
Abstract
Head injuries, resulting from mechanical forces impacting the scalp, skull, and brain, are a major cause of morbidity and mortality, particularly in road traffic accidents (RTA). While skull fractures alone may not be fatal, they often lead to significant haemorrhage and brain damage. This study aims to analyse the patterns of head injuries in postmortem cases, focusing on the type, site, and extent of skull fractures, and correlating these with scalp, facial, and brain injuries, especially in RTA cases. A cross-sectional descriptive study was conducted over a span of 12 months at a tertiary healthcare teaching hospital in western India. A total of 350 postmortem cases of fatal head injuries were examined, following ethical approval. Inclusion criteria encompassed individuals who died due to head trauma, while decomposed bodies, natural deaths, and cases with unknown histories were excluded. Data on injury mechanisms, demographics, and postmortem findings, including skull fractures and associated injuries, were collected and analysed using descriptive statistics. Among the 350 cases, 52.57% of skull fractures were linear, 33.71% comminuted, and 21.14% depressed. The most frequent external injuries included scalp lacerations (90.84%) and abrasions (42.25%). RTAs accounted for 40.85% of skull fractures, with a notable incidence in the 21–40 age group (44.86%). Intracranial injuries were common, with subarachnoid haemorrhage (88.29%), cerebral contusion (65.43%), and subdural hematoma (66.29%) as the most prevalent. The presence of skull fractures correlated significantly with both scalp injuries and intracranial haemorrhages. This study reveals that skull fractures, particularly linear and comminuted, are prevalent in fatal head injuries, especially due to RTAs. Significant intracranial damage, such as subarachnoid haemorrhage and cerebral contusion, was frequently observed. The findings emphasise the need for targeted preventive measures and improved management strategies for head trauma, particularly in young adults.
Introduction
A head injury occurs when mechanical forces cause significant or minor structural alterations to the scalp, skull, and/or skull contents. 1 Being the most exposed portion of the body, the head is frequently involved in occurrences and plays a significant role in road traffic accident (RTA) morbidity and death. 2 The scalp has a robust blood supply; therefore, injuries can range from minor abrasions to extensive lacerations, frequently resulting in substantial bleeding.3–5 Linear, compression, or comminuted fractures are the possible forms of skull fractures that can happen at the base or vault of the skull. The classification of these fractures as open or closed depends on the skin’s integrity.3, 5 Although single skull fractures seldom result in death or severe morbidity from head injuries, these injuries typically involve haemorrhage and brain tissue damage.3, 4 RTA, fall from height or on level ground, occupational injuries, and assault are the usual causes of trauma with geographical variation. The World Health Organization (WHO) predicts that by 2030, RTA will rank as the fifth most common cause of death globally.6, 7 Since the mean age of trauma victims typically falls within the highly productive middle age group, head injuries are especially alarming.8, 9
In light of this, the purpose of this study was to examine head injury patterns in postmortem cases, with a particular emphasis on the type, site, size, and extension of skull fractures. The study sought to correlate the occurrence and characteristics of skull fractures with associated injuries to the scalp, face, and brain. Additionally, it aimed to explore the circumstances leading to these injuries, particularly in RTA cases, and analyse how these factors relate to the patterns of skull fractures observed.
Methodology
This cross-sectional descriptive study was conducted over a period of 12 months in the Forensic Medicine department at a tertiary care teaching hospital in western India. The consecutive sampling method was deployed for this study, where special emphasis was given to individuals who died from fatal head injuries and were brought for medico-legal autopsies, with a sample size of 350 cases, based on an estimated monthly load of 30–35 cases. Inclusion criteria involved deceased individuals with fatal head injuries, while cases of decomposed bodies, unknown histories, extensive burns, or deaths from natural diseases were excluded. Data collection involved gathering personal details from police inquest papers, hospital records, and interviews with relatives. Information on the head injury, mechanisms like RTA, fall from height, fall of heavy object, assault, railway accident, and the victim’s profile in RTA were documented. A detailed postmortem examination was conducted, with a focus on head injuries, including skull fractures and sub-scalp injuries. A standardised proforma was used to collect data on injury characteristics, demographics, and contextual information. Descriptive statistics, such as frequencies, percentages, and distributions, were employed for data analysis, and the findings were compared with existing literature to draw relevant conclusions.
