
Abstract
This study assessed the potential of the foramen magnum (FM) in the Malaysian juvenile population to estimate sex using computed tomography (CT) data. A total of 200 (male = 100; female = 100) CT images of Malaysian individuals aged between 8 and 16 were retrieved. The maximum length (FML) and width (FMW), area (FMA 1 and FMA 2), and index (FMI) of the three-dimensional image of the FM were measured and analysed using Mimics software version 20 (Materialise N.V., Heverlee, Belgium). These metric data were then used to develop sex estimation models through discriminant function analysis (DFA) and binary logistic regression (BLR). The results showed that all measurements in males were significantly higher than in females (p < 0.001), demonstrating a high potential for accurate sex classification. Additionally, females exhibited a wider FM than males, as indicated by the FM index. Based on univariate DFA analysis, FML and FMA 2 were identified as reliable variables for sex estimation, achieving an accuracy of 68.5% with a low sex bias rate of 1.2%. The multivariate DFA yielded a higher accuracy of 70.5% compared to the univariate analysis. Similarly, univariate and multivariate BLR analyses demonstrated comparable accuracies of 68.5%. Overall, the DFA showed greater accuracy and lower sex bias across all cases, including original and validation samples. This study suggests that FM parameters can complement existing sex estimation methods and be integrated with other techniques to improve skeletal sex determination.
Keywords
Introduction
The study of anthropometric characteristics is vital in the field of forensics, particularly in resolving identification and documentation issues. The pelvis is preferable for sex estimation, followed by the skull and other postcranial bones. However, it was reported that the skull is reliable to be used after puberty. 1 The skull, characterised by the presence of the foramen magnum (FM),2–4 is the most sexually dimorphic part of the human skeleton. 5 FM is found in the median plane of the cranial cavity, with the largest circular opening in the occipital bone. This structure is in a well-protected anatomical position and shapes the base of the skull. 6 Furthermore, this foramen is a component of the posterior cranial fossa, linking the cranial base, the skull's foundation, and the vertebral canal. 7
FM reaches mature development relatively early in childhood. 8 Thus, it has been postulated that this structure is less likely to undergo significant secondary sexual changes, leading to sexual dimorphism. Moreover, FM measurements are useful when dealing with cases where only a fragment of the skull base can be assessed following population-specific standards. 1 Examining the morphology and morphometrics of the FM yields valuable insights for accurate sex prediction (>70%).4,9,10 Previous studies on adult sex estimation using FM measurements have been widely conducted in Saudi Arabian,6,11 European, 12 Turkish, 13 Egyptian,4,14 Iraqi, 3 Iranian, 15 Indian16,17 and Nepalese population. 18 To date, most research conducted on Malaysians has primarily focused on the adult population, with limited attention given to the juvenile population.19,20 This highlights the importance of further exploration into sex estimation using FM measurements in Malaysian juveniles.
The cranial base and FM remain intact over long periods due to their thickness and well-protected position, while other parts of the skull are more vulnerable to decomposition. 5 Moreover, the skull base is protected by an extensive soft-tissue mass comprising muscles, ligaments, and cartilage. 21 This protective layer allows FM to withstand external threats (explosions, fires), whereas the vulnerable facial regions are easily damaged. 21 FM is surrounded by four key components of the occipital bone (posteriorly located supra-occipital part of the squama, anterior basilar, and two lateral parts on either side of the skull) 22 and connected via the symmetrical posterior and anterior intraoccipital synchondroses. The posterior synchondroses fuse at 2–4 years old 23 and the anterior synchondroses develop simultaneously up to age 5–7. 24 Therefore, an individual is less likely to undergo significant changes in the FM region following secondary sexual changes. 12
Medicolegal investigation uses morphological and morphometric approaches to perform sex estimation. Nevertheless, morphometric techniques offer distinct advantages due to the objective quantification of sexual dimorphism in bone dimensions, including various measurements, indices, discriminant function analysis (DFA), and binary logistic regression (BLR).25,26 Meanwhile, morphological analysis is observer-dependent and possibly less reliable, particularly in fragmented skull cases. 27 The development of imaging techniques, such as computed tomography (CT), has been impactful in forensic research. 28 Recent studies have highlighted the potential of CT as a diagnostic instrument in forensic research for sex and age estimation.26,28 The aim of this study was to estimate sex in the Malaysian juvenile population using measurements of the FM obtained from CT data.
Materials and methods
Ethics approval was granted by the Medical Research Ethics Committee of the University Malaya Medical Centre (MREC ID No: 202147-10039). The inclusion criteria for this study were high-quality reconstructed images, individuals of Malaysian nationality, and an age range between 8 and 16 years. The exclusion criteria included non-Malaysians, low-quality images (e.g., blurring, artefacts, or incomplete FM scans), and scans of individuals with a history of trauma, surgery, or other pathological lesions (congenital or acquired) in the skull base region. An initial total of 250 multi-slice computed tomography (MSCT) scans (125 males and 125 females) were initially obtained for this study, with the original scans acquired between 2015 and 2022. However, 50 scans were excluded based on the predefined exclusion criteria. Finally, 200 MSCT skull images of individuals aged between 8 and 16 years (100 males and 100 females) were retrospectively obtained from the Oral Radiology Unit database at the University of Malaya Medical Centre (UMMC), Kuala Lumpur, Malaysia. Data collection for the MSCT scans was conducted between 2021 and 2022. These scans were originally performed for various clinical indications, including trauma assessment, surgical cases, evaluation of congenital or developmental conditions, infections, and other diagnostic purposes involving the craniofacial region. The scanning protocol was as follows: detector configuration = 32 × 0.5 mm, 0.75–1 mm slice thickness, tube voltage = 120 kV, tube current = 120 mA, and exposure time = 0.5 s. Subsequently, a high spatial frequency reconstruction algorithm was applied to reconstruct the images.
