
Abstract
Stature estimation remains a cornerstone in the domain of forensic identification, particularly in scenarios involving fragmented or incomplete human remains. Conventional techniques often rely on long bones for height estimation. However, when such skeletal elements are unavailable, smaller body parts such as fingers offer a potential alternative. The index and ring fingers, owing to their relative ease of measurement and preservation, have garnered attention in anthropometric research. This study investigates the relationship between the percutaneous lengths of the index and ring fingers and the overall stature of individuals in a rural South Indian population. To assess the correlation between finger lengths and stature, and to develop sex-specific regression models for height estimation based on index and ring finger measurements among adults in Ammapettai, Tamil Nadu. This cross-sectional study included 441 participants (males and females aged 18–60 years). Stature was measured using a standard stadiometer, and finger lengths were measured with a vernier caliper. In females, a significant positive correlation was observed between stature and finger lengths, particularly the right index and left ring fingers (R² = 0.889, p < .001). Conversely, males expressed weak and statistically insignificant correlations (R² = 0.017, p > .05). Regression equations for females demonstrated high accuracy, while those for males lacked predictive reliability. Finger length serves as a strong anthropometric predictor of stature in South Indian females, supporting the creation of gender and population-specific models for forensic applications. Though the method appears ineffective for male height estimation in this population group.
Introduction
Human identification is a cornerstone of forensic science, anthropology, and clinical anatomy, particularly in scenarios involving mass disasters, unidentified remains, or incomplete human skeletal structures.1, 2 Among the various biological parameters used for establishing personal identity, stature estimation plays a critical role. It is a vital biometric characteristic that remains relatively stable throughout adult life and is often used in medico-legal investigations to reconstruct the biological profile of individuals.3, 4 Traditionally, stature has been estimated using long bones such as the femur, tibia, or humerus. However, in cases where these major bones are unavailable or fragmented due to decomposition, trauma, or taphonomic changes, alternative methods using smaller body parts become necessary. Anthropometric measurements of the hand and fingers, which are more likely to be preserved, have gained increasing importance in such contexts.5, 6 Specifically, the percutaneous lengths of the index (2nd digit) and ring (4th digit) fingers have been explored for their correlation with overall body height in various populations. 7
The use of finger length as a proxy for stature prediction is based on the principle of proportionality in human growth and development. Fingers, particularly the index and ring fingers, develop in utero under the influence of genetic and hormonal factors and have shown consistent patterns of sexual dimorphism and population variability.8, 9 Studies have suggested that finger lengths exhibit a significant positive correlation with stature, making them useful in forensic anthropology, ergonomics, and clinical assessments. 10 However, due to regional, ethnic, and genetic diversity, the applicability of standard regression equations across different populations may not yield accurate results. 11 Hence, population-specific data are essential to improve the reliability of stature estimation from finger measurements. South India, particularly Tamil Nadu, represents a genetically and culturally diverse population with unique anthropometric characteristics. 12 Despite the growing body of research in forensic and biological anthropology, there is limited literature specifically targeting the South Indian demographic, especially rural subsets like the Ammapettai population in Tamil Nadu. Localized anthropometric studies can provide valuable baseline data that can enhance the precision of medico-legal investigations and anthropological research in these regions. 13
Identification of coalesced mutilated remains is a challenge to forensic anthropologists and experts, and hence, a need for studies on the estimation of stature from various body parts in different population groups. 14 Such studies can help in narrowing down the possible victim matches in cases of identification from dismembered remains. Among the various data of identification stature of an individual is one of the most critically important data. In situations when the entire body or even skeletal remains are found, it is quite convenient to establish the stature or height of the individual.15, 16 However, in situations when dismembered or mutilated human remains are found, it becomes increasingly difficult to establish the stature. The establishment of stature in the event when dismembered or fragmented human remains are found is a significant medico-legal problem.17, 18 This study will work toward creating an effective anthropometric tool for the estimation of the approximate stature from percutaneous index and ring finger dimensions among adult males and females living in the Tiruporur taluk of Tamil Nadu. This study aims to investigate the relationship between the percutaneous lengths of the index and ring fingers and the stature of individuals in the Ammapettai region of Tamil Nadu. By analyzing these measurements in a sample of the South Indian population, the study seeks to develop regression models that can accurately predict height from finger lengths, thereby offering a simple, non-invasive, and reliable tool for stature estimation in forensic and anthropometric applications.
