
Abstract
Cancer care represents a challenge for the healthcare systems of OECD member states. This also applies to the Netherlands, as cancer is the leading cause of death. High quality of care is essential to effectively tackle the burden of disease caused by cancer. According to the WHO health systems framework, quality is an intermediate goal of health systems, alongside safety, access and coverage. This study aimed to assess the quality of cancer care in the Netherlands, especially in terms of effectiveness. To assess the quality of cancer care in the Netherlands, participation rates in screening and 5-year survival rates for breast, cervical and colorectal cancer were used. The Netherlands is interested in ensuring quality healthcare, and quality is one of the three main objectives of the healthcare system. The 5-year survival rates for breast, cervical and colorectal cancer were above the respective OECD averages in 2014, but some countries are better positioned. Participation in screening for cervical cancer was relatively low in the Netherlands in 2017, below the OECD average. It can be concluded that the Netherlands has high-quality, effective cancer care and is striving to continuously improve it. However, there is room for improvement , especially with regard to participation in cervical cancer screening, transparency about the quality of healthcare and regional differences in the quality of care.
Introduction
As the Netherlands is one of the five wealthiest countries in the euro zone, the population holds high expectations regarding the quality of healthcare (Kroneman et al., 2016, p. 198). As in many other industrialised countries, the Netherlands’ number of people with chronic diseases and multimorbidity is increasing due to rising life expectancy and associated demographic changes, as well as medical and technological progress. Due to improvements in diagnosis and treatment options, cancer is increasingly developing into a chronic disease (Kroneman et al., 2016, p. 12). In 2016, cancer was the main cause of death, representing a major challenge for healthcare in the Netherlands (Organisation for Economic Co-operation and Development [OECD], 2020).