Results
Out of the forensic autopsies conducted during the study period, 350 cases of head injury were analysed. Following noteworthy and pertinent findings from the current study are shown in a table and figure format.
Discussion
As per our observations depicted in Figure 1, males made up 295 cases (84.29%) of the 350 head injury cases because they were more likely to be involved in outdoor activities like driving and working outside, making them more likely to be involved in accidents. In contrast, females made up 52 cases (14.86%), and they died primarily from RTA or unintentional falls at home. The study by Pathak Akhilesh et al. showed a similar outcome, with a 5:1 male-to-female head injury case ratio. 10 According to the study by Sachin Chourasia and Abhijit Rudra, of the 50 cases of traumatic head injury caused by blunt force trauma, 40 (80%) were male, while only 10 (20%) were female. The male victim to female victim ratio in this study was 4:1. 11 Out of 350 cases in the current study, the age group of 21–30 years old had the highest incidence of head injuries, as shown in Figure 2. comprising of 84 cases (24.00%) followed by age group of 31–40 years (21.71%) comprising of 76 cases. The obvious explanation is that people between the ages of 21 and 40 make up most of the workforce and spend most of their time outside due to a variety of work-related, educational, and athletic activities that require frequent travel. As a result, they are more likely to sustain injuries from falls, assaults, and other traffic incidents. Since kids and elderly individuals are typically indoors, which comprises the dependent population of society, the age range of 1–10 and over 80 years had the lowest number of instances. Similar findings were observed in the study by Kamble NP, Chavan GS, and Deokar RB, which found that the frequently affected age range was 21–30 years old (29%), then 31–40 years old (19%). 12 This study contrasted with that of Raja Rupani, Anoop Verma, and Shiuli Rathore (2013), who found that the age group most at risk was 41–50 years old, followed by 11–20 and 21–30 years old. 13
Sex-wise Distribution of Cases.
Age-wise Distribution of Cases.
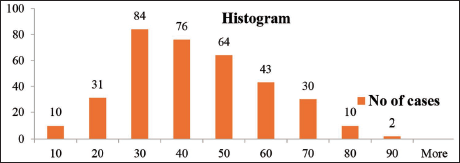
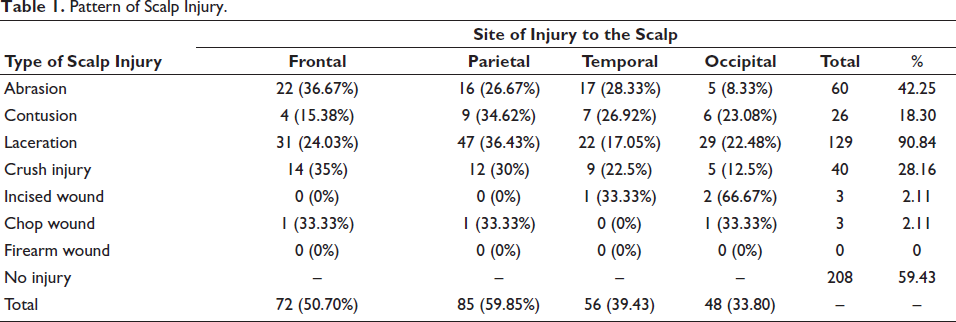
Table 1 shows the pattern of scalp injury according to the type of injury and site of scalp. Out of 350 cases, 208 cases (59.43%) did not show any kind of external injury to scalp, whereas remaining 142 cases (40.57%) showed presence of external injury to scalp. In 85 cases (59.85%), the parietal area was where these scalp injuries were most frequently observed, whereas least common site was occipital region in 48 cases (33.80%). Laceration was observed most frequently among all external injury over scalp which was seen in 129 cases (90.84%) with most common site being parietal region in 47 cases (36.43%) and least common site was temporal region in 22 cases (17.05%) followed by abrasion in 60 cases (42.25%), most common site of abrasion was frontal region in 22 cases (36.67%). The least common type of scalp injury was sharp force injuries, that was incised wounds and chop wounds, which accounted for three cases (2.11%) out of 142 cases showing presence of external injury to scalp. There was no case of firearm injury in the study. This study supports the result of a study carried out by Shivendra Jha et al., which showed that the most common type of scalp injury was laceration, which accounts for 46 cases (59.7%) of head injury due to RTA out of a total of 77 cases, followed by contusion, 21 cases (27.3%). 14 Similar trend was seen in a study by S.B. Bhatt, J.A. Tanna, who studied distribution of superficial injuries in vehicular accidents, where laceration was the most common injury over region of head and face in 30 cases (50%), followed by abrasion in 27 cases (45%). 15
Pattern of Scalp Injury.
