
Abstract
This Commentary presents preliminary findings from an online survey of 54 breast cancer patients exploring preferences for supportive care content and delivery formats in digital health tools. Differences by age and disease stage underscore the need for personalization and cocreation in mHealth design. These insights contribute to the ongoing discussion on patient-centered digital interventions for oncology care.
Commentary
Despite the proliferation of oncology mHealth tools, little is known about how breast cancer patients’ content preferences differ by age and clinical status. Understanding these nuances is essential to design supportive digital interventions that are engaging, sustainable, and equitable.
This commentary presents exploratory, descriptive findings from a small online survey conducted to stimulate discussion on patient-centered personalization in digital supportive care, rather than to provide generalizable population-level evidence.
mHealth interventions have increasingly been adopted in oncology to support symptom management, information provision, and psychosocial well-being. While evidence on clinical effectiveness is growing, less attention has been paid to how patient preferences for supportive content may vary across age and clinical status, particularly from a user-centered perspective.
Survey design and participants
An exploratory online survey was conducted between April and June 2025 among 54 adults (≥18 years) who self-reported a diagnosis of breast cancer. Participants were recruited primarily via Instagram, with additional dissemination through X and LinkedIn. Recruitment through social media implies a digitally engaged sample and may overrepresent individuals already familiar with digital tools. The survey was descriptive and aimed to capture self-reported preferences rather than to test hypotheses or establish causal relationships. The survey explored preferred supportive care topics (e.g. nutrition, doctor-validated information, and emotional support) and preferred content delivery formats (structured lists, chatbot interaction, or both). Participants were predominantly based in Spain. No identifiable personal data were collected.
The online questionnaire consisted of 9 structured items and one optional open-ended question. Items covered five domains: (1) demographic characteristics (sex assigned at birth, age group); (2) disease-related variables (physical activity habits, disease stage/extent, treatment received [multiple selection allowed]); (3) preferred supportive care content topics (participants were instructed to select up to three predefined options; multiple selection allowed); (4) preferred information delivery format (single-choice: structured list, chatbot interaction, or both); and (5) interest in personalized content (single-choice: yes/no/maybe). All response options were predefined, except for the final optional open-text item. The questionnaire was developed by the research team for exploratory purposes and was not a previously validated instrument. The survey was administered in Spanish. The original Spanish questionnaire is provided as Supplemental Material 1, and an English translation is provided as Supplemental Material 2 for transparency.
Age group categories were defined pragmatically for descriptive purposes. While no standardized age cut-offs exist in digital health research, age-related differences in functioning and psychosocial experience across broad life stages have been documented in oncology populations, supporting the use of age as a relevant stratification variable in exploratory analyses. 1 These groupings were used to explore potential preference patterns rather than to define clinically meaningful subpopulations. Participants selected preferred content categories from a predefined list; responses were analyzed descriptively. Doctor-validated information refers to content explicitly reviewed or endorsed by healthcare professionals.
The sample comprised 54 participants, predominantly aged 46–65 years (n = 37). Most respondents reported localized disease (n = 35), while 9 reported metastatic disease; 10 participants reported remission, cured status, or no active disease (Table 1).
Sample characteristics (N = 54).

Results are presented descriptively and should be interpreted as exploratory patterns rather than statistically robust subgroup comparisons. Subgroup analyses were purely descriptive and not powered for inferential statistical testing. No statistical comparisons between subgroups were conducted.
Most participants (≈70%) reported engaging in moderate physical activity 1–3 times per week. Participants aged 46–65 more frequently selected nutrition-related content. Participants aged 18–45 more frequently selected emotional support, while those over 65 more frequently selected doctor-validated information (Figure 1). These observations represent descriptive patterns.

Descriptive distribution of reported supportive care content preferences by age group (18–45 years, n = 10; 46–65 years, n = 37; >65 years, n = 7). Results are exploratory and hypothesis-generating.
Preferences also varied by clinical status: participants with localized disease more frequently selected nutrition-related content, whereas those with metastatic disease more frequently selected practical advice and coping strategies (Figure 2). These subgroup differences are descriptive and should be interpreted cautiously.