According to estimates by the OECD, a third of cases could be cured with timely detection and appropriate treatment, and another 30% could be prevented by adequate public health measures. Although OECD member states have made numerous efforts to improve cancer prevention and treatment, there is still room for improvement (OECD, 2013, p. 3). Cancer care in the Netherlands performs well, but can still be developed further in international comparison (OECD, 2013, pp. 35–108).
This study aimed to assess the quality of cancer care in the Netherlands, particularly in terms of effectiveness. First, the selected country is described using economic and socio-demographic factors, followed by a description of the health status of its population. The Dutch healthcare system is then presented. This is followed by a conceptual explanation of the intermediate objective of the quality of a healthcare system, based on which the quality of cancer care in the Netherlands is presented and assessed.
The Netherlands had a total of 17,231,017 inhabitants in 2018. Over the past decades, life expectancy has continuously improved. From 1990 to 2017, it rose from 77 to 82 years (see Table 1). Life expectancy in the Netherlands in 2017 is thus higher than the average of 80 years in OECD member states. The life expectancy of women at 83 years is in line with the OECD average (83 years) and that of men at 80 years is higher (78 years) (The World Bank, 2020).
Mortality and Health Indicators, 1990–2018 (selected years).
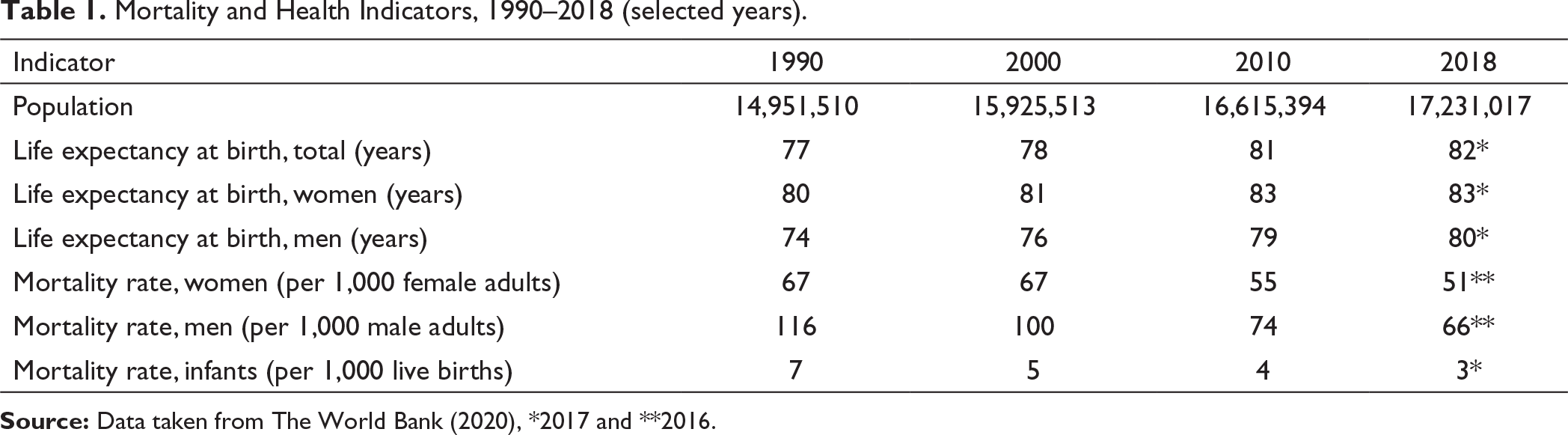
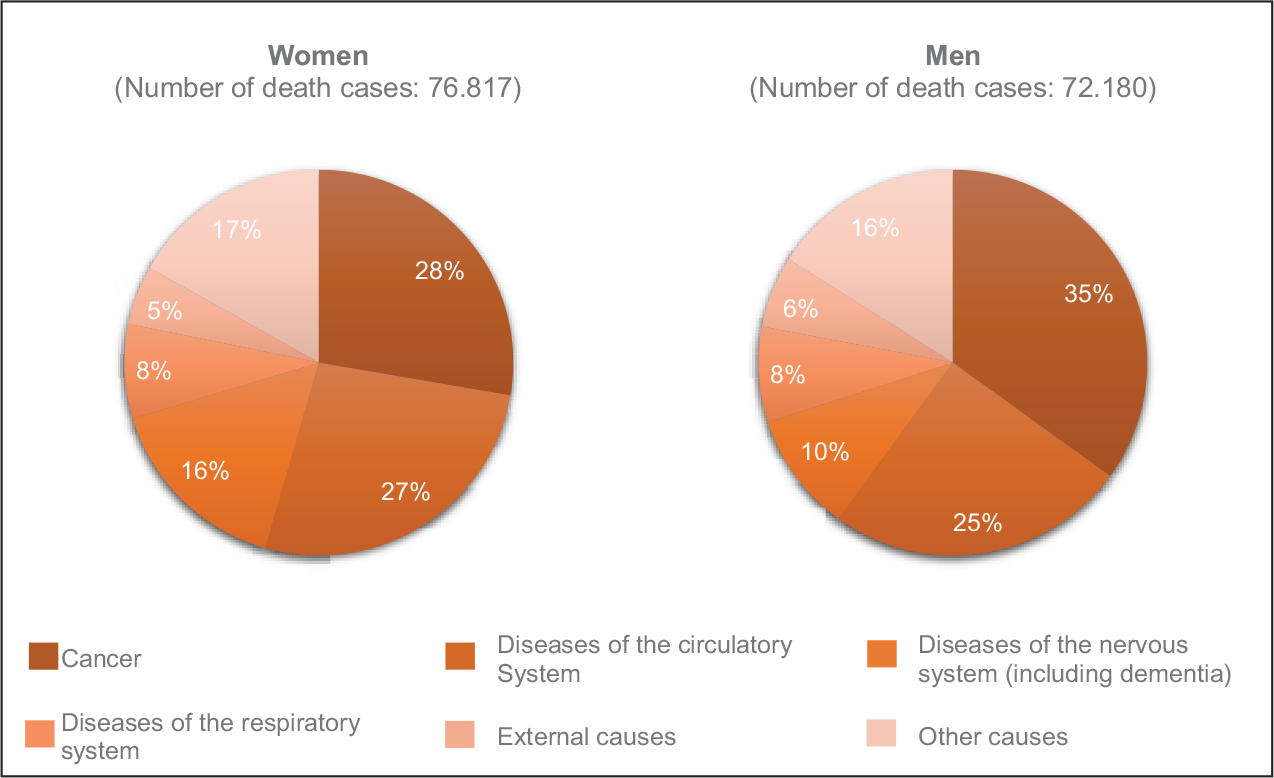
The mortality rates shown in Table 1 imply that they are declining for all age groups. The increase in life expectancy is based, in particular, on the decline in cardiovascular mortality (OECD and European Observatory on Health Systems and Policies, 2017, p. 2). The main cause of death is cancer for both women and men. Cardiovascular diseases are in the second place. In 2016, malignant neoplasms accounted for 35% of deaths in men and 28% in women (see Figure 1). The greatest burden of disease is caused by mental disorders, cardiovascular diseases and cancer (Kroneman et al., 2016, p. 10).
