
Abstract
This study investigated the socio-demographic characteristics and anatomical patterns of abdominal injuries among victims of road traffic accidents (RTAs) in Nairobi, Kenya, using autopsy findings. Conducted at Nairobi City Mortuary over a one-year period (July 2009–June 2010), the study examined 2,278 cases of violent deaths. Of these, 474 cases (20.8%) involved abdominal injuries, with 104 cases (21.9%) attributed to RTAs. The majority of victims were young adults, with a mean age of 29.04 years (range 12–59), and the most affected age group being 30–39 years. Males were disproportionately affected, accounting for 84.6% of cases, resulting in a male-to-female ratio of 5.5:1. Pedestrians constituted the largest proportion of victims (37.5%), followed by bicyclists (14.4%), highlighting their vulnerability in traffic environments. A total of 340 abdominal injuries were identified among the RTA victims. The most frequently injured structures included the liver (15.9%), lumbar vertebrae (15.9%), intestines (15.3%), stomach (14.7%), and abdominal aorta (14.1%). These findings demonstrate that abdominal trauma from RTAs commonly involves solid organs, hollow viscera, vascular structures, and skeletal components.
The study concludes that RTAs are a major contributor to fatal abdominal injuries in Kenya, particularly among young male pedestrians and cyclists. It underscores the need for comprehensive autopsy evaluation of all abdominal structures and calls for targeted road safety interventions, improved infrastructure, and policies aimed at protecting vulnerable road users to reduce mortality and injury burden.
Introduction and Literature Review
Abdominal injuries represent a significant proportion of traumatic injuries, being the third most commonly affected region in trauma cases, accounting for approximately 7%–10% of all trauma-related fatalities. 1 The mortality rate from abdominal injuries is high, with estimates around 17%, 2 and the morbidity associated with these injuries can range from organ damage to life-threatening conditions, due to the functional importance of the organs and major blood vessels contained within the abdomen. 3 Furthermore, diagnosing abdominal injuries presents significant challenges, often referred to as the “black box” of trauma, because these injuries can be asymptomatic or have nonspecific symptoms in the early stages. 4 The high mortality rates associated with abdominal injuries make them an urgent public health issue, particularly in regions with limited access to advanced medical care, such as Sub-Saharan Africa (SSA). 5
In the context of SSA, road traffic accidents (RTAs) have become one of the leading causes of abdominal injuries. RTA-related fatalities continue to rise in SSA, and Africa has the highest rate of road traffic injury (RTI) deaths globally. 6 In particular, RTAs are projected to become the leading cause of death for children aged 5–15 years and the second leading cause of premature death in the region. 7 In SSA, road injuries are the 7th and 8th leading causes of death in males and the overall population, respectively, and the 10th leading cause of healthy life years lost. 8 These injuries disproportionately affect the socioeconomically disadvantaged populations, with limited access to healthcare, poor infrastructure, and inadequate resources to respond to the problem. 9 Kenya, in particular, has one of the highest and fastest-growing rates of RTAs in the world, contributing significantly to the nation’s public health burden. 10
The issue of RTAs in Kenya is compounded by the country’s rapidly increasing urbanization, which has led to high traffic congestion and, consequently, higher risks for both vehicle occupants and pedestrians. As the capital city, Nairobi becomes more congested, the rates of traffic accidents and their resultant injuries—particularly abdominal trauma—are rising steadily. The lack of comprehensive studies characterizing RTA-related abdominal injuries in Kenya has hindered the development of targeted, context-specific interventions to improve patient outcomes in cases of abdominal trauma resulting from RTAs. A detailed understanding of the magnitude, age and gender distribution, and anatomical patterns of these injuries is crucial for formulating appropriate responses.
In India, where RTAs also present a major health issue, the pattern of abdominal trauma due to road accidents shows similar trends. Studies have reported that young males are the most affected demographic, with pedestrians and cyclists being particularly vulnerable. 11 The age distribution of RTA victims in India aligns with those in other developing nations, with a substantial proportion of victims in the 30–39 years age group.12, 13 Indian studies also show that the most common abdominal injuries caused by RTAs include liver and intestinal injuries, which are similar to findings from SSA, including Kenya.14, 15
Furthermore, studies in India have highlighted a significant concern regarding the lack of pedestrian infrastructure and the failure to enforce traffic laws, both of which exacerbate the impact of RTAs, particularly on vulnerable populations such as pedestrians and cyclists. 16 Similar patterns are observed in Nairobi, where the absence of dedicated pedestrian lanes, traffic calming measures, and speed control mechanisms contributes to a high rate of pedestrian injuries. 17 This suggests that urban planning and policy reforms targeting pedestrian safety could have significant benefits in reducing RTA-related abdominal trauma in Kenya as well.