Measurements
DICOM-formatted CT images were stored and subsequently reconstructed using 3D image segmentation software, Mimics V20.0 (Materialise, Heverlee, Belgium). The maximum length (FML), width (FMW), area (FMA), and index (FMI) of the FM 3D image were measured and analysed. The FML and FMW were assessed on axial cross-sections parallel to the foramen plane from optimal images to ensure that the maximum distances could be accurately measured. The maximum FML was obtained by measuring the principal axis in the anteroposterior direction. The FMW, perpendicular to the FML, was measured at the widest transverse diameter (see Figure 1). The FMA was determined based on the FML and FMW using two formulas. The first formula, denoted as FMA 1, employs a method suggested by Radinsky: 29 ¼ × π × length × width. The second formula, designated as FMA 2, utilised an approach developed by Teixeira: 30 π [(length × width)/4]2. Finally, the FMI was computed using the FML and FMW as follows: FMI = (FMW/FML) × 100. Then, the FM shape was categorised based on the FMI values as follows: narrow (<81.9), medium (82.0–85.9), or wide (>86.0). 31
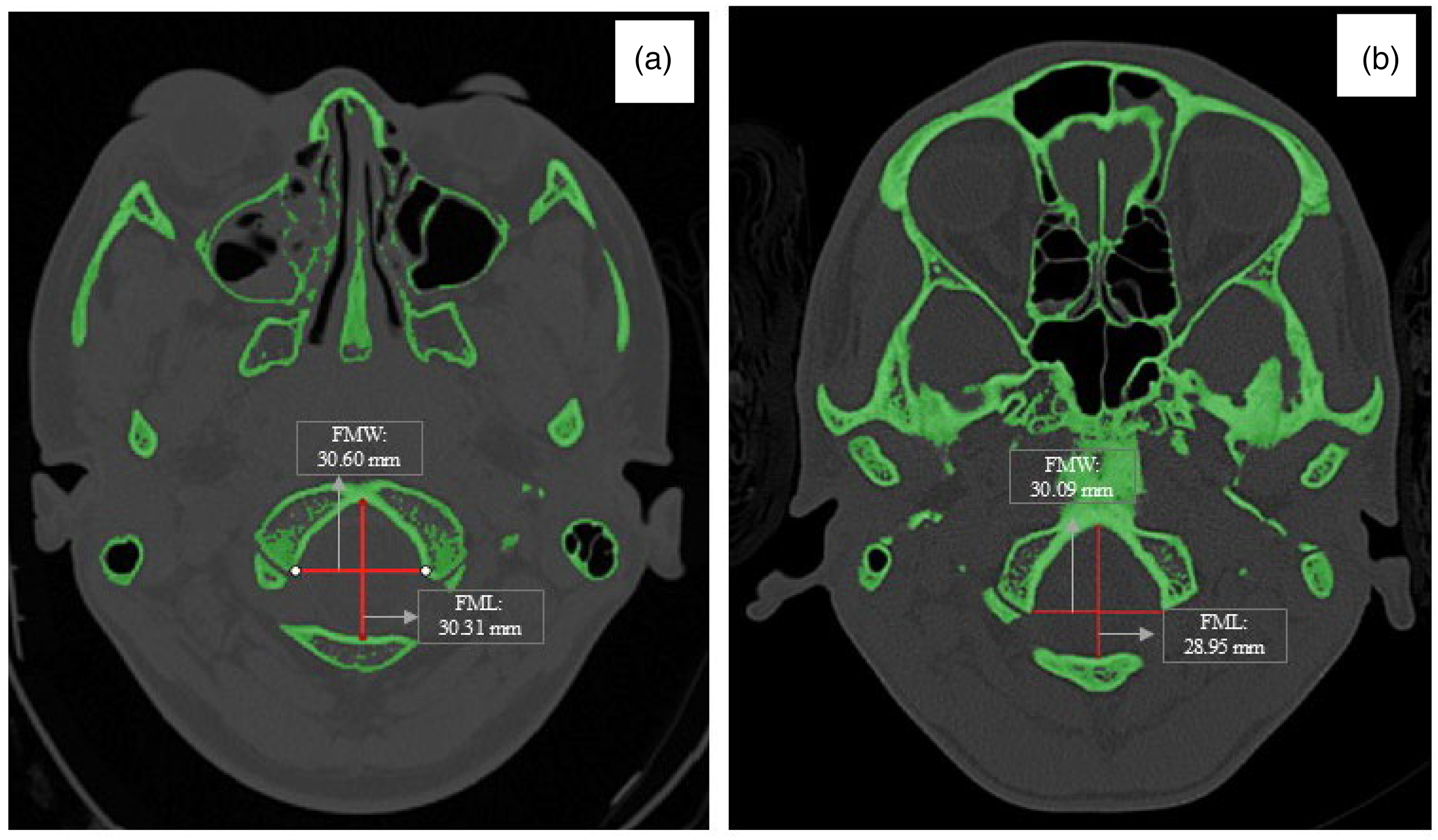
The length and width of the foramen magnum on axial cross-sectional view: (a) male, 14 years; (b) female, 12 years.
