
Abstract
Trauma is a major cause of disability and death in India, and thorax injuries constitute an important aspect of trauma. Our aim was to study the nature and pattern of thoracic injuries among the cases autopsied in the study period. Aforementioned data was compiled, analyzed and results drawn after 306 cases involving chest injuries were examined.
The deaths due to chest trauma constituted 24% of the total autopsied cases, and 84% were males. The majority of the deceased belonged to the age group of 21–40 years (N = 124 and 40.5%). Rib fractures were the most common skeletal injuries, followed by clavicular and sternal fractures. Head and neck (56%) were the commonest sites of other injury associated with chest injuries, followed by limb fractures (23%). Common internal organs injured were liver (15%), lung (8.9%), and heart (2.7%). Among accidents, road traffic accidents (RTA) was the most common cause of chest injuries, and pedestrians (24.4%) were the main affected than occupants of vehicles. In the majority of cases, the cause of death was hemorrhagic shock (51.5%), followed by trauma to head (27%).
This study concluded that road accidents were the most common causes of chest trauma, followed by railway accidents. Males in the productive age group (21–50 years) were the most affected in trauma. Lacerations and contusions were the most common injuries in intra-thoracic organs. Efforts can be made to decrease fatalities through the strict implementation of safety measures at workplaces and creating public awareness about road safety and precautions.
Introduction
Thorax is the upper part of the trunk, consisting of a musculoskeletal cage, a wall and an internal cavity. The chest wall surrounds the thoracic cavity with 12 pairs of ribs and articulates with 12 thoracic vertebrae posteriorly and with the sternum anteriorly. The diaphragm is the key muscle in thoracic cage movements of breathing. 1 The chest or thorax is regarded as one of the most vulnerable regions of the body to injury. Due to its accessible anatomical position and circumscribed dimension, the thorax is a major site of impact in any form of trauma. 2 Typically, chest injuries are caused by blunt mechanisms such as motor vehicle accidents or penetrating mechanisms such as stabbings. 3
Trauma to the thorax is responsible for over 70% of all deaths following road traffic accident (RTA), and blunt trauma to the chest alone is fatal in 10% of cases, rising to 30% if other injuries are present. In most cases, the cause of death is hemorrhage. 4 Thoracic cage injuries like abrasions, contusions and rib fractures are found in all fatal falls. Multiple fractures of the whole cage, including the sternum and thoracic spine, are found when the height of the fall is more than 25 meters along with ruptures and contusions of the lungs and heart. 5 In spite of high mortality rates, about 80%–90% of patients with life-threatening thoracic injuries can be managed by simple interventions like tube thoracotomy. 6 In this study, thoracic injuries were evaluated according to age, sex, pattern, and manner of causation of injuries, and period of survival after sustaining injury. All this information can be used in policymaking to reduce mortality and develop preventive strategies.
Materials and Methods
This study was aimed at knowing the epidemiologic pattern and characteristics of chest injuries in the autopsied trauma cases in our region and also to find out the mechanism of injury causation. This was a prospective study based on 306 trauma-related deaths with thoracic and other associated injuries brought to the mortuary of a referral center in Tirupati among the total of 1251 autopsies conducted during the study period (January 2014 to June 2015).
All the trauma victims with thoracic injuries were considered for the study and examined. The cases screened for thoracic injuries were mostly resulting from RTAs, railway accidents, assault, firearm injuries, falls from height, and falls due to electric shock. Relevant information regarding the circumstances of trauma and the course of death was obtained from friends, relatives, and police sources. The details were noted in a proforma prepared for the study, and data were analyzed. Cases with thermal injuries over the chest and those with head injuries from RTAs and assaults without chest injuries were excluded.
No conflict of interest or financial help has been taken from any source.
Observations
The pattern of injuries is as shown in the form of tables.
Table 1 shows the age and gender-wise distribution of fatal thoracic injuries. Of the 306 cases studied, 257 were male (84%). The majority of the victims belonged to the age group of 21–40 years (N = 140, 43.5%).
Age and Gender Wise Distribution of Cases.