Materials and Methods
Study Design and Setting
This was a cross-sectional observational study conducted in Ammapettai and Nellikuppam villages in the Tiruporur Taluk of Chengalpattu district, Tamil Nadu. The study targeted adult residents between the ages of 18 and 60 years, all of South Indian descent.
Study Duration
The study spanned a period of six months, during which data collection and analysis were conducted.
Sample Size Calculation
Using the formula, n = 4PQ/L², where P = 50%, Q = 50%, and L = 5% (margin of error), a base sample size of 400 was derived. Accounting for a 10% non-response rate, the final sample included 441 participants.
Inclusion Criteria
Adults aged 18–60 years.
Residents of Ammapettai or surrounding villages.
South Indian origin.
Voluntary participation with informed consent.
Exclusion Criteria
Individuals with congenital or acquired hand deformities.
Prior surgical intervention or trauma to the hands.
Joint diseases such as arthritis.
Syndromic or dysplastic conditions affecting finger morphology.
Sampling strategy: Entire groups (clusters) are randomly selected.
Ethical Considerations
Approval was obtained from the Institutional Ethics Committee prior to commencing the study. Written informed consent was obtained from all participants.
Anthropometric Measurements
All measurements were taken by a trained examiner to reduce observer bias.
Stature
Stature was measured using a stadiometer (Figures 1A and 1B) while participants stood barefoot in an upright posture with the head positioned in the Frankfurt plane. The height was recorded to the nearest 0.1 cm.
(A and B) Measurement of Stature Using Stadiometer.

Finger Lengths
All anthropometric measurements were taken by the same examiner, and each measurement was repeated twice at different times to reduce intra-observer error. To check inter-observer reliability, a subset of 10% of participants was re-measured by a second examiner, and the values were compared using intraclass correlation coefficients. Index finger length was measured using a digital vernier caliper (Figure 2). Participants placed their right-hand palm up on a flat surface. Finger length was measured from the proximal flexion crease at the base to the tip of the finger. Measurements included both index and ring fingers of each hand and were recorded in millimeters. Ring finger length was measured similarly (Figure 3).
Measurement of the Index Finger Using a Vernier Caliper.

Measurement of Ring Finger Using Vernier Caliper.

Statistical Analysis
SPSS version 16.0 was used for data analysis. Descriptive statistics were computed. Pearson’s correlation coefficient evaluated the associations between finger lengths and stature. Multiple linear regression was applied to develop predictive models for each sex. Statistical significance was considered at p < .05.
Results
Demographics and Descriptive Statistics
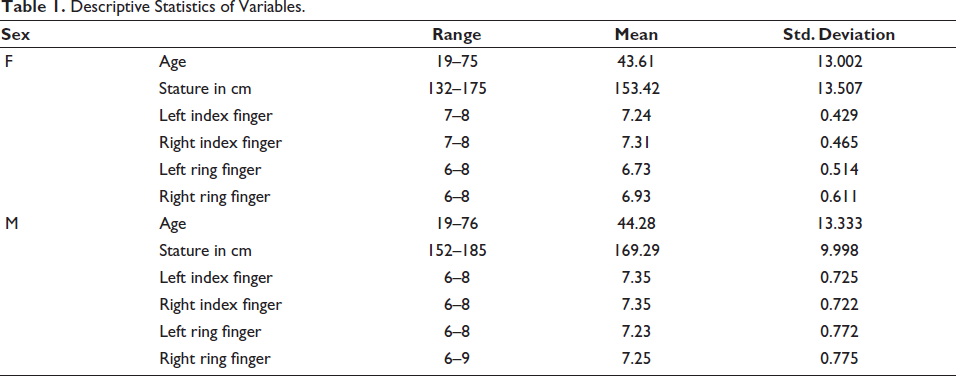
Descriptive statistics of age, stature, and finger lengths are presented in Table 1. Among the 441 participants, males were 316 and females were 125 among males had a mean stature of 169.29 ± 9.99 cm, while females averaged 153.42 ± 13.51 cm. Males also showed slightly higher finger length values compared to females, consistent with known sexual dimorphism in body proportions.