In summary, the current study aims to describe the magnitude, age and gender distribution, as well as the anatomical profile of abdominal injuries resulting from RTAs in Nairobi, Kenya. These findings will help fill the gap in local data and provide essential information to inform the development of more effective, data-driven interventions to reduce RTA-related abdominal injuries in the region. Additionally, by comparing trends with Indian studies on RTA-related abdominal trauma, the study hopes to provide broader insights into regional differences and shared challenges in managing these injuries.
Materials and Methods
This was a prospective descriptive autopsy study done at Nairobi city mortuary, the largest national referral forensic autopsy Center that receives cases from Nairobi county and its environs. Bodies which had recognizable body regions, parts and organs received within 72 hours were examined over a period of 1 year between July 2009 and June 2010. Sociodemographic data, place, circumstances and cause of trauma obtained from the relatives and police officers were recorded on standard forensic autopsy proformas. The cases were categorized into male and female, and then divided into eight (8) 10-year age groups: 1–9, 10–19, 20–29, 30–39, 40–49, 50–59, 60–69, and ≥70 years. Physical examination was done, starting with external features such as lacerations, bruises, wounds and blood stains. Dissection was then done according to the procedure by Rokistansky 8 where each of the anatomical structures was examined for location, extent and type of injury.
The abdominal contents were eviscerated en bloc by cutting through the esophagus, aorta and inferior vena cava superiorly and recto-sigmoid function inferiorly, dethatching the organs from the posterior abdominal wall and thoracic diaphragm. The abdominal block was carefully examined for individual organ involvement, paying attention to the solid organs, namely the liver, spleen and kidneys, as well as hollow organs like the stomach, small and large intestines. The aorta and inferior vena cava were also examined. The musculoskeletal envelope that remained was also examined for fractures and dislocations of the lumbar vertebrae.
These data were entered, analyzed and managed through the Statistical Package for the Social Sciences (SPSS) to generate descriptive statistics. The distribution of anatomical structures by age and gender was determined using frequencies and percentages.
Results
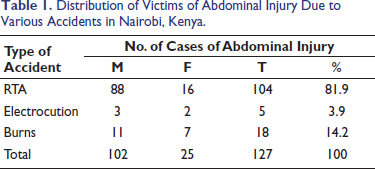
Out of the 2,278 cases of violent deaths, 474 (20.8%) of the victims sustained abdominal injury, indicating that the abdomen was the third most frequently injured region after the head and chest. Out of these 474, 127 (26.8%) were due to accidents, 104 (81.9%) of which were caused by RTA. This shows that abdominal injuries comprise about 4.6% of the total cases of violent deaths, and that RTA comprises 81.9% of accident-induced abdominal injuries (Table 1).
Distribution of Victims of Abdominal Injury Due to Various Accidents in Nairobi, Kenya.
Age and Gender Distribution
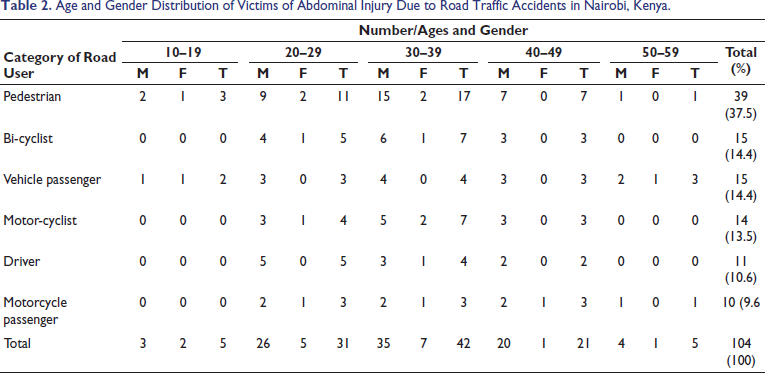
The mean age was 29.04 years, ranging from 12 to 59 years. The most frequently affected age group was 30–39 years (42; 40.4%), followed by 20–29 (31; 29.8%), then 40–49 (21; 20%). The 10–19 and 50–59 had equal numbers (5:4.8% each). Notably, there were no children aged below 10 years, and no elderly people aged over 60 years. Pedestrians and passengers were more widely spread across the age groups, clustering mostly at 30–39 years (17; 43.6%) and 4 (26.7%) respectively. Bicyclists, motorcyclists, and drivers largely clustered around 20–49 years.