Statistical analysis
The data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 26.0 (IBM, USA). Firstly, the Kolmogorov–Smirnov test was performed to determine if the data demonstrated a normal distribution. After the normality of the data distribution was confirmed, an independent-sample t-test was conducted to identify the differences in FM measurements between sexes. The numerical data were expressed as minimum and maximum values and mean ± standard deviation (SD). Pearson's correlation analysis was also performed to assess the strength and direction of the relationships between the FM measurements. The significance level was set at p < 0.001. The correlation strengths were classified following an earlier study 32 : very weak = 0.00–0.19, weak = 0.20–0.39, moderate = 0.40–0.59, strong = 0.60–0.79, and very strong = 0.80–1.00. A positive absolute correlation coefficient indicated a positive correlation, while a negative value represented a negative correlation.
The technical error of measurement (TEM), relative TEM (rTEM), and reliability coefficient (R) were calculated to assess the reliability of intraobserver and interobserver measurements. A total of 50 MSCT scans were used to assess intraobserver reliability through repeated measurements by the primary investigator, while interobserver reliability was evaluated by an experienced oral and maxillofacial radiologist with over 9 years of clinical experience.
All FM measurements were fitted in univariate and stepwise multivariate DFA to establish a sex prediction model. Initially, the centroids of the sectioning point for all generated discriminant functions were set at 0 in the male and female groups. A value of >0 is representative of the female sex, while a score of <0 for the discriminant function is indicative of the male sex. A cross-validation procedure that was leave-one-out classification was conducted. Then, the BLR analysis was performed to construct the sex estimation model. The cut-off value was set at 0.5; a predicted value of >0.5 was associated with males, whereas a value of <0.5 was indicative of females. Finally, the classification accuracy rates of the univariate and multivariate BLR models were determined.