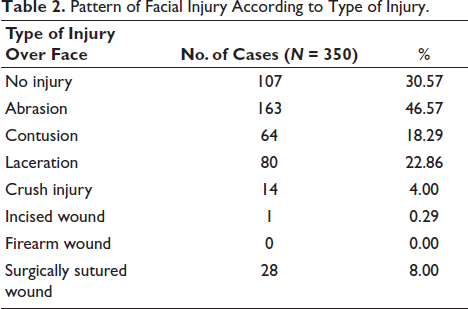
As shown in Table 2, out of 350 cases, only 107 cases (30.57%) did not show presence of any kind of facial injury, whereas remaining 253 cases (69.43%) showed presence of external injury over face. Among these, abrasion was commonest injury type encountered, which accounted for 163 in number (46.57%), then laceration, which accounted for 80 cases (22.86%). There was only one case of an incised wound, and no case of a firearm wound over the face. This study contrasts with the research conducted by Amit Kumar et al., according to which most common type of soft tissue injury over face was laceration, amounting to 79 cases (43.89%) out of 180 fatal accidents sustaining facial injury. 16 As per Table 3, only 22 cases (6.29%) did not show presence of any kind of under scalp injury, whereas remaining 328 cases (93.71%) showed presence of under scalp injury. Among which maximum number of cases were of sub-scalp contusion, which comprises 236 cases (67.43%), whereas least number of cases were of scalp laceration, that is, 53 cases (15.14%). Contusion of temporalis muscle was seen in 92 cases out of 350 (26.29%). According to a study by Sunil Nail, Dr Rupesh Naik, laceration was linked to skull fractures in 60 cases (61.86%) and scalp contusions in 104 cases (1.04%). 17
Pattern of Facial Injury According to Type of Injury.
Pattern of Under-scalp Injury.
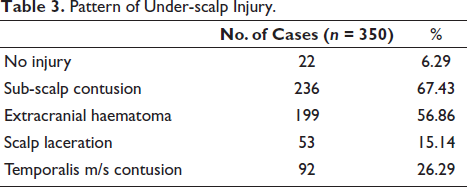
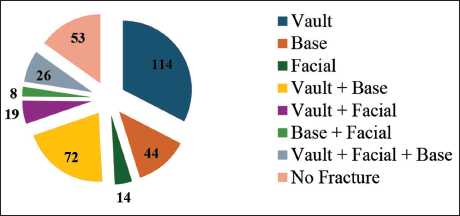
Figure 3 shows that out of 350 cases, 53 cases (15.14%) did not show presence of any skull fracture. The maximum number of cases of head injury showed presence of vault fracture in 114 cases (32.57%), followed by combined vault + base fracture in 72 cases (20.57%). The minimum number of cases was of facial fracture in 14 cases (4.0%), followed by combined fracture of facial + base in eight cases (2.29%). A similar trend was seen in a study conducted by Sachin Chaurasia et al., where out of 50 incidents in total, in 18 (46.15%) victims, the combination of vault and base fracture of skull was reported. In 19 cases (48.72%), skull vault alone was fractured, and in two cases (5.13%), the skull base was fractured. 11 This study contrasts with another by Raja Rupani et al. that found that, of 40 cases with skull fractures, 22 cases (55%) had a vault fracture, while 35% of cases involved both a base and a vault. 13
Pattern of Skull Fracture.
