
Abstract
Stature estimation is an essential component of forensic anthropology, aiding in personal identification from skeletal remains. While appendicular skeleton measurements are commonly used, in cases of mutilation or trauma, alternative reliable indicators such as the foramen magnum (FM) become crucial. To determine the correlation between stature and the dimensions of the FM and to derive regression equations for stature estimation in the Western Indian population. This prospective observational study was conducted on 106 medicolegal autopsies (76 males and 30 females) in a tertiary care center in Mumbai. Cadaveric stature was measured in the supine position. Anteroposterior (AP) and transverse diameters of the FM were measured post-brain removal using vernier calipers. Data were analyzed using SPSS v17.0 to derive regression equations. Strong positive correlations were observed between FM dimensions and stature in both sexes. In males, AP and transverse lengths showed very strong correlations (R = 0.89 and R = 0.91, respectively), while in females, correlations were slightly lower (R = 0.84 and R = 0.75). Regression equations were derived for each sex. The FM offers a valuable parameter for stature estimation, especially in cases involving fragmented or mutilated remains. This study provides population-specific regression equations useful for forensic investigations in the Western Indian population.
Keywords
Introduction
Stature is one of the vital parameters in forensic analysis, useful for personal identification. Numerous methods have been employed for estimating stature from skeletal remains, using both anatomical and mathematical approaches. Previous studies suggest considerable correlations between measurements of the bones of the appendicular skeleton and stature. Even then, it is essential to ascertain regression formulas using other parts of the skeleton, because there are conditions in which the limb bones are not offered in criminal cases. 1
The possibility of survival of the basal region of the occipital bone due to mechanical trauma is greater than the other parts of skull. This could be due to maximum soft tissue covering as well as more skull thickness in this part, and its comparatively more sheltered anatomical position. Therefore, even in cases of rigorous injury, base of skull can be available intact, which can serve as an important clue in identification. 2 The foramen magnum (FM) is a significant signpost of the base of the skull and can contribute intensively to stature estimation related to identification and various anthropological studies. In spite of this, very less research work in this relation has been conducted so far in relation to stature estimation. 3
Considering the structural integrity of base of skull, this parameter can be well preserved even in cases of bomb explosions, aircraft accidents and fire tragedies.4–12 These important markers can dole out as a funnel for stature estimation. No such study has been carried out in the western part of India for stature estimation using dimensions of FM. The majority of the studies conducted on FM are for the estimation of sex of the individual.
Hence, this study is carried out to derive an influential relationship between stature of an individual and the dimensions of FM and also to discover the regression equations for the estimation of stature from FM measurements. We can expect that this study will enhance available knowledge and serve as an incitement to future researchers conducting studies in this area, and will also help forensic experts in the field of identification.
Study Objective
To determine the correlation between the stature of the individual and dimensions of FM.
To derive a regression equation for estimating stature from FM dimensions.
Material and Methods
The research study was conducted in the Department of Forensic Medicine and Toxicology in a tertiary health institution in Western India. A study was conducted on a minimum of 106 individuals, comprising 76 males and 30 females. The birthplace of the deceased will also be obtained from the relatives of the deceased.
Study Design
Prospective observational study.
Inclusion Criteria
Dead bodies of individuals above 25 years of age and individuals born and raised in the Mumbai region are brought to the post-mortem center at this hospital for medicolegal autopsies.
Exclusion Criteria
Dead bodies of people aged less than 26 years.
Decomposed, mutilated, burnt/charred bodies and those with morphological abnormalities.
Deceased with rickets or other bony diseases.
Measurement of stature was done from the vertex of the head and the heel, with cadaver placed in a supine position, with a steel measuring tape to the nearest 0.1 cm, as shown in Figure 1. After removal of brain and dura mater attached to base of skull, measurements of FM were done using vernier calipers as follows.