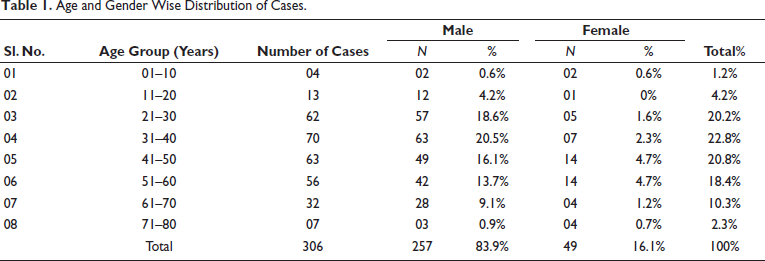
Table 2 shows the manner of causation of thoracic injuries with the number of casualties. RTAs were the most common cause of chest trauma (65%), followed by railway accidents (17%) and assault cases, including stab and firearm injuries (10%).
Manner of Causation of Thoracic Injuries.
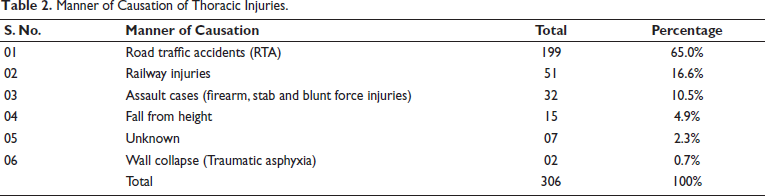
Table 3 shows the distribution of fatal thoracic injuries in terms of the period of survival of victims after the trauma. More than half of the victims were found spot dead (52%).
Period of Survival After Trauma.
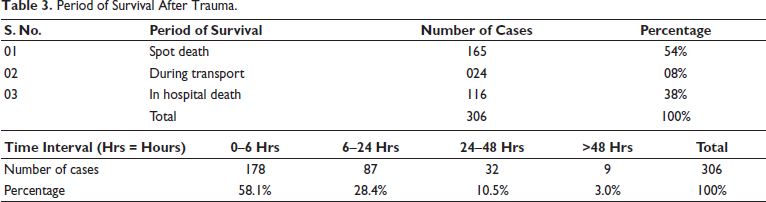
Table 4 shows the type and distribution of thoracic injuries. Rib fracture (37.3%) was the most common type of skeletal injury, followed by clavicular (8.2%) and sternal fractures (7.7%). Internal injuries were lacerations of the lung (13%), followed by those of the heart (4.2%).
Nature and Distribution of Fatal Thoracic Injuries.
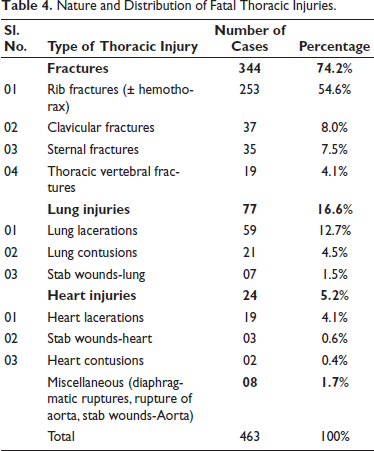
Table 5 shows the association of other bodily injuries contributing to death.
Association of Other Bodily Injuries Contributing to Death.
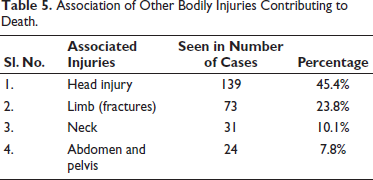
Table 6 shows the types of victims with thoracic injuries in road accidents. Pedestrians (24.4%) were the most affected type of victim.
Type and Distribution of Accident Victims with Thoracic Injury.
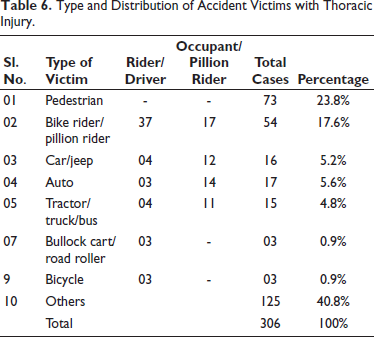
Table 7 shows the various causes of death among fatal cases involving thoracic injuries. Hemorrhagic shock (51.5%) was the major cause of death among the victims, followed by head trauma (27.7%).
Causes of Death in Cases Involving Thoracic Injuries.
