering attentionality. In the present results, flowing storylines of action were emerging and paid attention by various professionals in different organisations. Activities within long-term collaboration could not always be described as intentional, with predetermined outcomes; rather, activities within the collaborative project seemed to trigger several unplanned actions. This seemed to enable meaningful opportunities to be sensed, potentially contributing to integrating knowledge within oral health and municipal care.
Undergoing
Learning is situated through participation in practices, leading to the expansion of ideas and objects and inducing stakeholders to translate knowledge (Fenwick, 2006). The present results note the increase in the number of ROAG assessments. The mobilisational and empowering aspects of learning are captured by these data—different professionals reinvented themselves from their professional points of view, taking divergent actions to integrate oral health and municipal care.
The practical component of the ROAG course encouraged nursing staff to reflect on oral health and their professional responsibility. Practicing, performing and receiving ROAG assessments sparked numerous reactions and discussions. Given the intimate nature of the oral health (Lindqvist et al., 2013), staff suggested using dummies for future practical training. In the future, participants could choose to practice on dummies or colleagues, with the latter option helping them understand the experience of receiving a ROAG assessment.
Methodological Discussion
When applying a flow approach, the question of how to capture this change in an understandable way is problematic. As Hultin et al. (2021) concluded, it is very difficult to go beyond the actors when considering such a change. From the perspective of learning horizons, it would be important to challenge this dynamic aspect even more, to problematise how change can be identified and discussed.
Moving between inductive and deductive approaches entails challenges, and Graneheim et al. (2017) have stated that it is important to discuss the data remaining after such a combined research approach. In this article, the focus has been on change concerning ROAG, whereas the data addressed other issues as well. However, the overarching research question called for a primary focus: If the approach had not been intentionally limited, the results would have been overly broad and vague.
Finally, two dimensions are missing: The experiences of older adults and the outcome in terms of healthy ageing. Further research is clearly needed in these areas.
Ethics
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Swedish Ethics Review Authority (Dnr. 119-14 & 2020-04724). The Authority stated that there was no need for ethical approval, but the authors nevertheless obtained written advisory opinions.
Conclusion
The overall research question was: What change and learning outcomes can be identified through the lens of a flow approach? Applying a flow approach made it possible to sense movement, described as flowing lines of action, in a non-predetermined or non-actor-centred way. For example, using a flow approach allowed different paths towards a 10-fold increase in the number of ROAG assessments in a municipal organisation to be traced and described. Long-term interprofessional collaboration became apparent as an enabling factor when enabling healthy ageing during oral health care planning. The various methods used in research determine the story of change and learning and thereby define what change and learning are. Future research should continue to develop creative methods based on a flow approach, rendering movement and becoming within change and learning tractable and possible to study.
Footnotes
Acknowledgements
The authors are grateful to all participants in this study. Sincere acknowledges to Ms Beatrice Odenö, Mrs Christina Vinge Appelkvist, Ms Emma Johansson, Mrs Maria Ragnefil and Mrs Monica Ringdahl for sensing possibilities for action, contributing to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the Local Research and Development Board of Fyrbodal, Region Västra Götaland, Sweden, the Health Promotion Research Funding, Region Västra Götaland, Sweden and the Swedish Order of Freemasons, Grand Lodge of Sweden.