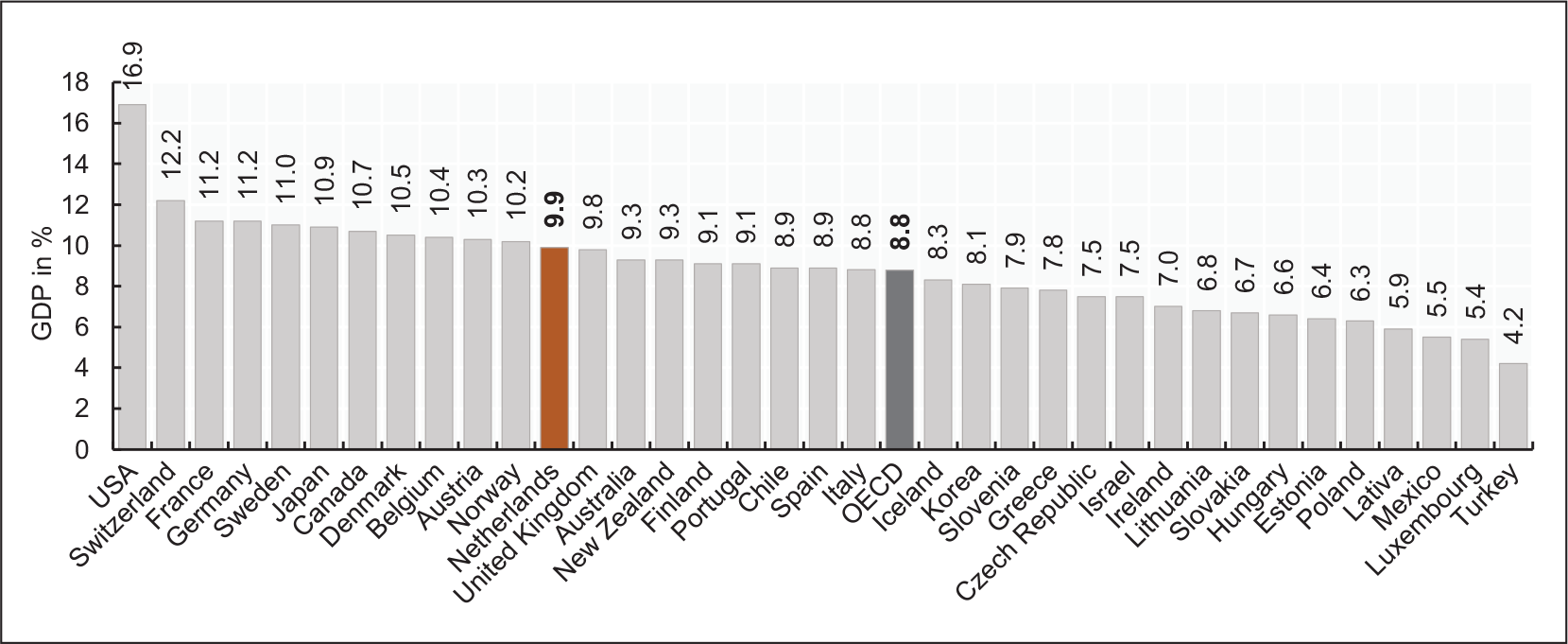
The gross domestic product (GDP) per capita (56,772.0 PPP) was higher than the OECD average in 2018 (45,935.3 PPP). Between the years 2000–2012, health expenditure in the Netherlands has continuously increased. Since 2012, a slight downward trend can be observed (The World Bank, 2020). Some indicators (e.g., the length of stay and the prescription of generic medicine) point to improvements in efficiency (Kroneman et al., 2016, p. 187). Nevertheless, healthcare expenditure is high by global comparison and amounted to 9.9% of GDP in 2018 (see Figure 2).
The Dutch Healthcare System
The Dutch government pursues three overarching objectives regarding the healthcare system: quality, accessibility and affordability (Kroneman et al., 2016, p. 187). Before describing and assessing the quality of cancer care in the Netherlands, a general description of the healthcare system is fundamental.
The Dutch Ministry of Health, Welfare and Sport is primarily responsible for healthcare and holds a regulatory role. It develops strategies and legislation to promote the health of the people and is responsible for ensuring that the three main objectives of the health system are met. The Ministry increasingly shares this responsibility with local authorities. Within the framework of service provision, there is an extensive delegation to private institutions (Kroneman et al., 2016, p. 25).
With the implementation of the health insurance reform in 2006, the Netherlands introduced compulsory insurance for the entire population in the field of curative care. Since then, the Health Insurance Act (Zorgverzekeringswet) requires all people of legal age to procure an insurance with a private health insurance company. The benefit basket is the same for all insurance companies and includes, in particular, general practitioner and hospital care, the provision of medicines, pregnancy and maternity benefits, the care of mental disorders and home nursing care. Voluntary health insurance policies can be used to ensure benefits excluded in the benefit basket (e.g., dental care).
Health insurance is financed in equal parts by a community-rated premium paid by the insured and an income-related employer’s contribution (Kroneman et al., 2016, p. 66). The premiums and employer contributions are pooled within a central health insurance fund and then, assigned to the health insurance companies, adjusted for risk. The state finances healthcare for children and young people under the age of 18 (OECD and European Observatory on Health Systems and Policies, 2017, p. 5). Service providers and health insurers negotiate the quality and price of care, with competition for quality still in its infancy (Kroneman et al., 2016, pp. 57–58).