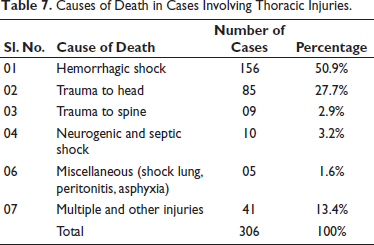
Table 8 shows the pattern of diurnal variations. The majority of the incidents occurred between 6 pm and 12 am (29%) and the least between 6 am and 12 pm (17%).
The Pattern of Diurnal Variations.
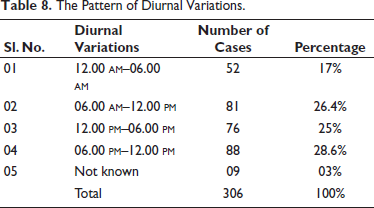
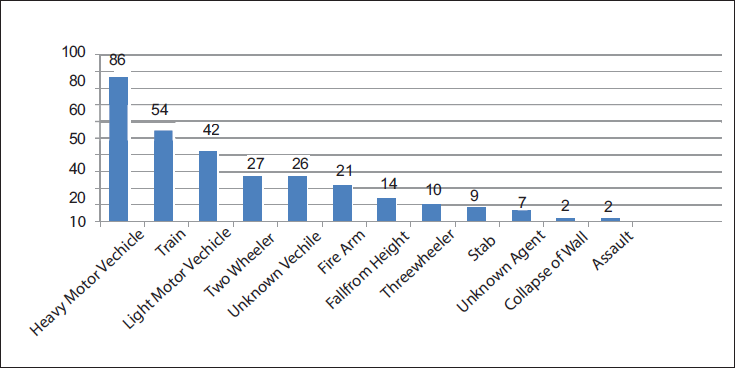
Figure 1 depicts the agent causing chest injury.
The Agent Causing Chest Injury.
Discussion
Injuries to the chest are mostly accidental, occasionally homicidal, and very rarely suicidal due to the accessible nature of the chest. In chest trauma, the mortality is very high unless promptly recognized and treated, the margin of safety is very slim, and initial care dictates the final result with varying degrees of severity. Chest injuries occurred in almost 70%–80% of RTAs. Sternal fractures are common due to steering wheel injuries in blunt trauma to the chest. 7 It was found that thoracic injuries were common, affecting about half of all trauma patients. Demirhan et al. observed that the mortality rate was 6.8%, and the morbidity rate was 3.3% among chest trauma patients in their study. 8 High mortality was explained by the multisystem injuries sustained by victims, among which the head injury is the most common associated lethal injury.
Age and Gender
In this study, the majority were in the age group between 21 and 40 years (N = 132 and 43%), that is, 21% of victims were aged between 21 and 30 years, followed by 22% between 31 and 40 years. Victims of extreme of ages (<10 years and >60 years) were fewer. Males outnumbered their female counterparts with 84% of fatalities, which was reflected in a study in Wardha where the most commonly involved age group was 21-40 years, with males outnumbering the females in a ratio of 6.7:1. 9 Minimum cases in the extremes of ages could be related to the care taken by the accompanying people and less mobility in this age group. B. Shetty et al. 10 and Katageri et al. 11 mentioned that the male-to-female ratio is more than 6:1 and 7.5:1, respectively, and commonly noticed between 21 and 40 years. Male preponderance is explained by the fact that the males work outdoors more compared to their female counterparts to earn a livelihood and are involved in driving, traveling, etc. Meera and Nabachandra 12 in their study of 120 cases of blunt thoracic injuries observed that the commonest age group of the victims was between 21 and 30 years, while the study by Abdul Raoof et al. 13 in 2019 found that the most commonly affected age group in chest trauma was 30–40 years (31%) and the commonest causative agent was RTA (71.4%), followed by firearm injury (19.4%).
Manner of Causation
In our study, the most observed manner of injuries were RTAs (65%), followed by railway injuries (16.6%), assault (10.5%), and falling from height (4.9%). This was in accordance with the studies8, 13 where in 65% of cases, blunt injury to the thorax was mostly related to traffic accidents. Partial agreement was observed with a study 12 in which vehicular accidents were the leading cause of blunt trauma to the thorax (86.40%), followed by assault by blunt weapon (8%), while another study 9 stated that vehicular accident was the leading cause of fatalities in 66.48%, followed by railway accidents in 19.55%, and domestic accidents in 3.91%. In a study on thoracic injuries in RTA victims by Agnihotri and Agarwal, 14 the most common victims were pedestrians (76), motorcyclists (15), cars (6), and cyclists (5), The pattern seen in external thoracic injuries was contusion in 58, abrasion in 32, laceration in 10, and incised wound in four cases in the same study.