Results
The descriptive statistics for the FM measurements were summarised in Table 1. The findings showed that all measurements in the male group were significantly higher than the female group (p < 0.001). FMI values demonstrated various shapes of FM in male and female skulls (see Figure 2). The higher FMI in the male group indicated that their FM was relatively longer than females, thus demonstrating a narrower foramen. In contrast, females often demonstrate wider FM due to their lower FMI values.
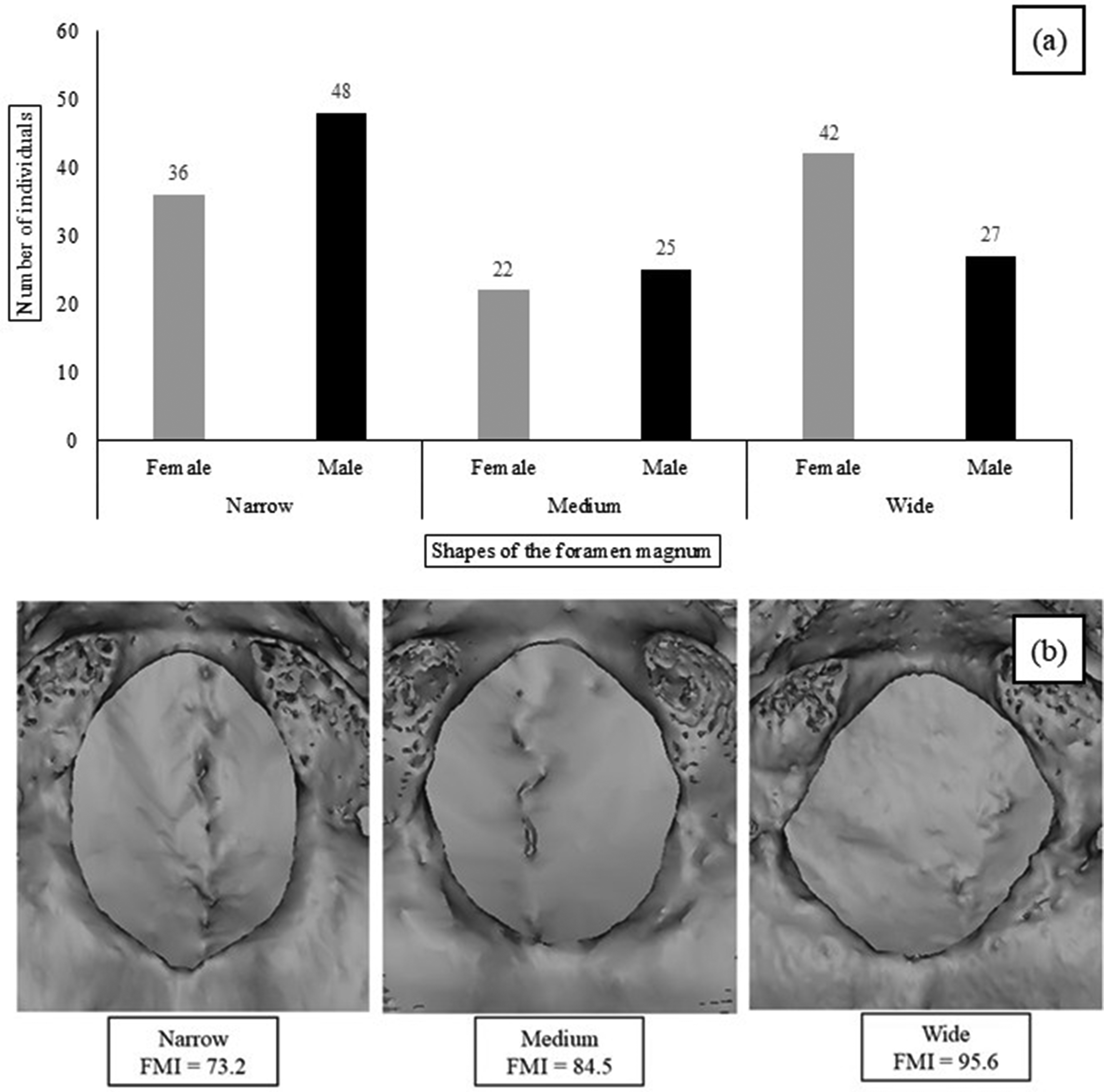
(a) Distribution of foramen magnum shapes in Malaysian males and females; (b) Foramen magnum shapes based on the foramen magnum index (FMI).
Comparison of foramen magnum parameters among male and female groups.
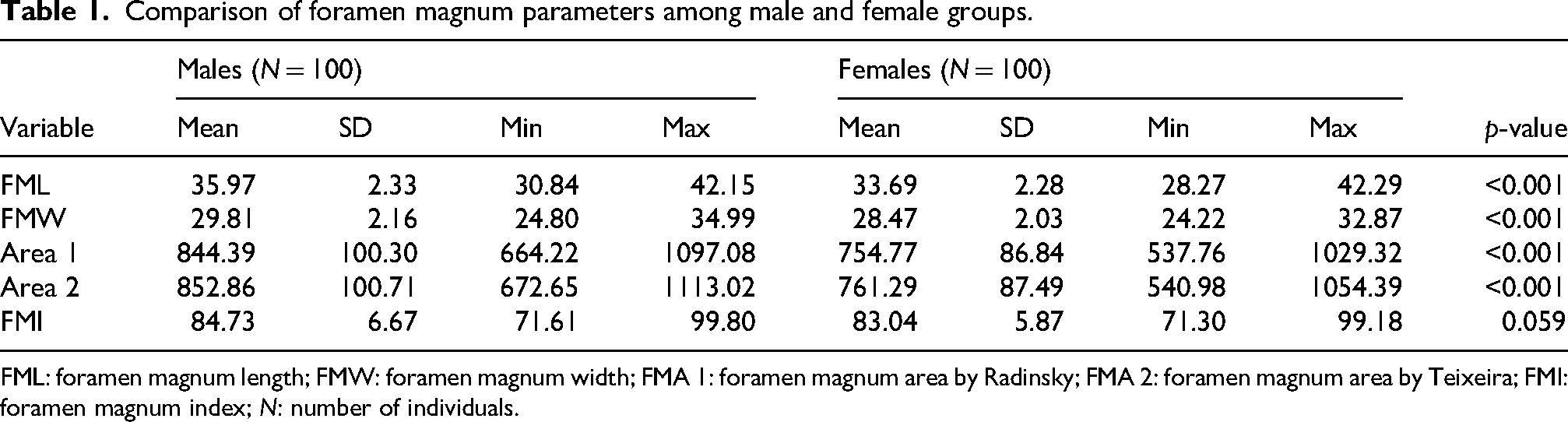
FML: foramen magnum length; FMW: foramen magnum width; FMA 1: foramen magnum area by Radinsky; FMA 2: foramen magnum area by Teixeira; FMI: foramen magnum index; N: number of individuals.
Pearson's correlation analysis indicated significant and positive correlations between most FM measurements and sex, except for the FMI (see Table 2). The most robust correlation was recorded between Areas 2 and 1 for males and females (r = 0.998 and 0.998), respectively. Conversely, the weakest correlations were between FMI and Area 2 (r = 0.071 and 0.004), followed by FMI and Area 1 (r = 0.124 and 0.060) in the male and female groups, respectively. The TEM, rTEM, and R values for intraobserver error were 0.21, 0.09%, and 0.89 for FML and 0.11, 0.21%, and 0.91 for FMW, respectively. For interobserver error, the corresponding values for FML were 0.31, 0.11%, and 0.87, and for FMW, were 0.21, 0.26%, and 0.88, respectively.
Correlations between FM measurements in males (lower left corner of the table) and females (upper right corner of the table).