In the context of healthcare, a distinction is made between preventive, primary, secondary and long-term care (Kroneman et al., 2016, p. 129). Public health services are the responsibility of the municipalities and include, for example, screening, vaccinations and health promotion. Population-based screening programmes exist for breast cancer, cervical cancer and colon cancer (OECD and European Observatory on Health Systems and Policies, 2017, p. 7). Participation in the screening is voluntary, and the Netherlands does not set targets for participation rates (Kroneman et al., 2016, p. 197). In well-developed primary care, a large proportion of patients (approx. 93%) are handled by general practitioners who act as gatekeepers to the healthcare system. Access to secondary care requires a referral from the general practitioner. After receiving the referral, patients have a free choice of hospital. Due to the increase in chronic diseases and multimorbidity, integrative care is gaining more and more attention (Kroneman et al., 2016, pp. 129–140).
The government has enacted various laws to ensure quality healthcare. The Health Care Inspectorate (IGZ) and the National Healthcare Institute (ZinNL) are responsible for supervising the quality of care (Kroneman et al., 2016, pp. 44–47). Quality assurance is carried out, in particular, by the service providers, sometimes in cooperation with health insurers, as well as with patients and consumer organisations. Over the past decades, many parties have worked on the implementation of quality registers. Progress has been made in the area of public reporting on the quality of healthcare outcomes, but this is still in its initial stages (Wammes et al., 2017, p. 117). This problem is currently being addressed by the ‘Outcome-based healthcare 2018–2022’ initiative of the Ministry of Health, Welfare and Sport. The aim is to make outcome indicators related to treatment transparent for 50% of the disease burden by 2022 (Ministerie van Volksgezondheid, 2018, p. 10).
Description and Evaluation of the Intermediate Objective Quality
This section provides a conceptual description of the intermediate objective of quality in a healthcare system. This is followed by a description and assessment of the quality of cancer care in the Netherlands.
Conceptual Explanation of Quality
The understanding of quality in healthcare varies across different contexts, levels of analysis and disciplines. In 1980, Avedis Donabedian made a distinction between the terms: quality and quality of care. He assumed that the quality of care goes hand in hand with the care processes and that maximizing the well-being of the patient is the goal of quality care (Busse et al., 2019, pp. 5–6).
Quality is the ability to achieve desirable objectives using legitimate means. Quality of care is the kind of care that is expected to maximize an inclusive measure of patient welfare after one has taken account of the balance of expected gains and losses that attend the process of care in all its parts. (Donabedian, 1980)
Ten years later, the Institute of Medicine (IOM, 1990, p. 21) defined the quality of healthcare as follows:
Quality of care is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.
In contrast to other definitions, the IOM definition does not exclusively focus on medical care, but on healthcare in general (including health promotion and prevention) and takes a salutogenic perspective by addressing individuals and population groups and not only patients (Busse et al., 2019, pp. 6–7).
The World Health Organization (WHO) defines the quality of healthcare according to three main dimensions: effectiveness, safety and person-centeredness. In addition, further attributes of qualitative healthcare, such as equity and efficiency are named, but these are distinguished from the core dimensions (WHO, 2018, p. 13).
For the evaluation of the quality of healthcare, the use of quality indicators is necessary. The most frequently used is Donabedian’s Triad, which differentiates between structural, process and outcome quality (Quentin et al., 2019, pp. 37–38). Donabedian (1988, p. 1745) assumes that ‘[..] a good structure increases the likelihood of good process, and a good process increases the likelihood of a good outcome’. Structures include the characteristics of the settings in which care is provided, the characteristics of resources (human and material resources) and organisational structures (e.g., organisation of medical staff). Processes are activities, which are performed when care is given and received. The effects of care on the health status of patients and population groups are defined as outcomes (Donabedian, 1988, p. 1745).
The Quality of Cancer Care in the Netherlands
Cancer care represents a challenge for the healthcare systems of OECD member states. This also applies to the Netherlands, as cancer is the leading cause of death (OECD, 2020). High quality of care is essential to effectively tackle the burden of disease caused by cancer. There are three areas of importance for ensuring high-quality cancer care (OECD, 2013, p. 12):
Resources: Medicine, personnel, institutions and equipment Practices: Access to evidence-based care, including prevention and screening Regulation and governance: National cancer control plans that include guidelines for care and monitoring, and set targets to be achieved and regulatory aspects of care (e.g., accreditation of services)
Five-year survival rates are often used to assess the quality of cancer care in a country. These reflect both the early detection of the disease and the effectiveness of treatment (OECD, 2013, p. 25). Early detection of cancer through screening and adequate treatment contributes to improved survival (van den Berg et al., 2014, p. 134).
Participation rates in mammography screening (2016: 77.3%) and colorectal cancer screening (2017: 72.7%) were relatively high in the Netherlands (Rijksinstituut voor Volksgezondheid en Milieu, 2020a, 2020c). Participation in cervical cancer screening was 56.9% in 2017, below the OECD average of 59.5% (OECD, 2020).