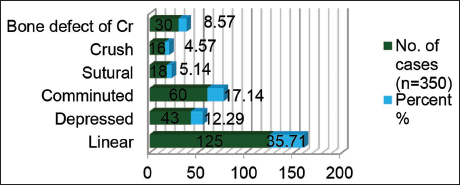
In our study, as depicted in Figure 4, among skull vault fractures, fissured/linear fracture was most common with 125 cases (35.71%), then comminuted and depressed fracture in 60 cases (17.14%) and 43 cases (12.29%) respectively. Crush fracture was least common in 16 cases (4.57%). A bone defect of craniotomy was seen in 30 cases (8.57%). This supports the findings of a research by Sunil Naik and Rupeshkumar Naik, in which the majority of 51 patients (52.6%) had linear or fissure fractures, 20 cases (20.6%) had comminuted fractures, 10 cases (10.3%) had both comminuted and depressed fractures, and others had various fractures. 17 This is also consistent with research by Dinesh Kumar et al. that found that the most prevalent kind of skull fracture was linear, occurring in 132 instances (16.34%), followed by comminuted fracture vertex in 128 cases (15.84%) and depressed fracture vertex in 122 cases (15.10%). Basal fractures were the least frequent type of fracture, occurring in 121 cases (14.98%). 18 In contrast, research by Ashok Kumar Rajaput et al. found that 46 cases (48.93%) of skull fractures were comminuted, 38 cases (40.42%) had linear fractures, 8 cases (8.5%) had depressed fractures, and 1 (1.06%) case had sutural and gutter fracture. 19
Pattern of Fracture of the Vault According to the Type of Vault Fracture.
As mentioned in Table 4, we reported that, most common site of linear fracture was temporal bone in 60 victims (32.61%), followed by parietal bone in 51 cases (27.72%). Least common site for linear fracture was occipital bone in 31 cases (16.85%). Most common site for depressed fracture was frontal bone in 22 cases (29.73%), followed by parietal bone in 20 cases (27.03%). A comminuted fracture was noted maximum over frontal bone in 42 cases (35.59%). Crush fracture was noted maximum over temporal parietal region in 16 cases (30.77%). This can be explained by the fact that the lateral part of the frontal and occipital zones, as well as the temporo-parietal regions, are the most susceptible thin areas of the skull. The thin structure is primarily responsible for temporal bone involvement. The frequent involvement of parietal bone in crush and depressed fractures is mainly due to prominences and elevation of the bones of skull. According to a study by Yavuz M. Sunay et al., there were more depressed fractures in the frontal and parietal regions and linear fractures in the temporal and occipital regions (p < .001). 20 In research by Arvind Kumar et al., skull fractures were discovered in 1183 (69.63%) patients of head injuries, showing a similar pattern. The temporal bone 559 (47.25%) was the most often affected bone, followed by the parietal (45.47%), occipital (41.01%), and frontal (33.64%) bones. 21 A study by Shri Bhagwan et al. noticed a contrast result, with bony involvement being maximum at frontal bone (44.3%) followed by temporal bone (30.6%). 2
Pattern of Fracture of the Vault According to the Site of Vault Fracture.

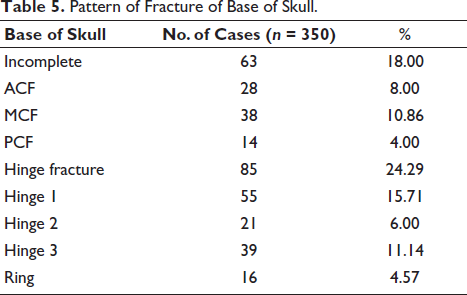
As shown in Table 5, among fractures of base of skull, maximum number of cases were of hinge fracture in 85 cases (24.29%), among which hinge fracture type 1, which involves middle cranial fossa, was seen in majority of cases, 21 cases (15.71%). The least common site of basal fracture was seen in posterior cranial fossa and ring fracture, which is also seen in posterior cranial fossa in 14 cases (4%) and 16 cases (4.57%), respectively. This is comparable to research by Saurabh Chattopadhyay and Chandrabhal Tripathi, in which only fatal cases (58.9%, n43) had a fracture of skull base. Posterior cranial fossa fracture was least frequent (4.1%); however, most vulnerable area to mechanical harm was middle cranial fossa. (38.35% n-28). 22
Pattern of Fracture of Base of Skull.