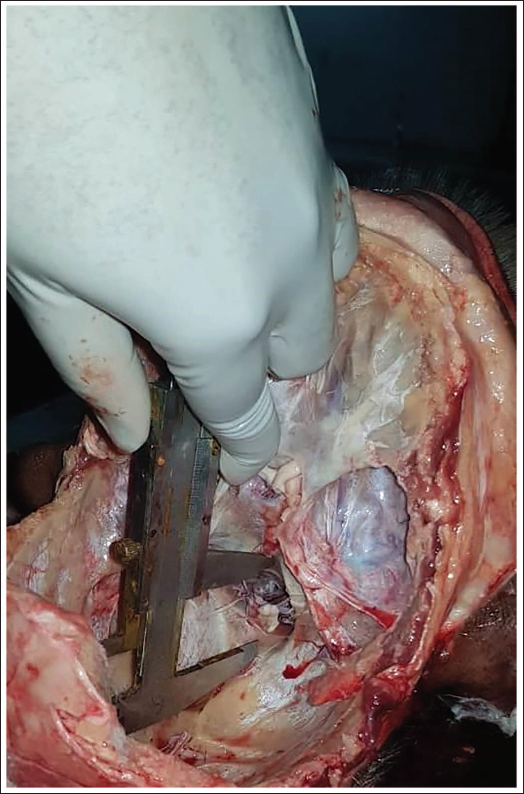
Maximum anteroposterior length (APL) along the sagittal line, that is, the distance between basion and opishthion. Basion and Opisthion are the points in the midsagittal plane intersecting the anterior margin and the posterior margin of the FM, respectively, as shown in Figure 2.
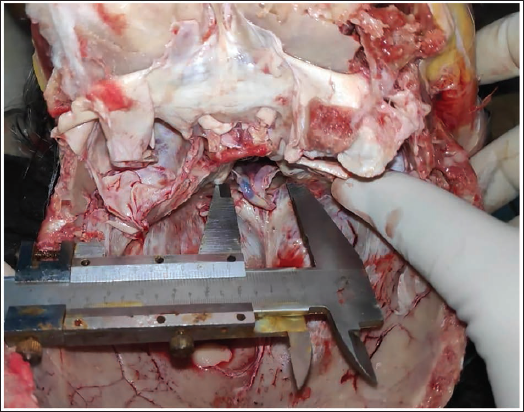
Maximum breadth or transverse length (TL) along coronal line- distance between the lateral margins of FM at the point of maximum lateral curvature as shown in Figure 3. 13
Showing Measurement of Cadaveric Length (Stature).

Showing Measurement for APL of Foramen Magnum.
Showing Measurement for TL of Foramen Magnum.
Due precaution was taken to remove soft tissues and expose the bone to prevent errors in measurements. To avoid intra-observer error, two repeated measurements were done, and the average of the two was considered for calculation. If the error is more than 0.1 mm, then a third measurement is done. 3
Analysis of data was done using SPSS for Windows v17.026 to develop a linear regression equation for stature assessment from the dimensions of FM. Also, the strength of association of stature with dimensions of FM was compared between males and females. IEC (Institutional Ethical Committee) approval was taken before starting the study.
Observation and Results
The present study was carried out in the Department of Forensic Medicine and Toxicology, a tertiary care hospital in western India. Total of 106 cases were studied for the estimation of stature from the dimensions of FM. Out of the total cases, 76 (71.7%) cases were of males, while 30 (28.3%) cases were of females.
The maximum number of cases was between ages 26 and 40 years in males and females, while the lowest numbers of cases were in age groups older than 70 years.
Descriptive statistical analysis of the Dimensions of FM in cadavers in relation to stature in females is as follows:
Stature in females ranged from 147 cm to 172 cm, with a mean (±SD) was 155.93 cm (±7.99 cm), and a 95% confidence interval of the mean was ±2.982. The mean APL of FM was 3.17 cm and (±SD) was (±0.37), ranging from 2.8 cm to 3.9 cm, while the 95% confidence interval of the mean was ±0.139. The mean TL of FM was 2.75 cm and (±SD) was (±0.26), ranging from 2.5 cm to 3.4 cm, while the 95% confidence interval of the mean was ±0.098.
Descriptive statistical analysis of the Dimensions of FM in cadavers in relation to stature in males. It is as follows:
Cadaveric length (stature) in males ranged from 147 cm to 180 cm, with a mean (±SD) was 164.24 cm (±7.66 cm) and a 95% confidence interval of the mean was ±1.750. The mean APL of FM was 3.39 cm and (±SD) was (±0.42), ranging from 2.8 cm to 4.2 cm, while the 95% confidence interval of the mean was ±0.095. The mean TL of FM was 2.91 cm and (±SD) was (±0.22), ranging from 2.5 cm to 3.3 cm, while the 95% confidence interval of the mean was ±0.051.
A simple regression formula was obtained to estimate stature from the dimensions of FM in males and females (Table 1). Strength of correlation for the dimensions of FM with Stature varies between males and females. The strength of correlation varies from moderate positive correlation to very strong positive correlation. Correlation coefficient or Pearson coefficient value (R) for Females was 0.84 and 0.75 for AP length and TL of FM, while it was 0.91 and 0.64 for AP length.