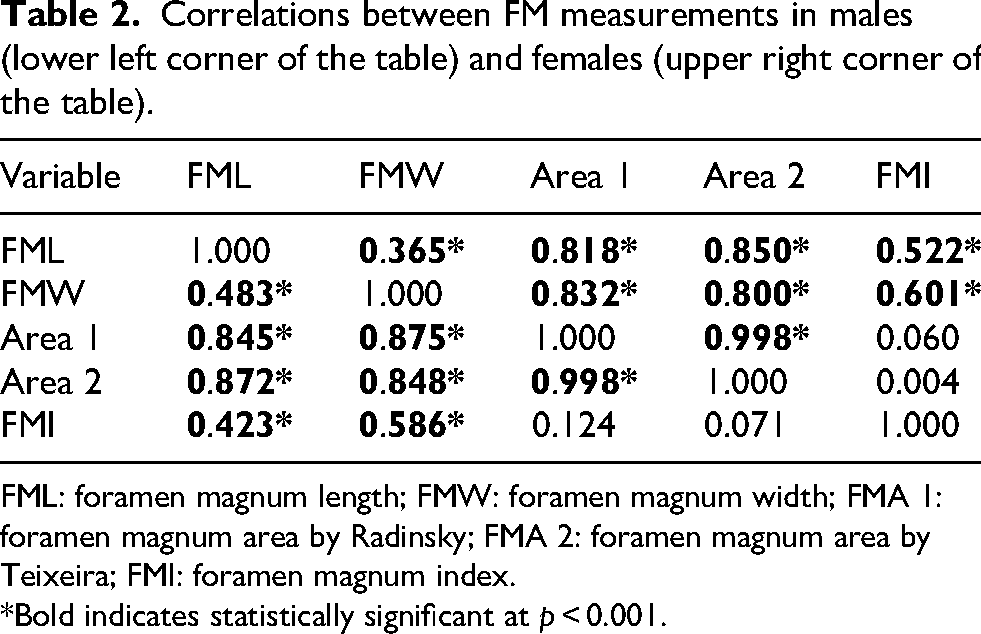
FML: foramen magnum length; FMW: foramen magnum width; FMA 1: foramen magnum area by Radinsky; FMA 2: foramen magnum area by Teixeira; FMI: foramen magnum index.
*Bold indicates statistically significant at p < 0.001.
DFA for univariate and multivariate analysis of FM measurements was presented in Table 3. The accuracy of the discriminant functions ranged from 58% to 68.5%. Furthermore, all the univariate discriminant functions displayed a higher accuracy in classifying males compared to females. In the univariate analysis, FML and Area 2 were the most reliable variables for sex estimation, with high accuracy (68.5%) and low sex bias rate (1.2%). The least reliable variable was FMW, with low accuracy (58%) and a high sex bias rate (3%). Notably, the multivariate discriminant function demonstrated a slightly better accuracy rate (70.5%) than the univariate analysis.
Univariate and multivariate discriminant function models for sex estimation using foramen magnum measurements.
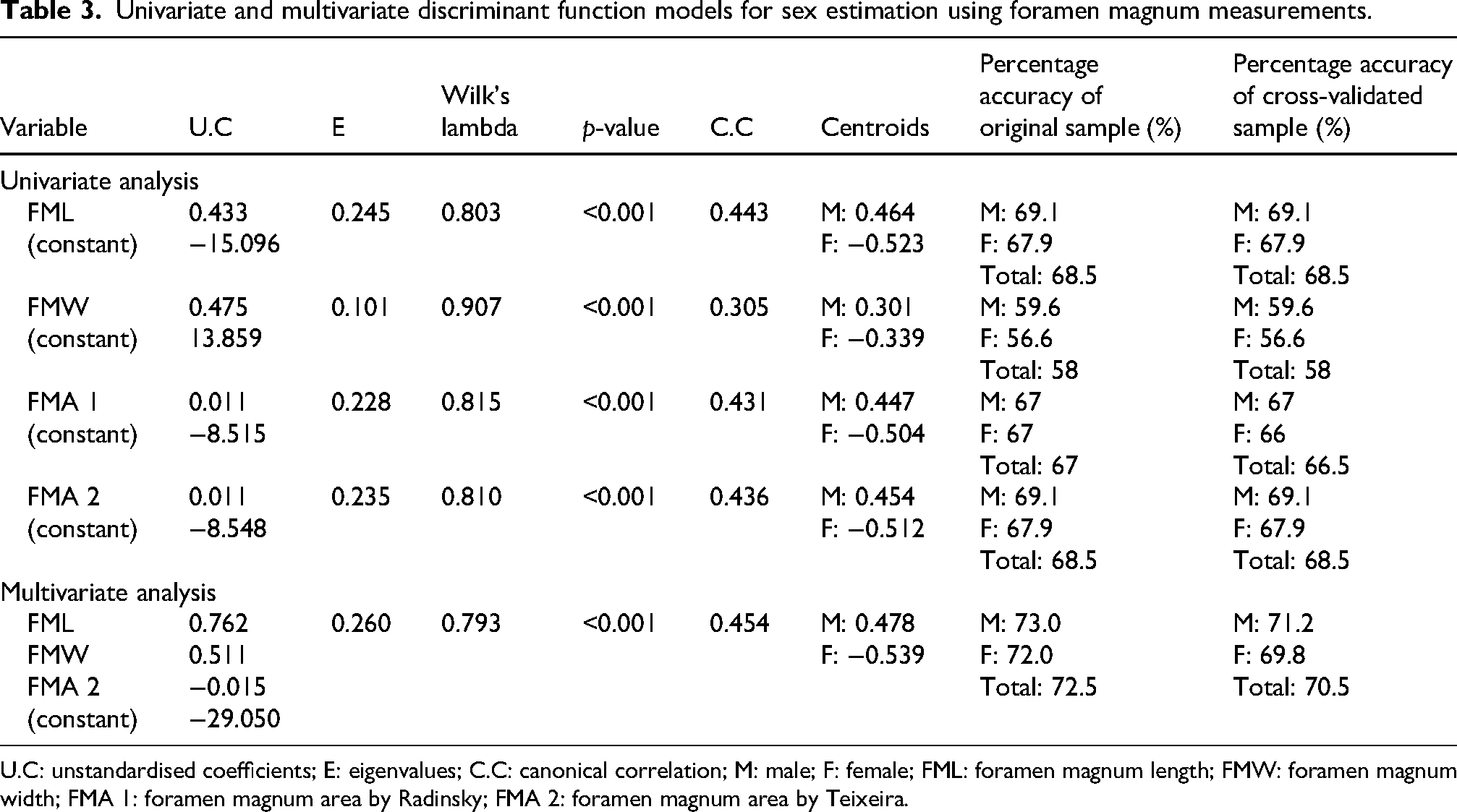
U.C: unstandardised coefficients; E: eigenvalues; C.C: canonical correlation; M: male; F: female; FML: foramen magnum length; FMW: foramen magnum width; FMA 1: foramen magnum area by Radinsky; FMA 2: foramen magnum area by Teixeira.
Table 4 shows the findings from the univariate and multivariate BLR analysis. In the univariate analysis, FML was the most reliable variable for sex estimation, with a higher accuracy (68.5%) and a lower sex bias rate (2.8%). In contrast, the least reliable single variable was FMW, with a lower accuracy (62%) and a higher sex bias rate (14.6%). Moreover, all the univariate discriminant functions were more accurate in classifying males than females. Similar to the univariate analysis, the multivariate BLR analysis recorded an accuracy rate of 68.5%. A comparison between the DFA and BLR methods revealed that the former yielded higher overall accuracy and the lowest sex bias in all cases (original and validation samples).
Univariate and multivariate binary logistic regression models for sex estimation using foramen magnum measurements.
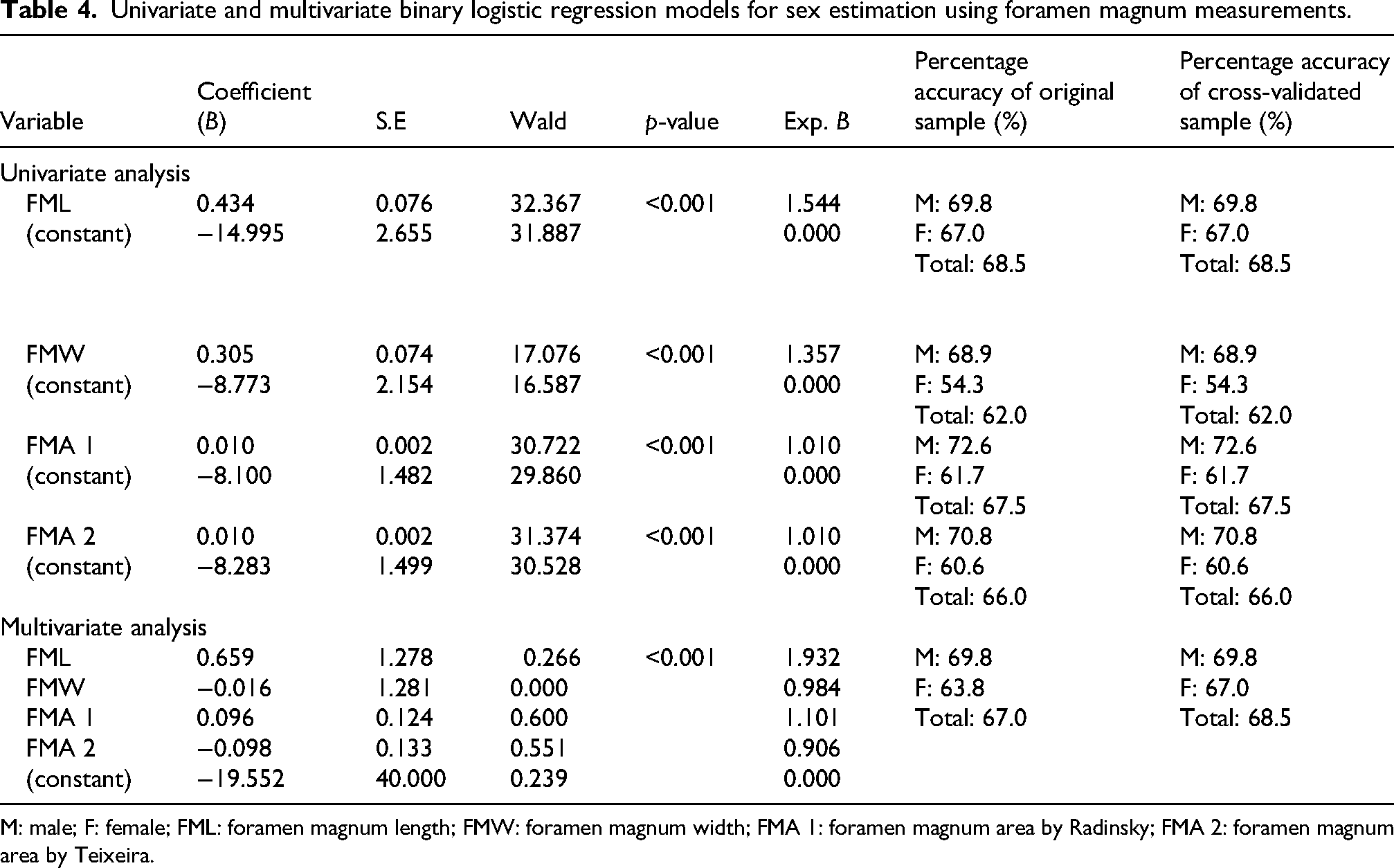
M: male; F: female; FML: foramen magnum length; FMW: foramen magnum width; FMA 1: foramen magnum area by Radinsky; FMA 2: foramen magnum area by Teixeira.
Discussion