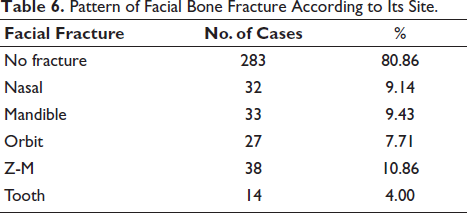
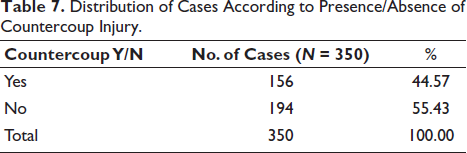
Out of 350 cases, as shown in Table 6, no facial bone fracture was observed in 283 cases (80.86%). Among facial bone fractures, most common site was zygomatico-maxillary (Z-M) bone in 38 cases (10.86%), followed by mandible in 33 cases (9.43%). Amitkumar et al.’s study revealed that the mandible bone was the most frequently fractured facial bone, accounting for 5 (39.45%) of all cases. Four cases of nasal bone fracture (29.36%) and two cases of tooth fracture (17.43%) were documented. Zygomatico-maxillary complex fractures, amounting to only one, were the least frequent kind of fracture. Table 7 shows that 156 cases (44.57%) out of total of 350 cases of head injury showed presence of counter coup injury along with coup injury, which is suggestive of moving head in cases of RTA and Falls. According to a study conducted by Udaya Shankar et al. of a total of 181 cases, 28 cases had coup and contrecoup injuries. 23 According to research by Shivendra Jha et al., contrecoup injuries were most common in the frontal areas (62.5%), then in occipital (18.75%), right side lateral (2% or 22.5%), and left side lateral region (1% or 6.25%). Because of abundance of bony projections that originate from the base of the anterior cranial fossa, the frontal areas may have a higher prevalence of contrecoup lesions. It is reasonable to assume that the right lateral has a higher incidence of contrecoup lesions because the right side is more likely to be struck there. 14
Pattern of Facial Bone Fracture According to Its Site.
Distribution of Cases According to Presence/Absence of Countercoup Injury.
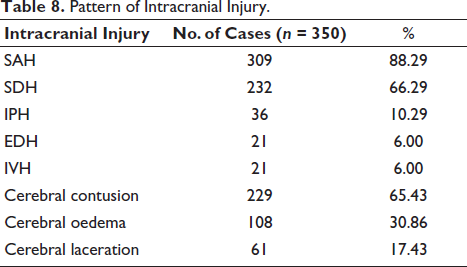
In the present study, as shown in Table 8, the maximum number of cases of subarachnoid haemorrhage (SAH) was present in 309 cases (88.29%), followed by subdural haemorrhage (SDH) in 232 cases (66.29%). Both Extradural haemorrhage (EDH) and Intraventricular haemorrhage (IVH) were seen in only 21 cases (6%). Brain contusion was the most common injury encountered in 229 cases (65.43%), then brain oedema in 108 cases (30.86%) and laceration of the brain in 61 cases (17.43%). In their study, Shreemantakumar Das and Asis Kumar Ray found that 182 cases—or 87.92% of the total of 207 head injuries—had intracerebral haemorrhage (ICH), either alone or in combination. The mixed kind of haemorrhage variety accounted for 74 cases, or 35.74%, of the 207 head injuries in the dataset. Subdural haemorrhage, however, was the largest when considered separately, accounting for 58 (28.01%), then extradural 20 (9.66%) and subarachnoid 17 (18.21%). Intracerebral haemorrhage 13 (6.28%) was the least common, and 25 cases (12.07%) had no visible haemorrhages. 24 Ganveer GB et al. observed a similar pattern in brain damage, indicating that cerebral contusion was the commonest, occurring in 41 cases (56.1%), then cerebral oedema in 24 instances (32.8%). 25
Pattern of Intracranial Injury.