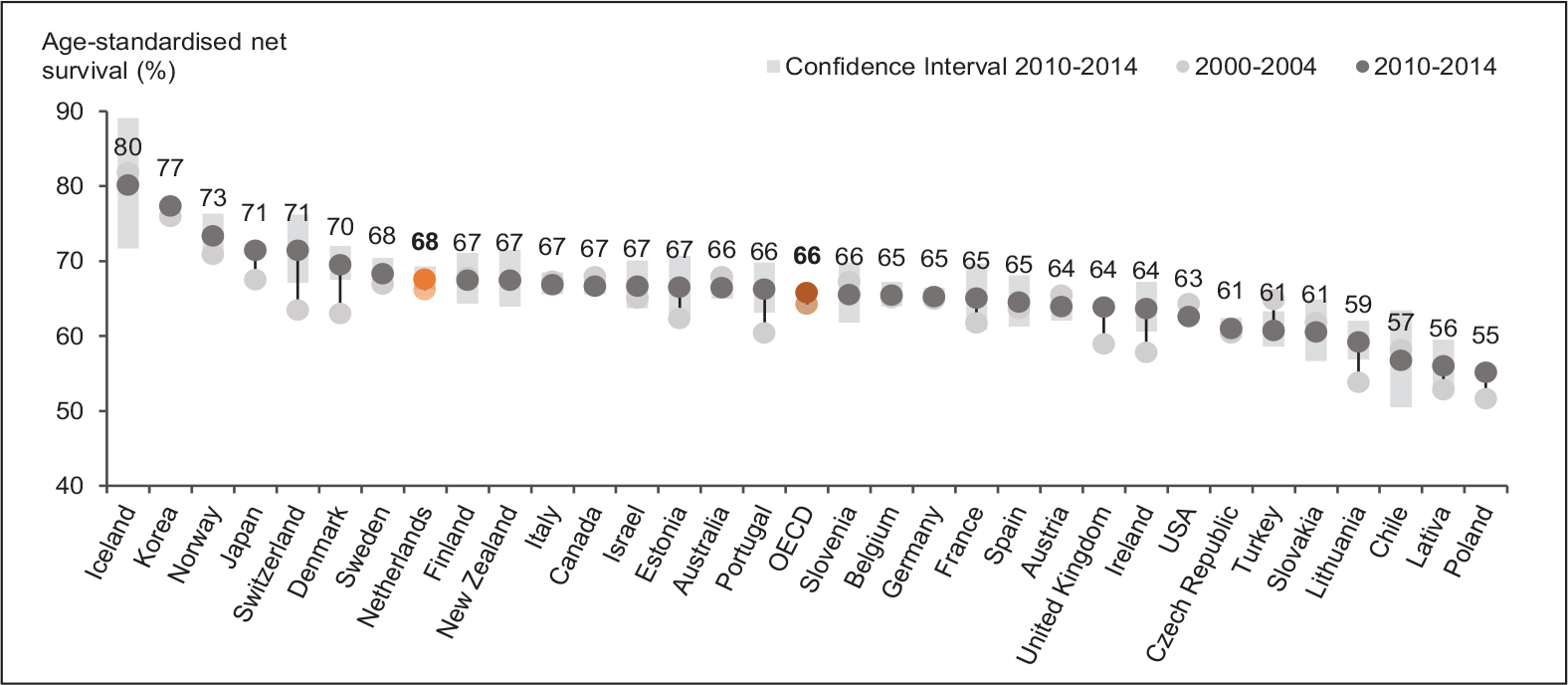
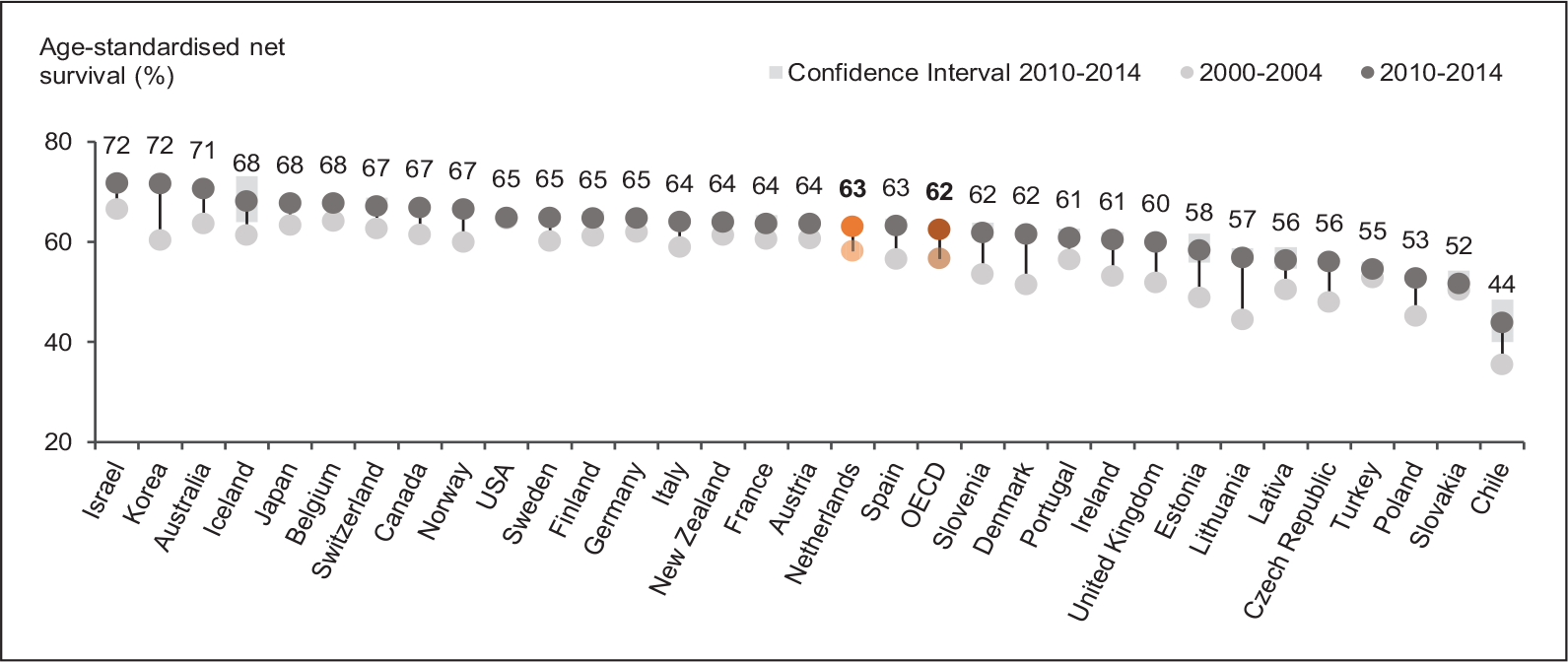
For those cancer types for which screening programmes are available in the Netherlands, the 5-year survival rates were in the upper to middle range by international standards. From 2000 to 2014, the respective survival rates slightly increased (see Figures 3–5). Figure 3 shows that the 5-year survival rate for breast cancer (87%) was slightly above the OECD average (85%). The Netherlands was also well-positioned with a survival rate of 68% for cervical cancer (OECD: 66%) (see Figure 4). The survival rate for colorectal cancer (63%) was almost in line with the OECD average (62%) (see Figure 5).
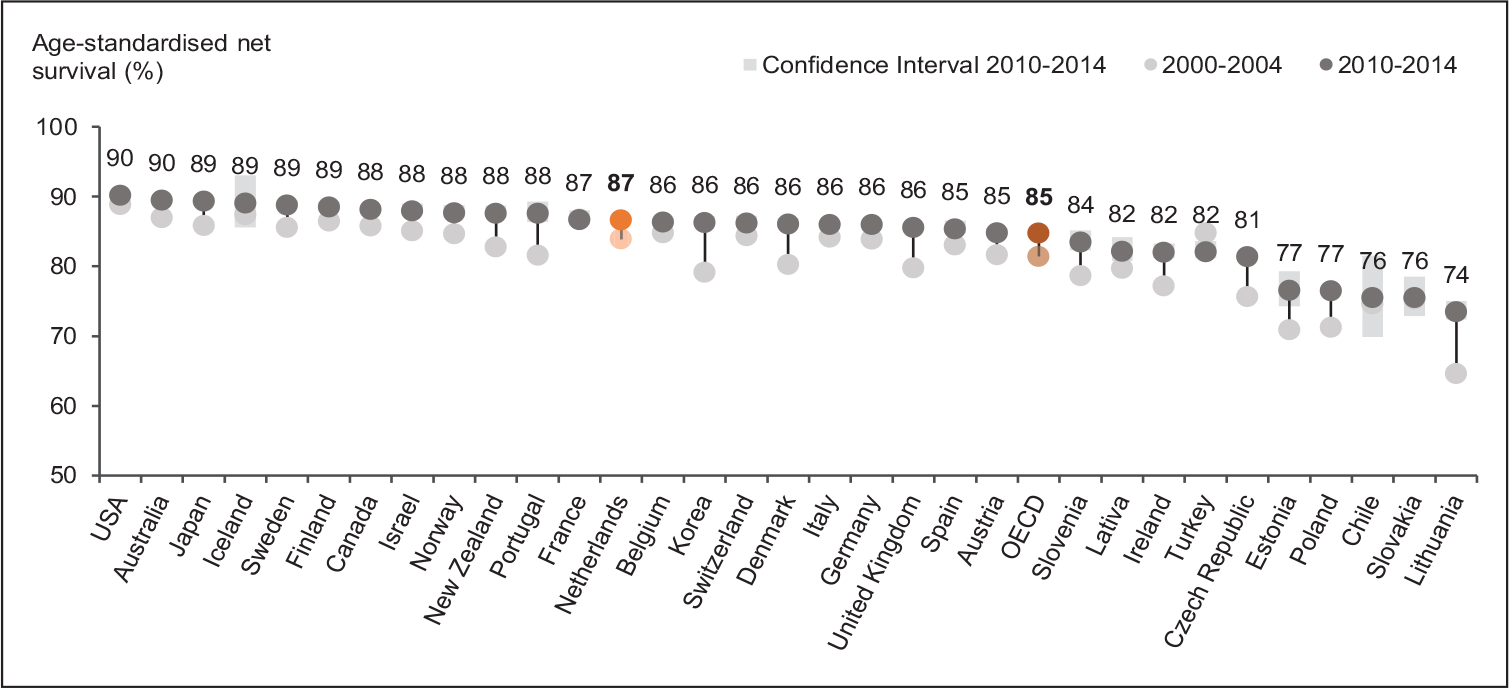
The 5-year survival for breast cancer improved by about 3% in the Netherlands between 2000 and 2014 (OECD, 2020). This is due to the screening programme that was introduced in 1990 and improved treatment. Screening is used to detect less aggressive and smaller tumours more frequently. This allows earlier treatment initiation and less invasive therapy. As a part of the treatment, improvements have been achieved in adjuvant therapies (hormonal and chemical) and surgical interventions (van den Berg et al., 2014, p. 133).
Figure 4 shows that the Dutch survival rate for cervical cancer has virtually remained unchanged from 2000-2014. The effects of treatment improvements (e.g., combined radiotherapy and hyperthermia) and the screening programme are not reflected in this figure. The confidence intervals of survival rates are relatively large due to the low incidence and mortality of cervical cancer (van den Berg et al., 2014, p. 136).