The present study aims to estimate sex in the Malaysian juvenile population using measurements of the FM obtained from CT data. The age range of 8–16 years was chosen to focus on juveniles during an important stage of skull development. At this age, the FM is fully developed for accurate measurement, making it suitable for studying early signs of sex differences.23,24 This age range also minimises potential measurement errors associated with younger children, whose cranial structures may not be fully ossified or clearly delineated in imaging scans.
The current study observed that sexual dimorphism in the FM was evident among juveniles aged 8 years and older, manifested by the larger FM dimensions in males. Furthermore, statistically significant differences were observed in FML, FMW, and FMA between the sexes, indicating a dimorphism in FM. Similarly, Seifert et al. 33 and Meral et al. 34 reported significant sex-based differences in nearly all linear FM measurements. Other studies have also reported that the sagittal and transverse dimensions of FM were often significantly higher in males than in females.10,35–37 However, some reports have indicated minimal or no differences between sexes.38–40 These findings may be due to individual variation in cranial size, influenced by genetic and hormonal factors during development. 33
Population differences play a crucial role in defining sexual differences in the FM. The FML and FMW measurements of the Malaysian population are comparable to numerous other populations for both males and females.2–4,9,11,12,31,41–43 However, the Malaysian population also exhibited both higher6,10,34,35,44 and lower45,46 FML and FMW measurements compared to certain populations. Regarding the FMA, most populations exhibited higher measurements than the Malaysian population,2,11,31,34,35,47 except in certain studies.3,13,43,48 Therefore, acquiring data specific to the population is important for achieving a high accuracy rate in sex estimation.
Linear discriminant classification has been the preferred statistical analysis of skeletal metric traits in sex estimation using bones. 