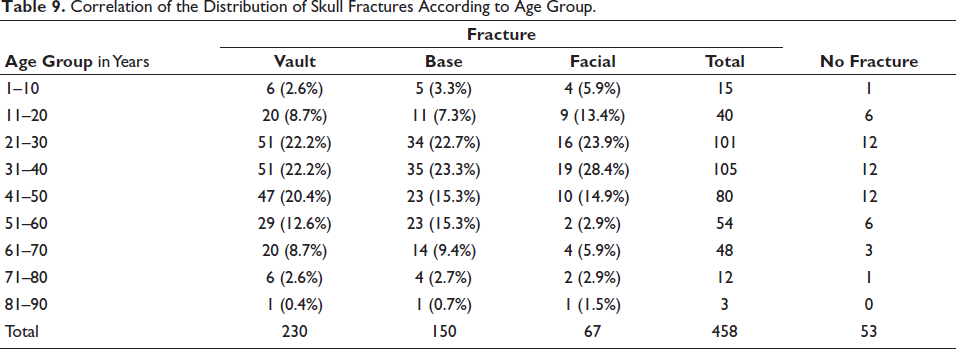
In the current study, as depicted in Tables 9 and 10 age group mostly affected by skull fracture was 31–40 years with 105 cases, then 21–30 years with 101 cases, while there was only one case of skull fracture in 81–90 years. All three varieties of skull fracture, that is, fracture of vault, basilar fracture and facial bone fracture, showed dominance in the age group of 31–40 years. A study conducted by Anand Patil et al. observed that the most frequently affected age group of victims with skull fracture was 21–30 years, that is, 52 cases (30%), then 31–40 years, that is, 51 cases (29%) and a single case in 61–70 years. 26 We observed that both fracture of vault and basilar fracture showed male preponderance, among which fracture of vault was present in 199 cases (51.6%), followed by basilar fracture in 132 cases (34.3%). Facial fracture showed female preponderance in 13 cases (21.6%). Percentage of females with vault fracture was equivalent to percentage of males with vault fracture. As shown in Table 11, fracture of vault was the dominant type of skull fracture in RTA (143 cases, 40.85%), fall of heavy object (16 cases, 4.57%), assault (12 cases, 3.42%), while basilar fractures were dominant in cases of fall from height in 53 cases (15.14%). Railway accidents show dominance of facial fractures in 15 cases (6.48%). A similar pattern was observed in research by Pathak Akhilesh et al., that basilar fractures are somewhat more common in cases of falls from height, linear fractures are more likely in situations of RTAS. Compared to falls from heights and assaults, RTAs are more likely to result in linear fractures that extend to the base of the skull. This is because head injuries caused by forceful contact with a broad resisting surface, such as the ground, are more likely to occur in these situations, especially when the victim is moving. 10 A study conducted by S.R. Saritha, C.S. Sreedevi observed that among all cases of fall from height, the skull was fractured in 36 cases (35.3%). Skull fractures with brain injury and intracranial haemorrhage were the most common combination of head injuries (25.5%). 27 Abhishekh Sangal et al. conducted a study to analyse the pattern of homicidal deaths, among which in over half (49.33%) of the homicide victims, the most vulnerable parts were the chest and abdomen combined, followed by the head in 18.06%. 28
Correlation of the Distribution of Skull Fractures According to Age Group.
Correlation of the Distribution of Skull Fracture According to Gender.

Correlation of Distribution of Skull Fracture According to Mechanism of Head Injury.
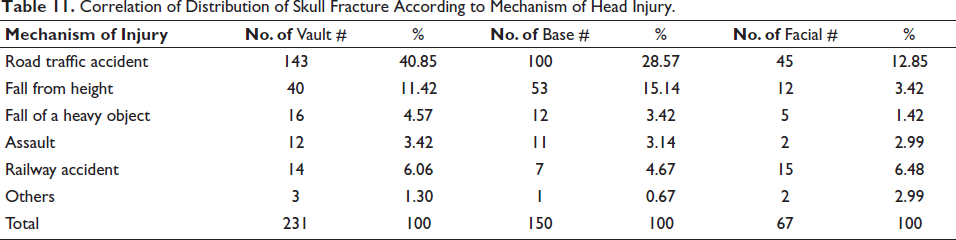
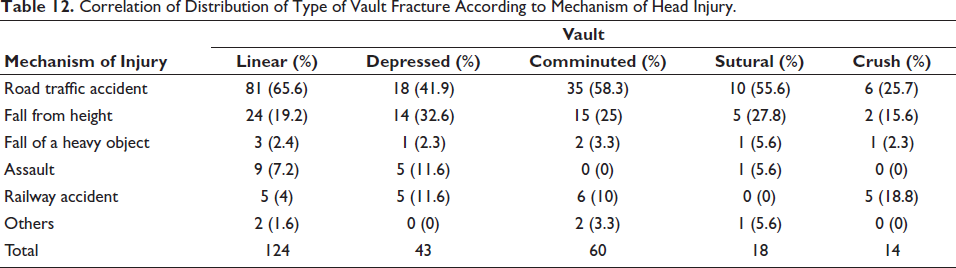
Table 12 shows that RTA shows dominance of linear fracture in 81 victims (65.6%), then comminuted fracture in 35 victims (58.3%). Victims of falls from height show dominance of depressed fracture in 14 cases (32.6%), followed by sutural fracture in five cases (27.8%). The fall of a heavy object on the head shows maximum number of victims with sutural fracture in 8 (5.6%) cases, assault shows dominance of depressed fracture in five cases (11.6%), and railway accidents show exclusive presence of crush fracture in five cases (18.8%). In their study, Yavuz MS et al. demonstrated that the striking power, strike area, and physical characteristics of the skull at the point of impact are associated with the occurrence, degree of deformation, and extent of fracture. Compared to a linear fracture, the highest frequency of depressed fractures in homicide cases suggests that a significant amount of force was used. The force that causes harm to the underlying brain increases with the amount of force applied. 20 Table 13 shows a similar trend was observed in a study by Dr Sunil Kumar Soni et al., where in traffic accidents, fracture of skull was found in 57% victims and with commonest type of skull fracture being linear fracture alone (n = 64, 32%), then depressed (n = 19, 9.5%) and least common sutural fracture alone. 29 The study is in contrast to study by Dr Sunil Naik, where all cases of homicidal deaths with skull fracture show a majority of linear fracture in 51 cases (52.6%), then comminuted 20 (20.6%), while 10 (10.3%) victims sustained both comminuted and depressed fractures, followed by others. 17
Correlation of Distribution of Type of Vault Fracture According to Mechanism of Head Injury.