For colorectal cancer, the 5-year survival rate has increased from 58% to 63% (OECD, 2020). The improved survival is based on advances in treatment, particularly, the more frequent use of adjuvant chemotherapy. Screening for colorectal cancer was introduced in the Netherlands in 2014, and therefore, does not provide an explanatory approach (van den Berg et al., 2014, pp. 137–139).
Global comparisons show large differences in survival rates and consistent patterns of countries with stronger and weaker performance. It is reasonable to assume that these differences do not occur by chance, but rather result from systematic differences in the organization, funding and management of cancer treatment programmes (OECD & European Commission, 2013, p. 2).
National cancer control plans are an important part of quality cancer care. In the Netherlands, such a plan (National Cancer Control Programme) exists since 2004 and covers not only prevention and diagnosis but also treatment, follow-up and psychosocial care, as well as aspects of education and research (OECD, 2013, pp. 93–97). To improve the quality and coordination of care, seven regional comprehensive cancer centres (CCC) have been established in the Netherlands since 1978. The CCCs each cover an area with 5–20 hospitals and each hospital is assigned to a Centre. The Centres are responsible, among other things, for the development and implementation of guidelines, for the administration of the Netherlands Cancer Registry (NCR) and for improving the coordination of cancer and palliative care. Since 2011, they have been organised under the umbrella of the nationwide organization IKNL (Integraal Kankercentrum Nederland) (Elferink et al., 2010a, p. 75; Rijksinstituut voor Volksgezondheid en Milieu, 2020b). Since 1989, the NCR has been collecting data for all cancer patients with regard to diagnosis, tumour characteristics and initial treatment. The data are made available to policymakers (Ministry of Health, Welfare and Sport), the healthcare sector (hospitals and other health care facilities, professionals and patient organisations) and the scientific community (IKNL).
The OECD study ‘Cancer Care: Assuring Quality to Improve Survival’ compares the quality of cancer care in OECD member states in a comprehensive manner. Cancer care in the Netherlands has many positive aspects, such as the existence of population-based screening programmes, good access to care, the existence of a national cancer control plan and treatment guidelines, the accreditation of facilities and services, as well as various strategies to ensure sufficient human resources (e.g., certification systems for the training of medical personnel with expertise in cancer care and nurse practitioners in oncology). On the other hand, there are areas in which the Netherlands is positioned lower in international comparison: the time between diagnosis and the start of treatment (especially, for colorectal cancer), evaluation of the performance of the healthcare system, transparency with regard to the quality of healthcare, quality differences between hospitals and benchmarking of healthcare providers (OECD, 2013, pp. 35–108).