Detailed Regression Statistics Showing Correlation of Dimensions of Foramen Magnum in Males and Females.

Similarly, the R value in males was 0.89 and 0.91 for APL and TL of FM, while it was 0.89 and 0.75 for APL.
Overall, the strength of correlation was better in males compared to females.
In males, a very strong positive correlation was observed with TL of FM, while the other three dimensions showed a strong positive correlation.
Both the dimensions of FM showed a strong positive correlation with the cadaveric length. The standard error of estimate for females was 4.47 and 5.42 for AP length and TL of FM.
Similarly, the R value in males was 3.57 and 3.14 for AP length and TL of FM.
Discussion
The number of cases in the present study was almost similar to Gruber et al. (2009) (03), Radhakrishna et al. 14 and Ukoha et al., 15 while the method, that is, on medicolegal autopsy, was similar to Babu et al. 16
Distribution of the Stature of Male and Female
As per Table 2, Stature in females ranged from 147 cm to 172 cm, with a mean (±SD) was 155.93 cm (±7.99 cm) and a 95% confidence interval of the mean was ±2.982. As per Table 3, Stature in males ranged from 147 cm to 180 cm, with a mean (±SD) was 164.24 cm (±7.66 cm), and a 95% confidence interval of the mean was ±1.750.
Comparison of APL and TL of Foramen Magnum with Other Studies in Males.
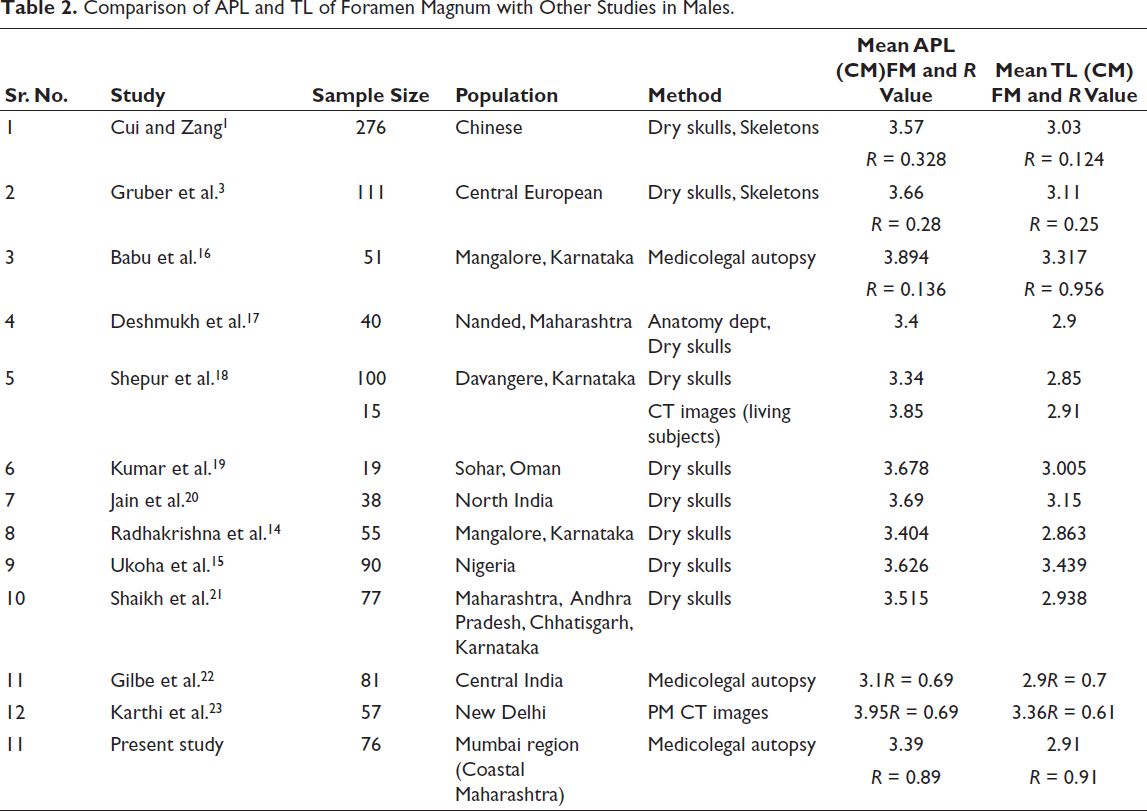
The above findings were almost similar to Cui and Zang’s 1 study in China, which showed the mean stature of the cadaver was 165.22 cm in North Chinese males and 161.01 cm in South Chinese males. Babu et al. 16 stated the mean stature of the population of Mangalore as 166.66 cm in males, which is almost similar to the present study.