Bad roads, speeding, inadequate and unscientific traffic planning, low use of helmets, consuming alcohol, using phone while driving, and violations of the traffic rules have contributed to much of the occurrences of RTAs. This may be explained by the fact that RTAs constitute a complex phenomenon with multiple causative factors. The rise in the number of RTAs can be attributed to the rashness of the drivers and carelessness of pedestrians, tiredness, fatigue of the drivers, and poor visibility due to a lack of street lights, rapid urbanization, and tremendous growth in road transport.
Period of Survival of Victims
In this study of 306 autopsied cases with thoracic injuries, 54% of victims died on the spot, 38% died while undergoing treatment in the hospital, and 8% died during transportation. Regarding time interval, 178 cases died between 0 and 6 hours after trauma (58%), 87 cases died between 6 and 24 hours (28%), 32 cases died between 24 and 48 hours (10.5%), and nine cases died after 48 hours (3%). A study in 2012 on various patterns of injuries due to falling from height observed that in 57.69% of cases, death occurred on the spot. 15 The percentage of victims of thoracic trauma who died at the place of incidence was 47% in a study by Meera and Nabachandra, which is similar to our study. This study is also comparable to one in Vijaypur (2016), which showed 48 of 104 cases of deaths due to chest injuries had died on the spot, while 33 cases died on their way to the hospital and 21 cases died while undergoing treatment in the hospital. 16 Deaths occurring within the first few hours may be due to the grave injury itself, which rapidly progresses to death. Deaths that occur between the first few hours of trauma and the next 24 hours result from secondary complications. In cases of survival for two or more days, apart from the primary injury, the associated infection, metabolic and nutritional disorders may play a role in causing death.
Pattern of Injuries
Similar to many studies9, 11, 12, 16 on the chest injuries, rib fracture was the most common skeletal injury in thorax in our study (55.8%), followed by the fracture of the clavicle (8.2%). The fractures of sternum and thoracic vertebrae occurred in 8% and 4% of cases, respectively. In injuries to the thoracic cavity, the lung is the most injured organ involved in 77 cases, followed by heart in 24 cases, which is similar to an autopsy-based study in Pune. 17 Diaphragmatic and aortic ruptures and stab wounds of the aorta were seen in eight cases. Lungs are easily injured as they occupy most of the space in the thoracic cage, making them more vulnerable to injury from trauma. This study is comparable with studies where blunt chest trauma in vehicular accidents in nearly 50% of the cases was associated with ribs and sternal fractures.12, 13
Chest wall bones were the commonest bones to have been fractured in most types of victims of RTA, but pelvic and limb bones were also more commonly involved in pedestrian victims as compared to other types of victims of RTA. 18 Our study disagrees with Ismail and al-Refaie; in their study over a period of 10 years examined 472 victims and observed rib fractures in only 23.9% of cases, pulmonary contusions in 27.1%, and lacerations in 6.9% of cases. 19 The lung (61%) was the most common organ involved in the chest trauma, as per many studies.10–14 Bhimrao et al. 20 in their study on injuries from RTAs noted that the thorax was more commonly involved than the abdominal region and abrasion was the commonest external injury, followed by contusion and laceration.
Association of Other Injuries
The associated bodily injuries contributing to death were head injuries in 45.3%, limb injuries (fractures) in 23.6%, and neck in 10% of cases. Our study varies slightly with the study by Aggarwal et al. 21 who conducted a study on 100 cases of RTA referred for autopsy in Patiala and found that the most common site involved was head and face (85%) followed by lower limb (65%) and upper limb (54%). Head injury was the most common injury, present alone in 130 cases (46%) and in 220 (78%) cases along with other injuries in a study on RTA victims in Bhopal. 22
Distribution of Accident Cases with Chest Injuries
Pedestrians (24.4%), followed by two-wheeler occupants (18%), four-wheeler occupants (16%), and auto (5.2%), were the commonest victims involved in RTA and most of the patients succumbed on the way to hospital (56%) as observed in our study. A study on deaths due to RTA revealed that pedestrian injuries are seen in 38.3% of the victims, motor vehicles in 28.1%, and motorcycle crash in 19.9%. 19 Motorcyclist occupants formed the largest group (28.84%) followed by the pedestrians (25%) in a study in Chitradurga, Karnataka 11 where pedestrian had sustained head injuries (84.61%). This can be explained by the fact that majority of the road users are pedestrians thus exposed to higher risk of accidents.