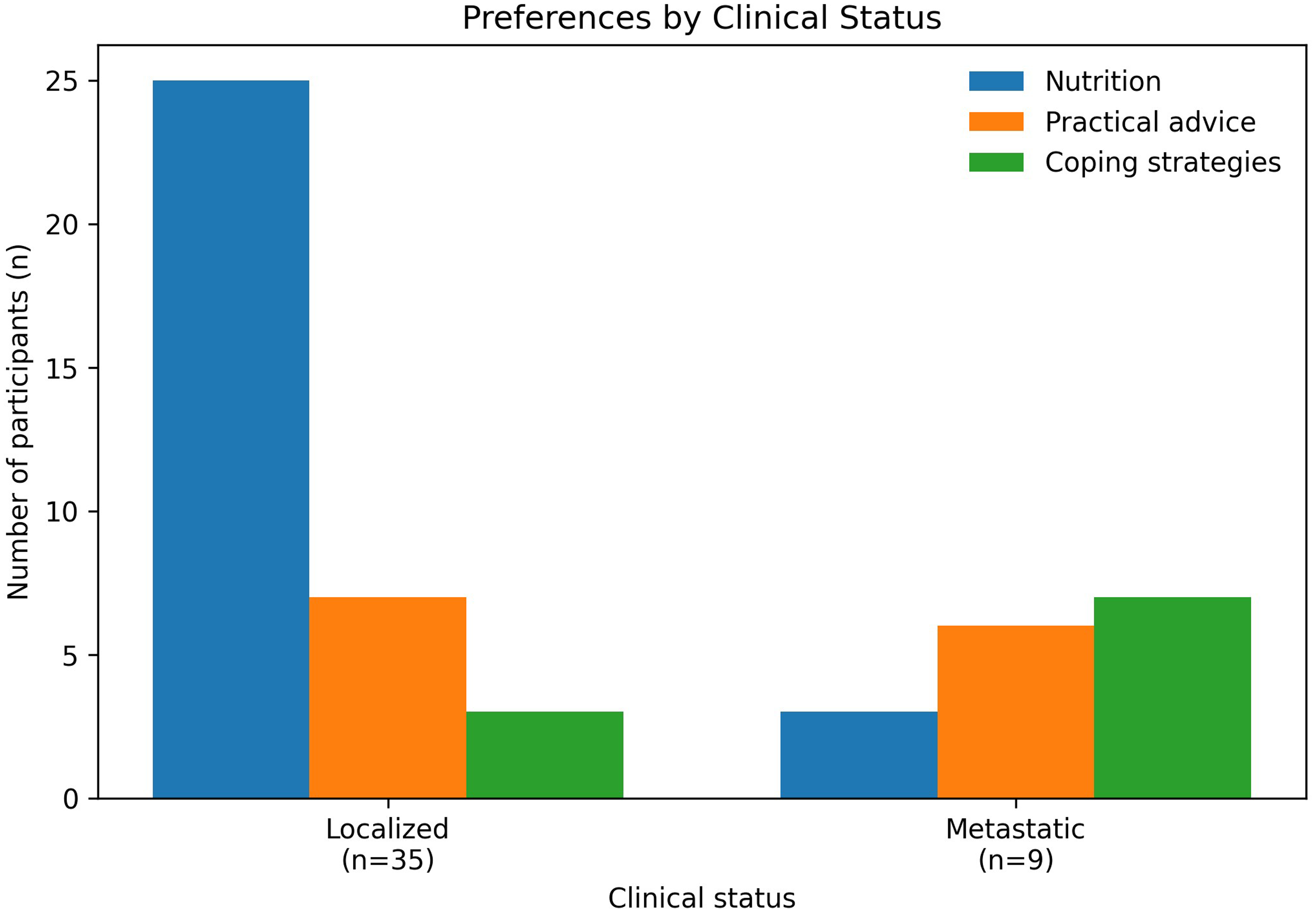
Descriptive distribution of reported supportive care content preferences by clinical status (localized disease, n = 35; metastatic disease, n = 9). Participants reporting remission/cured status were excluded from subgroup visualization due to heterogeneity. Findings should be interpreted cautiously due to the small sample size.
Regarding preferred information delivery format, 58.2% of participants preferred a combination of structured lists and chatbot interaction, 30.9% preferred structured lists only, and 10.9% selected chatbot-only interaction. Response completeness for the delivery-format item was 100% (N = 54).
A large majority (81.8%) expressed interest in receiving personalized content tailored to their clinical situation or habits, 14.5% were uncertain, and 1.8% reported no interest in personalization.