Distribution of APL and TL of FM of Males
The mean APL of FM was 3.39 cm and (±SD) was (±0.42), ranging from 2.8 cm to 4.2 cm, while the 95% confidence interval of the mean was ±0.095. The mean TL of FM was 2.91 cm and (±SD) was (±0.22), ranging from 2.5 cm to 3.3 cm, while the 95% confidence interval of the mean was ±0.051 as given in Table 3.
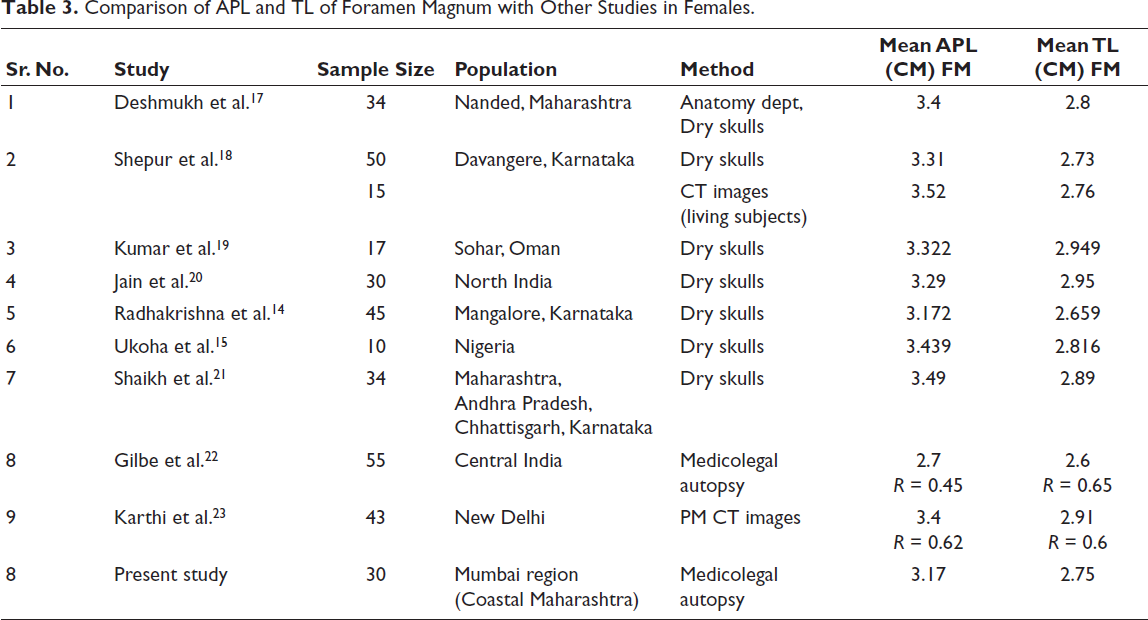
Comparison of APL and TL of Foramen Magnum with Other Studies in Females.
Mean APL of FM in males in the present study were in accordance with studies of Deshmukh et al., 17 Shepur et al., 18 (dry skulls study) and Radhakrishna et al. 14 While it was slightly on the lower side as compared to the findings of Shaikh et al. 21
Similarly, findings obtained in the present study of mean APL of FM in males were not consistent with the studies of Gruber et al., 3 Babu et al., 16 Shepur et al. 18 (CT Images Living subjects), Kumar et al., 19 Jain et al., 20 Cui and Zang, 1 Gilbe et al., 22 Karthi et al., 23 and Ukoha et al. 15
Differences in the findings of various studies could be due to environmental variations, genetic differences and nutritional factors, as the study conducted by Gruber et al. was done in central Europe, Cui and Zang 1 in China, Babu et al. 16 in Mangalore, Karnataka, Kumar et al. 19 in Oman, Jain et al. 20 in North India and Ukoha et al. 15 in Nigeria. A study conducted by Shepur et al. 18 was done on Living subjects by Computed Tomography examination could be a factor responsible for the difference in findings, as in the same study conducted on dry skulls, findings obtained match with the findings in the present study.