In this study, as mentioned in Table 13, majority of victims with fracture of vault had corresponding laceration type of external injury to scalp and face in 58 cases, followed by abrasion in 32 cases. Contusion was the most common external injury seen in victims with basilar fracture in 21 cases, whereas abrasion and laceration were dominant types of external injury in cases of facial fracture in 20 and 18 cases, respectively. The majority of victims without skull fracture showed dominance of laceration type of injury. Most scalp abrasions had associated fissured/linear fractures (59%) of the cranial vault and base of skull bones, then comminuted fractures (30.8%), as per a study by Udaya Shankar et al. The most frequent calvarial fractures associated with scalp lacerations were comminuted fractures (52.8%), then fissured/linear fractures (24.2%). However, there were no skull bone fractures because in 12 cases (15.7%), lacerations were only deep in the scalp tissue. 23
Correlation of Distribution of Type of Skull Fracture According to External Injury to Scalp and Face.
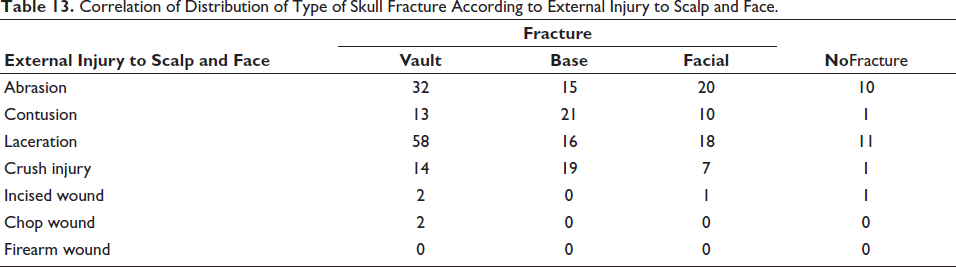
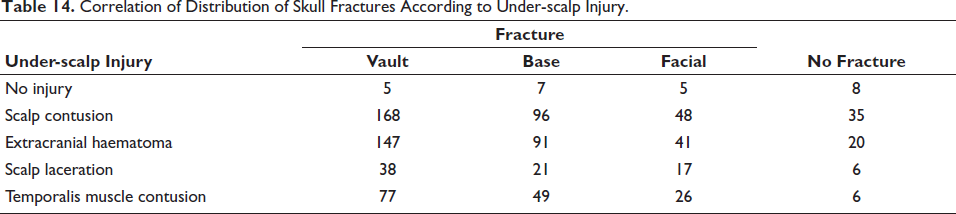
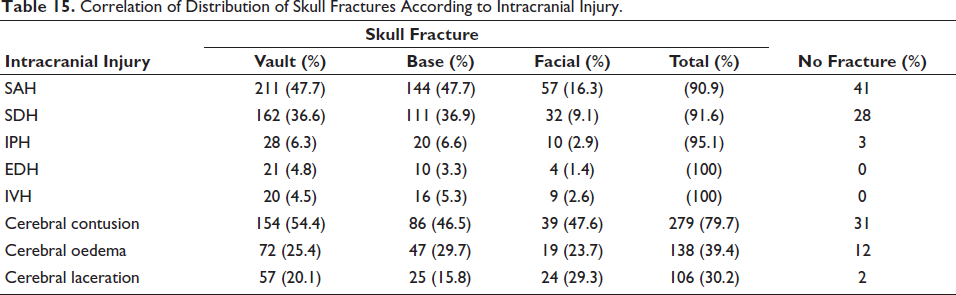
Table 14 shows the fracture of the vault, which shows maximum incidence of corresponding scalp contusion in 168 cases, followed by extracranial hematoma in 147 cases; basilar fracture shows incidence of scalp contusion in 96 cases, whereas facial fracture shows corresponding scalp contusion in 48 cases. The analysis of Table 15, emphasising the type of skull fracture pertaining to type and presence of intracranial haemorrhage, reveals that skull fracture shows 100% presence in all cases of head injury with extradural haemorrhage and intraventricular haemorrhage, among which vault fracture shows dominance in 21 cases (6%) and 20 cases (5.7%) respectively. Subarachnoid haemorrhage was the least common among all intracranial haemorrhages with corresponding fracture in 90.9% cases. Most of the cases with fracture of the vault lead to rupture of the epidural space’s blood vessels, thus the incidence of extradural haemorrhage is maximum among cases with fracture of the vault, in 21 cases (4.8%). However, the force of impact was more in basilar fractures, which were transmitted to the deeper structures of the brain, leading to maximum incidence of intraparenchymal haemorrhage and intraventricular haemorrhage in 20 cases (6.6%) and 16 cases (5.3%), respectively. In the present study, the most common injury to brain encountered in fracture of vault is brain contusion in 154 cases (54.4%). Basilar fracture shows dominance of oedema of brain in 47 cases (29.7%), whereas facial fracture shows the presence of laceration of brain exclusively in 24 cases (29.3%). The fact that brain contusions and lacerations are more common in areas where the brain encounters projectile buttresses and ridges on the inner surface of the skull, such as the orbital surfaces of the frontal lobes and the inferior surface of the temporal poles, can help to explain the higher incidence of laceration-type brain injury in facial fractures and contusion in vault fractures.