These descriptive patterns suggest that younger participants may place greater emphasis on emotional support and peer connection, which may reflect greater psychosocial and identity-related challenges earlier in the disease trajectory. In contrast, older participants expressed stronger interest in doctor-validated information, potentially reflecting preferences for clarity, reassurance, and authoritative guidance. While speculative, these patterns align with prior literature on age-related differences in digital health engagement.
From a design perspective, these exploratory findings suggest that mHealth tools for breast cancer supportive care may benefit from flexible, modular content delivery that adapts to user characteristics such as age and clinical status, rather than relying on one-size-fits-all approaches.
Our findings reinforce that breast cancer patients have diverse and evolving informational and emotional needs. This aligns with recent reviews highlighting personalization, usability, and empowerment as central to digital health design.2–4 The results also extend prior focus-group evidence underscoring usability and reliability as key patient requirements, 5 and complement a recent systematic review showing heterogeneous yet promising effects of mHealth interventions on patient-reported outcomes. 6 Together, these findings suggest that while digital tools can enhance quality of life, their long-term impact depends on systematically integrating patient perspectives and ensuring accessibility across clinical status and age groups.
In conclusion, breast cancer patients are active stakeholders with stratified, context-specific preferences. Future mHealth development should prioritize co-creation, segmentation by age and clinical status, and multi-format content delivery, avoiding one-size-fits-all approaches that risk disengagement.
Limitations
This commentary has several limitations. The small sample size and recruitment via social media limit generalizability and introduce selection bias toward digitally active individuals. Clinical characteristics were self-reported, and no validated questionnaire was used.
Although participants were instructed to select up to three content preferences, some selected additional options; all responses were retained for descriptive analysis.
Recruitment via social media likely selected for digitally engaged individuals with higher digital literacy and access to technology. This may have led to underrepresentation of older adults, individuals with limited digital skills, or those less connected to online cancer communities. Consequently, the findings may overestimate interest in digital supportive care and should be interpreted cautiously when considering implementation in routine oncology settings.
The findings should therefore be interpreted as exploratory and hypothesis-generating, intended to inform future, more robust studies rather than to support definitive conclusions.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261430085 - Supplemental material for Breast cancer patients’ preferences for digital supportive care content: Preliminary findings and future directions
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261430085 for Breast cancer patients’ preferences for digital supportive care content: Preliminary findings and future directions by María Ángeles Fuentes-Expósito, Ana Belen Rodriguez, Raquel Gomez, Montserrat Muñoz Mateu, Manuel Armayones-Ruíz and Inmaculada Grau-Corral in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076261430085 - Supplemental material for Breast cancer patients’ preferences for digital supportive care content: Preliminary findings and future directions
Supplemental material, sj-pdf-2-dhj-10.1177_20552076261430085 for Breast cancer patients’ preferences for digital supportive care content: Preliminary findings and future directions by María Ángeles Fuentes-Expósito, Ana Belen Rodriguez, Raquel Gomez, Montserrat Muñoz Mateu, Manuel Armayones-Ruíz and Inmaculada Grau-Corral in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank all participants who completed the survey and the Fundación iSYS team for technical support. With the support of the Industrial Doctorates Plan of the Department of Research and Universities of the Government of Catalonia (Generalitat de Catalunya). REF: 2024 DI 00041.
ORCID iDs
Ethics approval and consent to participate
The survey was conducted within the framework of the doctoral research project “SPARK – Smart Personalized Adaptive Re-engagement in mHealth for Breast Cancer Patients,” which received approval from the Research Ethics Committee of the Universitat Oberta de Catalunya (UOC) (Reference: CE25-TE03, approved on 13 February 2025). The present survey was covered under this approved protocol. It was anonymous, non-interventional, and collected no identifiable personal data. In accordance with institutional guidance for minimal-risk anonymous surveys, written informed consent was not required; voluntary completion of the questionnaire was considered to imply consent to participate. All procedures complied with the General Data Protection Regulation (EU) 2016/679.
Author contributions
MAF-E conceived the study, designed the survey, analyzed the data, and drafted the manuscript. MA-R and IG-C contributed to study conceptualization and critical revision. ABR, RG, and MMM contributed to clinical interpretation and manuscript review. All authors contributed to the conception, writing, and approval of the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Aggregated, de-identified data are available from the corresponding author upon reasonable request.
Guarantor
María Ángeles Fuentes-Expósito.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.