Of the 104 victims of abdominal injury, there were 88 males and 16 females, giving a male: female ratio of 5.5:1. This male predominance persisted in the age groups 20–29 and 30–39 years. In the 40–49 age group, the M:F ratio was 20:1. Of the 16 females, 12 (75%) were clustered in the 21–39 year age group, the other age groups only having 1 or 2 victims (Table 2).
Age and Gender Distribution of Victims of Abdominal Injury Due to Road Traffic Accidents in Nairobi, Kenya.
Categories of Road Users
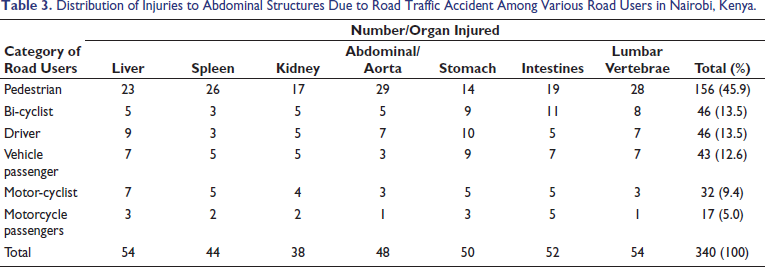
The most commonly involved category of road user was the pedestrian (39; 37.5%), followed by bicyclists and vehicle passengers (15; 14.4% each), then motorcyclists (14; 13.5%) and drivers (11; 10.6%). The least affected were motorcycle passengers who comprised only 10 (10, 9.6%) (Table 2). There was a total of 340 injuries in the abdomen. The highest number was among pedestrians (156; 45.9%), followed by drivers and cyclists (46; 13.5% each), then vehicle passengers (43; 12.6%). Motorcycle passengers were the least involved (17; 5.0%) (Table 3).
Distribution of Injuries to Abdominal Structures Due to Road Traffic Accident Among Various Road Users in Nairobi, Kenya.
Anatomical Distribution of Injuries
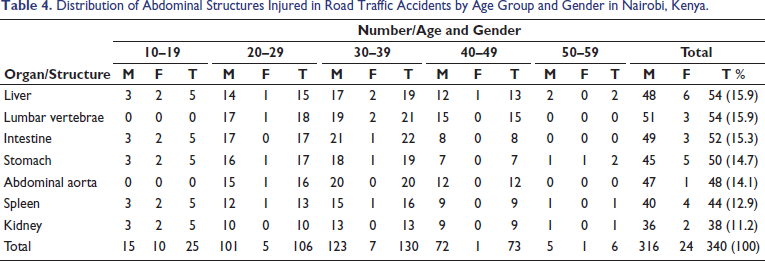
The 340 injuries involved digestive, urinary organs, vascular and skeletal structures. Of the digestive and urinary, the liver was the most commonly injured organ (54; 15.9%), followed by intestines (52; 15.3%), stomach (50; 14.7%), and then spleen (44; 12.9%). The kidney was the least involved (38; 11.2%). Lumbar vertebrae were fractured in 54 (15.9%), while the abdominal aorta was injured in 48 (14.1%) cases. When disaggregated for gender, the pattern varied somewhat. Among males, of 316 injuries, the intestines were the most commonly involved (49; 14.4%), followed by the liver (48; 14.1%), then stomach (45; 13.2%) and spleen (40; 11.8%). In the females, the liver was the most commonly involved (6; 25%), followed by the stomach (5; 20.8%), then the spleen (4:16.7%) (Table 4).
Distribution of Abdominal Structures Injured in Road Traffic Accidents by Age Group and Gender in Nairobi, Kenya.
When the category of road user was considered, individual structures involved varied. For example, among pedestrians for the 156 injuries, the abdominal aorta was the most commonly injured structure (29; 18.6%), followed by lumbar vertebral fracture (28; 17.9%), spleen (26; 16.7%), liver (23; 14.7%), intestines (19; 12.2%), then kidney (17; 10.9%). Among drivers, for 46 injuries the most commonly involved structures was the stomach (10; 21.7%) followed by liver (9; 19.6%); Aorta and lumbar vertebrae (7; 15.2% each), the kidney and intestines (5; 10.9% each), with the spleen being the least involved (3; 6.5%) (Table 3).