Correlation of Distribution of Skull Fractures According to Under-scalp Injury.
Correlation of Distribution of Skull Fractures According to Intracranial Injury.
Limitations
The study was limited to a single tertiary care centre in western India, which may affect the generalizability of its findings to broader populations or other regions. It included only fatal head injury cases brought for medico-legal autopsy, thus excluding non-fatal or treated cases that might show different patterns of skull fractures. Cases with decomposed bodies, unknown histories, or extensive burns were excluded, potentially omitting relevant data that could influence injury pattern analysis.
Conclusion
The study demonstrates a clear gender and age distribution in head injury cases, with males being predominantly affected (84.29%), especially in the active working age group of 21–40 years, which correlates with the increased outdoor and vehicular activities. The most common types of injuries observed were lacerations and contusions, primarily in the parietal and frontal regions of the scalp and face. Skull fractures were frequent, with the vault and basilar fractures being the most prevalent. RTAs were identified as the primary cause of injuries, followed by falls and assaults, with fracture patterns varying depending on the type of incident. Intracranial haemorrhages, such as subarachnoid haemorrhage and subdural haemorrhage, were the most common complications observed.
The findings of this study are consistent with previous research, but some variations were noted in the injury types and locations. The overall results underline the significance of trauma severity and impact direction on the type of injury sustained, as well as the role of age and gender in the vulnerability to head injuries.
Recommendations
Based on the findings, it is recommended to prioritise road safety measures, especially for males and individuals aged 21–40 years, who are more prone to head injuries due to accidents. Public awareness campaigns on safe driving, helmet use, and fall prevention should be implemented, with a focus on high-risk occupations and age groups. Further, better emergency medical protocols and early diagnosis should be promoted to manage scalp and brain injuries effectively. Additionally, efforts should be directed towards the prevention of falls in the elderly and children, as well as the management of fractures, particularly vault and basilar fractures, through improved trauma care and services for rehabilitation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Institutional Ethics Committee’s ethical permission was acquired by letter number IECBHR/131-2020 dated 4 December 2020.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
This study was conducted on mandated forensic autopsies, as directed by the Police/Magistrate inquest. While consent is not required for the medico-legal autopsy itself, Ethical approval for the research was granted by the IEC of the Institute. All identifying information has been anonymized to protect the confidentiality and privacy of the deceased.