11 In this study, univariate DFA analysis identified FML, FMA 2, and FMA 1 as the most reliable individual variables for sex prediction, with accuracy rates of 68.5%, 68.5%, and 66.5%, respectively. The findings of the current study were consistent with a previous study conducted by Aljarrah et al., 11 which examined 472 CT scans of the Saudi Arabian population. This study found that FMA (65% and 66.4% using formulas by Radinsky and Teixeria, respectively) and FML (62.45%) were superior tools for skull sexing. 11 Likewise, other studies identified FML13,49 and FMA2,3,11 as the best individual variables for sex identification, with accuracy rates between 66.4% and 90.7%. In this study, FMW was found to be the least reliable sex predictor, with an overall accuracy of 58%. This finding contradicts earlier studies that reported FMW as one of the most reliable sex predictors, with an accuracy of 64.7%–90%.4,10,49
The accuracy rate of this present study (70.5%) is observed to be higher than those reported in previous studies involving adults.2,3,6,11–13,31,42,43 Tellioglu et al. 13 utilised CT images to measure the FM and reported an overall sex estimation accuracy of 66%. Meanwhile, Tambawala et al. 2 reported an overall accuracy of 66.4%. Conversely, Abdel-Karim et al. 4 and El-Barrany et al. 10 recorded an accuracy rate of 90% and 84.3%, respectively, in sex estimation using FM variables. Veroni et al. 9 reported a higher accuracy of 75.8% in determining sex from juvenile FM. The higher accuracy could be attributed to the inclusion of occipital condyles in the overall measurements. 9 Furthermore, the FM undergoes earlier maturation and fusion than other skeletal elements, potentially limiting their sexual dimorphism and significant response to secondary sexual changes. 36
The FM shape is influenced by developmental changes affecting four parts of the occipital bone morphology and the intra-occipital synchondroses. The prevalence of the FM shape in the Malaysian population is oval or oval-to-round. Specifically, males tend to have a narrow oval shape, whereas females commonly display a rounded shape. Previous research indicates that the oval shape was more commonly found in Polish, 41 Greek, 50 and Sudanese populations, 36 while the round shape was predominant among the Swiss population 35 and Turks. 37 In addition, no significant difference was observed in the FM shape between males and females in the Malaysian population, consistent with previous research.35–37,41 This indicates that the FM shape is not a reliable indicator of sex for Malaysian juveniles.