In addition to global comparisons, regional differences are also relevant for assessing the quality of cancer care in the Netherlands. In 2007, the Dutch Cancer Society founded a Quality of Cancer Care Taskforce to evaluate the quality of cancer care. The results of the study showed that the quality of care varies according to region and hospital. The differences between hospitals can be explained in part by the procedural volume and the type of hospital (general hospital, educational hospital for surgery or university hospital) (Wouters et al., 2010, pp. 3–10). Study results indicated that cancer patients in the Netherlands are more often treated according to current standards and have higher survival rates in university hospitals and hospitals with a high procedural volume. However, differences in the quality of care are mainly due to the variation level of individual hospitals. Since the NCR lacks relevant information on differences in the case mix between hospitals, it is not possible to adequately explain the variation. One potential reason is the fast pace with which new, evidence-based treatment strategies are introduced (Elferink et al., 2010a, pp. 74–81; 2010b, pp. 64–72; Wouters et al., 2010, pp. 3–10). According to Elferink et al. (2010b, p. 66), the regional differences result, among other things, from the fact that each CCC region treatment guideline is discussed in multidisciplinary meetings.
From the presentation of the quality of cancer care, it can be concluded that, compared to other OECD member states, the Netherlands is in the middle to upper range. Potential for improvement lies in the reduction of regional differences in the provision of cancer care above all.
Discussion
The Netherlands is interested in ensuring quality healthcare and quality is one of the three main objectives of the healthcare system (Kroneman et al., 2016, p. 187). This paper aimed to assess the quality of cancer care in the Netherlands, especially in terms of effectiveness.
Due to the decline in cardiovascular mortality, cancer is the main cause of death in the Netherlands (OECD, 2020). The Dutch healthcare system has made progress in fighting cancer by introducing population-based screening programmes and implementing treatment improvements (van den Berg et al., 2014, pp. 133–139). This is reflected in the increased 5-year survival rates (OECD, 2020). The National Cancer Control Programme, introduced in 2004, is another important element in ensuring the quality of cancer care. It takes a holistic approach by addressing issues that go beyond prevention and diagnosis (OECD, 2013, 93–97).
Since coordination is also highly relevant in the context of quality care, seven regional Comprehensive Cancer Centres have been implemented (Rijksinstituut voor Volksgezondheid en Milieu, 2020b). In addition, the Netherlands is devoting increasing attention to integrated care in order to meet the complex needs of cancer patients (OECD, 2013, p. 97). In the field of monitoring, the Netherlands Cancer Registry is an established information structure (IKNL).
The Dutch survival rates for breast, cervical and colorectal cancers were above the respective OECD averages in 2014, but some countries are better positioned. There is potential for improvement, especially regarding the survival of colorectal cancer (OECD, 2020). It should be noted that screening for colorectal cancer has only been available since 2014 (van den Berg et al., 2014, p. 139). The data on 5-year survival are from the same year. It can be assumed that the positive effect of screening will be reflected in future survival rates.
The international differences in survival rates are not random (OECD & European Commission, 2013, p. 2). The orientation towards other countries that perform better in terms of quality represents an approach to improving cancer care in the Netherlands. This includes all the above Scandinavian countries (see Figures 3–5). Participation in screening is recommended in the Netherlands, but not mandatory. No targets are set for participation rates (Kroneman et al., 2016, p. 197). Participation in screening for cervical cancer was relatively low in the Netherlands in 2017, below the OECD average (OECD, 2020). This can be increased, for example, by setting higher targets for participation rates. Another challenge is the variation in the quality of care by a region and a hospital (Wouters et al., 2010, pp. 3–10). The underlying causes have not yet been adequately identified. First, there is a need for research to identify the factors causing this variation. The next step should be focused on implications to reduce the differences.
The present analysis has some limitations. The most recent data for 5-year survival are from 2014 and are, therefore, not sufficiently up-to-date. No more recent data were found in the database analysis. The author used studies from 2010 and 2013 to describe regional differences in the quality of care. The Netherlands Cancer Registry could have been used for this subject area, but public access to the data is limited. Only nationwide survival rates are included in the Registry, regional survival data are missing. Furthermore, the comparison of survival rates is subject to limitations. Screening programmes contribute to an improvement of the survival statistics through the lead-time bias and the length-time bias. Besides, survival rates are not adapted to the tumour stage at the time of diagnosis, thus making it more difficult to evaluate the effects of screening programmes and treatment improvements (OECD, 2013, p. 25). Furthermore, a more differentiated assessment of the quality of cancer care requires the consideration of other factors, such as differences between service providers, resources for cancer care and other dimensions of quality (safety and person-centeredness).
Taking into account the limitations mentioned above, it can be concluded that the Netherlands has high-quality, effective cancer care and is striving to continuously improve it. However, there is room for improvement, especially with regard to participation in cervical cancer screening, transparency about the quality of healthcare and regional differences in the quality of care
Footnotes
Acknowledgements
I want to thank Anne Spranger for her general support during the implementation of the study. I would also like to thank Christoph Stallmann for his critical review of the manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.