With regard to agents causing thoracic injury in this study, heavy motor vehicles (HMV) constituted 28% followed by train 16.6%, light motor vehicles (LMV) 14%, and two-wheelers 9% and firearms (7%) (Figure 1). A study 10 mentioned that HMV constituted 44.4% which is similar to this study, while another study 13 noted LMV (car) as the commonest offending vehicle in 36.3% of cases, followed by HMV (truck) in 29% and two wheelers in 14.5% of cases. Two-wheelers were the commonest type of victim’s vehicle in contrast to HMV (truck/bus) as the major type of offending vehicle causing thoracic injuries in RTA, as claimed by Bhimrao et al. 20 while four wheelers (46.9%), followed by two wheelers (37.9%), were the vehicles involved as in a study in Northeast India. 23
Causes of Death
It is well known that head injury is the leading cause of death in trauma patients. Head and neck (56.2%) were the commonest sites of injury associated with chest injuries followed by limb fractures (23.6%) in our study. Hemorrhagic shock (51.5%) was the main cause of death in thoracic injuries, followed by trauma to the head (27%) and poly trauma (13.6%). Study by Dhillon et al. was identical to ours in that hemorrhagic shock was the cause of death in the majority of the victims. 24 Meera and Nabachandra stated that the commonest cause of death was hemorrhagic shock in chest trauma combined with head injury in 48.8% of cases. 12 The high percentage of deaths was due to severe hemorrhage from rib and sternal fractures with associated injury to vital organs like the heart, lung, liver, and spleen and injury to great vessels. 8 Gupta et al. concluded that head and neck injuries were responsible for most deaths (70%) in their study on two-wheeler accident cases in Davanagere (Karnataka), though the commonest thoracic injury in riders and pillion riders was rib fracture. 25
Diurnal Variation
From this study, it was observed that the maximum number of cases were reported between 6 pm and 12 am (29%), followed by 6 am and 12 pm (27%), 12 pm and 6 pm (25%), and the least were found between12 am and 6 am (17%). The reason for the occurrence of more number of incidents, especially during the hours of late evening and night, may be due to poor visibility of drivers, due to sudden focusing of headlights of opposite vehicles, tiredness and exhaustion of the drivers, and being unaware of the bad/risky road conditions during the journey. It was noticed that, in a study on RTA victims in 2017, most of the accidents occurred in the afternoon hours between 12 pm and 6 pm, followed by late evening. 23
Conclusion
Trauma in the form of accidents, assaults, and railway injuries is the most dreaded problem in present-day society. This study concluded that RTA is the most common cause of chest trauma, followed by railway injuries. Males in the productive age group (21–50 years) are most susceptible to chest trauma, as they are more involved in work, driving, or traveling. The fatality rate in chest trauma cases depends on the severity of thoracic injuries and associated injuries like head injuries as contributing factors. Rib fracture is the most common thoracic wall injury, and lung laceration is the most commonly seen intrathoracic lesion.
The increasing incidence of trauma and accident cases is adding more burden to the autopsy workload of the tertiary care hospitals and justifies the need for appointing emergency physicians and medico-legal experts both at primary and secondary health care centers to effectively cater to the trauma cases. The mortality due to trauma cases can be decreased if victims are transported to a trauma care center nearby at the earliest. The fact that majority cases were spot deaths affirms the urgency and priority of having a robust pre-hospital trauma care and quick ambulance services.
Good awareness about the traffic rules and helmet use, both among riders and pedestrians, helps in the prevention of RTAs. Public education regarding the ill effects of speed driving, drunken driving, and the usage of phones while driving should be given. Improving road conditions and training the public on pre-hospital management of trauma and basic life support (BLS) can go a long way in saving many more lives.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institution’s Ethics Committee (IEC) was taken on November 26, 2014, prior to starting the study (as shown in Appendix A, page no.17).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.