Classification methods such as DFA and BLR have become integral parts of diverse statistical analyses, enabling swift data processing. 33 The present study observed that DFA consistently obtained a slightly higher overall accuracy and lowest sex bias across all cases (original and validation samples). Similarly, Gapert et al. 12 reported that BLR achieved lower accuracy rates compared to DFA when developed on a sample of 158 crania from the British population. In a study conducted by Edwards et al., 35 the authors reported that BLR had a relatively lower ability to classify females, despite achieving a higher overall accuracy than DFA. This demonstrates the robustness of DFA, as it predicts both sexes equally effectively. 12
Virtual model measurements may present certain limitations when compared to direct measurements on dry skeletal remains. However, recent research has demonstrated that the associated error in virtual assessments of juvenile crania typically does not exceed 2 mm, indicating a high degree of reliability.51–54 Moreover, the average difference between measurements obtained from virtual models and those from dry bones has been reported to be approximately 1.5%, a variance considered minimal and negligible.55,56 These findings affirm that cranial measurements derived from CT scans are sufficiently accurate and can serve as a dependable alternative to traditional dry bone measurements in forensic and anthropological analyses.
In forensic casework, especially in cases involving juvenile remains, sex estimation is often limited due to the incomplete development of sexually dimorphic traits. The present study provides forensic anthropologists with an alternative approach by validating the use of FM dimensions as a reliable indicator of sex in Malaysian juveniles. The FM is one of the preserved cranial structures in fragmentary remains; hence, these findings are particularly valuable in mass disaster situations, criminal investigations, or archaeological contexts where only partial remains are available. 5 Moreover, the use of MSCT data allows for retrospective analysis and 3D reconstruction, offering practical advantages for long-term forensic investigations. 28 Finally, the present study not only supports current forensic applications but also lays a foundation for future methodological innovation in the field.
This study has a few limitations that should be acknowledged. First, the sample may not fully represent the entire Malaysian population, as the MSCT data were obtained from a single medical institution, which may limit the generalisability of the findings to other regions. Second, the socioeconomic background of the individuals was unknown, and it was assumed that all participants had equal access to healthcare. Despite these limitations, the study has several strengths. It utilises high-resolution MSCT, allowing for precise and reliable measurement of the FM. It also addresses a gap in the literature by focusing on the Malaysian juvenile population. The balanced sample of 100 males and 100 females adds to the strength of the analysis, enhancing the reliability of the results. Importantly, the findings offer potential applications for sex estimation in juvenile individuals within the Malaysian population.
The present study offers valuable findings that contribute to the foundation for future research in the development of sex identification methods. To enhance the generalisability and accuracy of such models, future studies should consider expanding the sample size to include individuals from various geographic regions across Malaysia, thereby enabling the identification of population-specific patterns. Additionally, incorporating adult populations will provide a more comprehensive understanding of sexual dimorphism in the FM across different age groups. Lastly, the integration of advanced computational approaches, such as machine learning and deep learning, presents significant potential in forensic anthropology. With access to large and diverse datasets, these technologies may offer more accurate, efficient, and objective methods for sex estimation.
Conclusion
This study demonstrated the potential of the skull base as an indicator for sex estimation in the Malaysian juvenile population. The FM sexual differences offer valuable and reliable information in cases where genetic profiling is impossible due to bone deterioration and partial skull remains. Achieving a higher precision in sex estimation largely depends on utilising representative population standards for individual classification.33,57 Our findings suggest that FM parameters can complement the existing sexing data and be combined with other methods to aid in estimating the sex of a skeleton.
Footnotes
Acknowledgements
The first author expresses gratitude to the Radiology Department at University Malaya Medical Centre (UMMC) for their support in acquiring MSCT scans.
Ethical approval
Ethical approval was obtained from the Medical Research Ethics Committee, University Malaya Medical Centre (MREC ID No: 202147-10039). In addition, all procedures conducted in this study involving human participants were in compliance with the guidelines and regulation standards of the national research committee and with the 1964 Helsinki declaration.
Consent to participate
The requirement for informed consent was waived by the Medical Research Ethics Committee, University Malaya Medical Centre because this is a retrospective study based on CT images obtained from the hospital archive system.
Consent for publication
Not applicable.
Author contributions
SNSMH, RAR, and NI contributed to the conception and design of the work; acquisition, analysis, and interpretation of data; drafting of the manuscript; and final approval of the version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research management fund (Project No.: RMF 0637-2021) from Universiti Malaya was used to fund this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Requests for accessing the datasets during the current study should be directly addressed to the corresponding author on reasonable request.