Discussion
Occurrence of Abdominal Injuries Due to RTAs
The findings of the current study reveal that 22% of fatal abdominal injuries are caused by RTAs. This result aligns with the findings of previous studies, which reported a similar proportion of 15%. However, it is lower than the higher frequencies observed in Tanzania (53.7%) 18 and Uganda (52%). 19 The variation in these statistics can be attributed to multiple factors, including the category of road users, the demographic profile of victims, and the traffic regulations enforced in different regions. For instance, the road infrastructure and the socioeconomic conditions of a region can greatly affect the prevalence of RTAs. In high-income countries, the frequency of fatal abdominal injuries due to RTAs might be lower due to better road safety regulations and infrastructure, such as pedestrian tracks and safer driving conditions. On the other hand, in developing nations, a lack of pedestrian safety and traffic law enforcement contributes to higher rates of such injuries.
The current study’s findings are similar to those reported in India, where RTAs are a major cause of fatal abdominal injuries, particularly among young males. Other studies have emphasized the need for timely intervention in cases of abdominal trauma resulting from high-velocity impacts. The study highlights that, in both African and Asian settings, the prevalence of young males suffering from abdominal trauma is considerable, further supporting the hypothesis that young males, especially those in the working-age group, are disproportionately affected by RTAs. The urban setting of this study and the emphasis on youthful demographics resonate with findings from Indian research, where young males are frequently involved in fatal RTAs.
Age and Gender Distribution of RTA Victims
The mean age of RTA victims in the current study was 29.04 years, with the most commonly involved age group being 30–39 years. This is consistent with age distributions reported in studies from Africa 20 and Asia, 5 but is younger compared to reports from Europe. 21 The absence of significant abdominal injuries in children below 10 years and adults over 60 years in this study is notable and contrasts with several studies that report a higher involvement of both older adults and children under 10 years in fatal abdominal injuries due to RTAs. This discrepancy can likely be explained by the urbanicity of the population under study, where young adults in the active working-age group are more commonly involved in road traffic collisions. The relative lack of injuries in younger children and elderly individuals might also reflect the differing traffic patterns in urban versus rural settings, where young and older people may not be as exposed to heavy traffic.
A critical factor contributing to this phenomenon, particularly in Indian studies, is the “young male syndrome,” which has been well-documented in forensic literature. This syndrome is linked to higher risk-taking behaviors, a higher tendency to violate traffic laws, more aggressive driving habits, and frequent alcohol and substance use. 6 Young male victims, aged 15–35 years, are the predominant demographic in RTA fatalities, which places a significant socioeconomic burden on the community, as this group is typically the most productive segment of society.
Categories of Road Users Involved in RTAs
The current study found that pedestrians comprised nearly 40% of RTA victims, followed by bicyclists (14.4%), with drivers being the least involved (just over 10%). This distribution mirrors the findings of Okemwa et al. in Nairobi but contrasts with reports from countries like Serbia, Nigeria, Ethiopia, and Turkey, where vehicle occupants (drivers and passengers) predominate.22, 23 This variation can be attributed to the differences in road infrastructure between high- and low-income countries. In many developing countries, pedestrian and cyclist tracks are either poorly developed or non-existent, and vehicles often dominate the roadways, leading to a higher rate of accidents involving pedestrians and cyclists.
In India, pedestrians are the most vulnerable road users, making up over 35% of RTA victims in urban centers. The lack of proper pedestrian infrastructure, such as dedicated pedestrian tracks and safe crossings, is a key factor contributing to the high mortality rate among pedestrians. The absence of cyclist lanes and the poor enforcement of speed limits exacerbate this issue. Educational programs, engineering measures, and legislative interventions, such as the construction of safer pedestrian and cyclist paths, have been proven to reduce road trauma events in many countries and should be prioritized in urban areas.
Conclusion
RTAs are a major cause of fatal abdominal injury. They predominantly involve young males, especially pedestrians, and cause injury to hollow digestive organs, the abdominal aorta and lumbar vertebrae. Evaluation of RTA victims for abdominal injury should therefore include digestive, vascular and skeletal structures. We recommend the mainstreaming of pedestrian and bicycle tracks on city roads.