Descriptive Statistics of Variables.
Correlation Analysis
Females
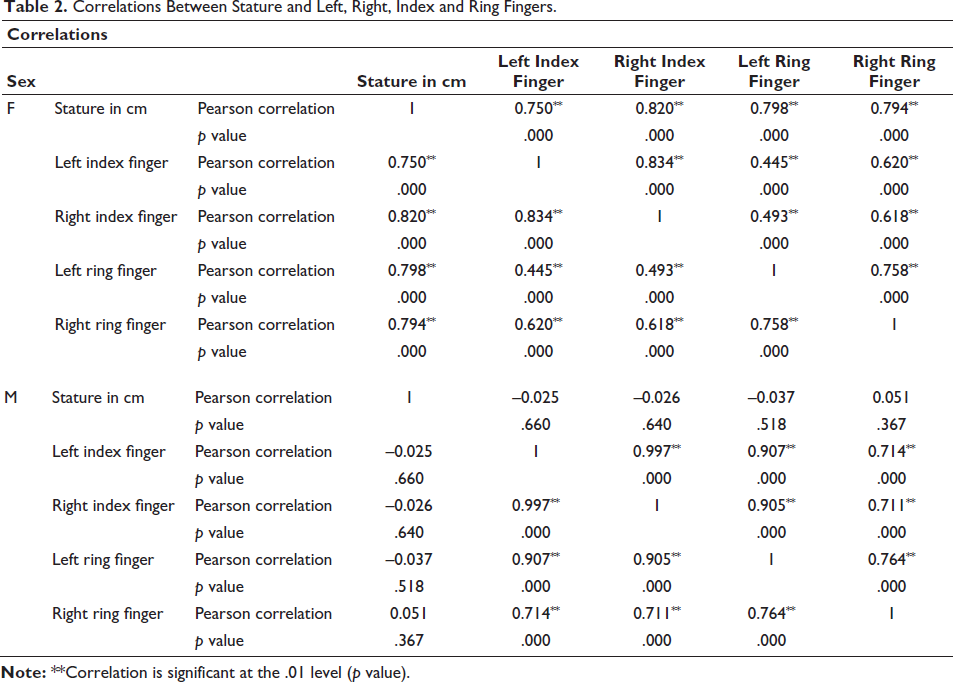
Correlation coefficients between stature and finger lengths are shown in Table 2. A strong and statistically significant correlation existed between stature and all finger lengths:
Right index finger: r = 0.820 Left ring finger: r = 0.798 Right ring finger: r = 0.794 Left index finger: r = 0.750 (p < .001 for all)
Correlations Between Stature and Left, Right, Index and Ring Fingers.
Males
Correlations were weak and non-significant:
R-values ranged from −0.037 to 0.051 All p > .05
In the present study, the key assumptions underlying linear regression—specifically, normality of residuals and linearity of relationships—were formally tested prior to model application. These assumptions are critical to ensure the validity and reliability of regression-based predictions. Failure to assess them may affect the interpretability of the regression coefficients and the accuracy of stature estimation.
Regression Models
Females
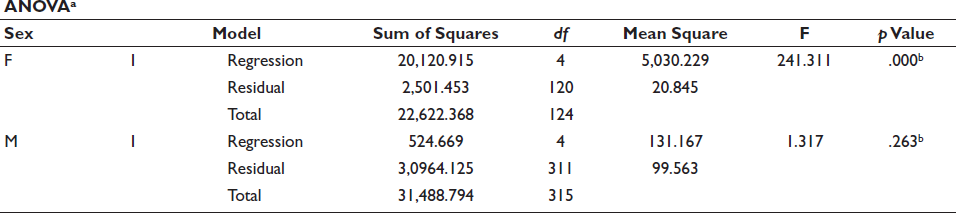
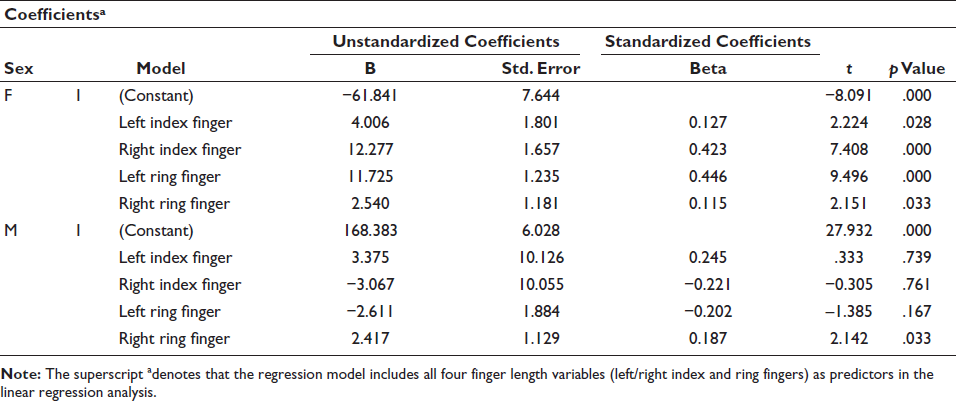
Regression model summaries and coefficients are detailed in Table 3. The multiple regression model was statistically significant and demonstrated high predictive power:
R² = 0.889 F-statistic = 241.31, p < .001 Significant predictors: Right Index Finger (B = 12.277), Left Ring Finger (B = 11.725)
Linear Regression Models Among Study Variables and Gender.