Mean TL of FM in males in the present study were in accordance with studies of Deshmukh et al., 17 Gilbe et al. 22 and Shepur et al. 18 (CT images study). While it was more or less similar to findings of Radhakrishna et al., 14 Shepur et al. 18 (dry skulls), and Shaikh et al. 21
Similarly, findings obtained in present study of mean TL of FM in males were not consistent with the studies of Cui and Zang, 1 Gruber et al., 3 YP Raghavendra Babu et al., 16 Kumar et al., 19 Jain et al., 20 Karthi et al., 23 and Ukoha et al. 15 Difference in the findings with various studies could be due variations in environmental conditions, genetic, nutritional factors and difference in sample size.
In the current study R value in Males for APL and TL of FM was 0.89 and 0.91. Both the dimensions had having strong positive correlation with stature, but the TL had having more strong positive correlation with stature as compared to the APL. In a study done by Gruber et al., 3 sagittal (R = 0.28) and transverse diameters (R = 0.25) and in a study performed by Cui and Zang, 1 with R values for APL and TL is 0.328 and 0.124, showed weak correlation with stature. Both the dimensions in both the studies had having very weak positive correlation, which is inconsistent with the present study. Also, the sagittal diameter had having slightly better correlation than the transverse diameter, which is also not consistent with the present study.
Similarly, in the YP Raghavendra Babu et al. 16 study, R value for APL and TL of FM was 0.136 and 0.956. TL was showing a strong positive correlation, while APL was showing a very weak positive correlation with stature. This shows that only TL of FM can be used as a reliable indicator for stature estimation, which is partly compatible with our study, where both dimensions were strongly positive. A study done by Gilbe et al. 22 showed a moderately positive correlation, where TL had having better correlation compared to AP length, which is opposite to the study done by Karthi et al. 23
The mean APL of FM was 3.17 cm and (±SD) was (±0.37), ranging from 2.8 cm to 3.9 cm, while the 95% confidence interval of the mean was ±0.139. The mean TL of FM was 2.75 cm and (±SD) was (±0.26), ranging from 2.5 cm to 3.4 cm, while the 95% confidence interval of the mean was ±0.098 as given in Table 3.
Mean APL of FM in females in the present study were exactly similar to the study of Radhakrishna et al. 14 While it does not match with the rest of the studies. Differences in the findings of various studies could be due to environmental variations, genetic differences and nutritional factors and differences in sample size.
Mean TL of FM in females in the current study were in agreement with studies of Shepur et al. 18 While it was slightly less compared to findings of Deshmukh et al. 17 and Ukoha et al. 15
Similarly, findings obtained in present study of mean TL of FM in females were inconsistent with the studies of Cui and Zang 1 Gruber et al., 3 Babu et al., 16 Kumar et al., 19 Jain et al., 20 Radhakrishna et al., 14 Gilbe et al., 22 Karthi et al., 23 and Shaikh et al. 21 Difference in the findings with various studies could be due variations in environmental conditions, genetic, nutritional factors and difference in sample size.
Limitations of the Study
In the current study, the sample size was restricted, especially in the case of females. Therefore, stature estimation from FM dimensions to be carried out with vigilance. The current study will be applicable for stature estimation from FM dimensions in the population of coastal Maharashtra and cannot be loosely used for the pan-India population. The utility of the current study for stature estimation is constrained to mutilated remains for autopsy and to be used with skeletal remains with caution.
Conclusion
Although the appendicular skeleton is conventionally used for stature estimation, forensic situations often present only fragmented remains. The FM, owing to its anatomical protection and high survival rate even in mutilating trauma, offers a robust parameter. However, its potential remains underexplored in the Indian context, particularly in the Western coastal population. “This study demonstrates that the FM, especially its transverse diameter, can be a reliable parameter for stature estimation in forensic cases where traditional bones may be unavailable.” The strong correlation, particularly in males, supports its use in medicolegal identification in Western Indian populations. Further studies with larger, more diverse populations and advanced imaging can help refine these findings for broader forensic application.
Footnotes
Abbreviations
APL: Anteroposterior length
TL: Transverse length
FM: Foramen magnum
Authors Undertaking
We confirm that the information provided above is correct. I/We confirm that I/we have contributed sufficiently as per the ICMJE guidelines to be eligible for authorship in the submission made to IJME, and state that I/each of us am/is equally responsible and accountable for the entire content of the submission. We also state that the submission is our original work and is free of plagiarism of any kind.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
The ethical approval has been obtained by the Institutional Ethics Committee at the author’s institution (Seth G.S. Medical College and KEM Hospital, Mumbai), approval letter no IEC (II)/OUT/1118/18 dated 27/11/2018.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.