Males
The regression model lacked predictive utility:
R² = 0.017, Adjusted R² = 0.004
F-statistic = 1.317, p = .263
Only the right ring finger showed minimal statistical significance (B = 2.417, p = .033)
Discussion
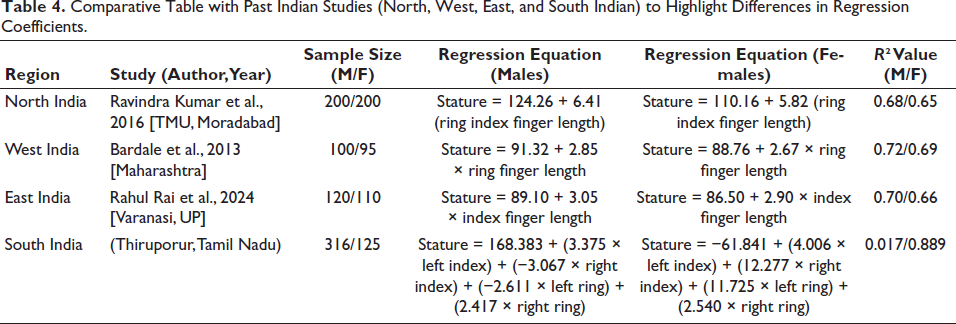
A comparative overview of regression equations across Indian populations is provided in Table 4. Anthropometric traits are known to be influenced by ethnic background, nutrition, climatic conditions, and genetic factors. 19 Tamil Nadu, particularly its rural populations, displays unique anthropometric profiles. Thus, generating localized data, as achieved in this study, fills a critical gap in regional forensic anthropology and improves the applicability of stature estimation methods in medico-legal investigations involving South Indian populations. 20 Previous studies conducted in northern and western India, as well as among tribal communities, have also reported that body proportions vary significantly across regions. Therefore, applying regression equations derived from non-local populations may lead to substantial errors. 21 The current study contributes valuable region-specific data and statistical models to aid accurate identification in forensic and archaeological. In forensic scenarios involving decomposed or mutilated bodies, where only isolated body parts such as fingers may be available, establishing an individual’s stature becomes crucial. This study offers a practical method for stature estimation from finger lengths in females, thereby aiding in narrowing down potential identities when other means of identification are unavailable. Moreover, the use of simple, non-invasive tools such as a vernier caliper and stadiometer makes this method accessible even in low-resource settings. The inclusion of both left- and right-hand measurements further enhances the method’s adaptability, especially when only one hand or partial remains are recovered.22, 23
Comparative Table with Past Indian Studies (North, West, East, and South Indian) to Highlight Differences in Regression Coefficients.
This study focused specifically on determining the predictive value of index and ring finger lengths in estimating adult stature, and whether sex-specific regression equations could be developed for reliable application in forensic settings. The mean stature for males was significantly higher than that of females, which aligns with the established sexual dimorphism seen in human populations. 24 Males also exhibited greater percutaneous finger lengths on average, which is consistent with global and regional anthropometric literature. These findings confirm the reliability of using hand dimensions to reflect general body proportions and reinforce the need to treat male and female data separately in statistical modeling. The analysis revealed a strong and statistically significant positive correlation between stature and finger lengths in females, suggesting that as the lengths of the index and ring fingers increase, so does the overall height of the individual.25, 26 This supports earlier findings from regional studies in India and other parts of Asia, which also identified hand and finger measurements as reliable predictors of stature, particularly in female subjects. In contrast, among males, the correlations between finger lengths and stature were weak and statistically insignificant. This could be due to greater variability in male body proportions or environmental and genetic influences affecting growth patterns. Another potential explanation lies in occupational factors or manual labor, which may disproportionately affect finger morphology in males from rural communities due to repetitive stress and physical activity from an early age.27, 28
Commonly, women show less variation in body proportions, making finger length a more dependable indicator of height. Estrogen endorses steady and foreseeable bone development, including finger length. In men, testosterone leads to more variability in growth patterns, which can weaken the link between finger length and stature. The index-to-ring finger ratio (2D:4D) tends to be more unchanging in females, while males show wider variation due to prenatal hormonal effects. This consistency in females supports stronger predictive models. Female height is less prejudiced by external factors like nutrition and physical activity, which often affect male growth more significantly. This stability enhances the correlation between finger length and stature. 28
Multiple regression analysis further confirmed that finger measurements are useful for stature estimation only in females. The model generated for female participants explained nearly 89% of the variance in stature (R² = 0.889), demonstrating high predictive accuracy. Notably, the right index and left ring fingers emerged as the strongest individual predictors, suggesting their utility in forensic identification. Conversely, the regression model for males had poor predictive value, with a very low R² of 0.017. Despite a statistically significant contribution from the right ring finger, the overall model lacked robustness, indicating that finger lengths alone are insufficient for stature estimation in this subgroup. These gender differences underscore the necessity of developing population- and sex-specific regression equations, as a universal model may not yield reliable results due to inherent biological and lifestyle variations.29, 30 The strong correlation between stature and finger lengths in females observed in this study is consistent with findings from Krishan et al. 31 (2015) in North India and Ilayperuma et al. 32 (2009) in Sri Lanka, where finger dimensions were also reported as reliable predictors of height. However, unlike these studies, our results did not demonstrate significant predictive value among males, which is in agreement with Rastogi et al. 33 (2008), who also found weaker correlations in male populations. Such discrepancies may reflect population-specific variations, occupational influences, or environmental factors. This study contributes region-specific regression models for stature estimation in rural South Indian females, a population group with limited published data. By establishing locally validated equations, it reduces the risk of error that arises when applying non-regional models. This enhances the utility of anthropometric methods in forensic identification within the South Indian setting
Despite its strengths, this study is not without limitations. First, the sample was limited to one rural geographical area and may not represent the entire South Indian population. Second, occupational and nutritional histories were not considered, which could have influenced finger dimensions and overall body development, particularly among males. Future research could focus on including additional anthropometric markers such as palm length, foot dimensions, or limb segment ratios to enhance the predictive accuracy for males. Additionally, expanding the sample to include urban populations or broader age groups would increase the generalizability of the findings.
Conclusion
This study established a strong and statistically significant relationship between percutaneous finger lengths and stature in South Indian females, demonstrating high predictive value. However, in males, finger lengths showed minimal correlation, limiting their utility for height estimation. The findings emphasize the importance of gender-specific anthropometric models in forensic identification. Regression equations developed from this population provide a valuable tool for stature estimation when limited body parts are available. The method is simple, non-invasive, and practical in resource-constrained settings. Future studies should explore broader populations and include additional anthropometric variables for improved accuracy.
Footnotes
Authors’ Contribution
M. Mukesh contributed to conceptualization, study design, data acquisition, medico-legal analysis, and manuscript drafting.
Dipayan Deb Barman contributed to literature review, statistical analysis, manuscript editing, and final approval of the manuscript.
Karan Kumar S contributed to case documentation and coordination of ethical compliance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was reviewed and approved by the Institutional Ethics Committee of Shri Sathya Sai Medical College and Research Institute (IEC No. 928/2024; dated 26 February 2024). The study was conducted in accordance with the ethical standards of the Declaration of Helsinki (2013 revision) and relevant national guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants or from their legal guardians, where applicable.