RTAs remain a major cause of fatal abdominal injuries, particularly involving young males, pedestrians, and cyclists. These injuries frequently affect the liver, intestines, stomach, abdominal aorta, and lumbar vertebrae. Given the severity and high mortality associated with these injuries, it is crucial to comprehensively evaluate RTA victims for abdominal injuries, including vascular and skeletal structures. Preventive measures should prioritize pedestrian and cyclist safety, particularly in urban areas, through the development of pedestrian tracks, cyclist lanes, and improved traffic law enforcement.
Recommendations
Enhanced Road Safety Infrastructure
One of the primary recommendations is the improvement of road infrastructure, particularly the creation of dedicated pedestrian pathways and cyclist lanes. In this study, pedestrians made up nearly 40% of the victims, highlighting the vulnerability of non-motorized road users. The implementation of pedestrian overpasses, subways, and safe crossings would significantly mitigate pedestrian-related fatalities. Similarly, cyclists need more dedicated tracks to reduce collisions with vehicles. In urban areas, where traffic congestion is high, these measures are crucial in protecting vulnerable road users. Investing in traffic calming measures, such as speed bumps, pedestrian signals, and better road signs, would also reduce the frequency of fatal accidents.
Legislation and Strict Law Enforcement
There is an urgent need for stricter enforcement of existing traffic regulations. In particular, the study underscores the importance of speed limit enforcement and the use of seatbelts for all road users. Studies from India (Patel et al., 2021) and other countries have shown that speed-related accidents account for a substantial proportion of RTAs, particularly involving pedestrians and cyclists. The mandatory use of helmets for cyclists and motorcyclists, and stricter laws governing the use of mobile phones while driving, should be enforced with regular checks. Police and law enforcement agencies must take a more active role in monitoring road safety behaviors, and penalizing those who violate these safety norms.
Public Awareness and Educational Campaigns
Increasing public awareness about the risks of RTAs and the importance of safe road behaviors can significantly reduce the number of injuries. Educational campaigns aimed at young males, who are disproportionately affected by RTAs, should focus on the dangers of reckless driving, the importance of wearing seatbelts, and the risks of substance abuse and distracted driving (e.g., mobile phone usage). Schools, universities, and workplaces should be involved in road safety education to target a wide demographic, particularly those at higher risk. Public service announcements, social media campaigns, and workshops on road safety can help instil safer habits in drivers and pedestrians alike.
Improved Medical Response and Trauma Care
Given the high mortality rate associated with abdominal aortic injuries (AAI) and lumbar spine fractures, it is essential that emergency medical services (EMS) and trauma care units are adequately equipped to handle such injuries. Medical personnel should be trained to recognize and address these injuries early, especially in high-impact motor vehicle accidents (MVAs). The study found that lumbar vertebral fractures and abdominal vascular injuries frequently co-occur, necessitating a more comprehensive trauma assessment. Trauma centers should adopt a multidisciplinary approach, including vascular surgeons, orthopedic specialists, and emergency physicians, to address complex injuries. Prompt diagnosis through advanced imaging (CT scans and MRIs) is critical in the management of such trauma.
Urban Planning and Pedestrian Safety
Urban planning in high-density areas should prioritize pedestrian safety through the incorporation of pedestrian zones, crosswalks, and traffic signals that protect pedestrians from high-speed vehicles. Ensuring that major intersections and busy roadways are designed with pedestrian safety in mind will help decrease pedestrian-related fatalities. Moreover, public transport systems should be improved to reduce the number of pedestrians and cyclists on busy roads. As highlighted in the study, the lack of pedestrian infrastructure in many cities is a significant factor in pedestrian-related fatalities. Cities should embrace walkability as an important urban design goal, creating environments where walking and cycling are safe, convenient, and accessible.
Focus on Vulnerable Road Users: Pedestrians and Cyclists
Special attention must be given to pedestrians and cyclists, who are among the most vulnerable road users. In countries like India, where the prevalence of non-motorized transport is high, targeted interventions are needed to protect these individuals. This includes better pedestrian crossings, traffic control devices, and segregated cycling lanes. Government policies should focus on improving accessibility and safety for pedestrians and cyclists, which is especially important in cities where pedestrian and cyclist traffic is substantial. Moreover, enforcing cycling helmet use and making reflective gear mandatory for night cycling would reduce fatalities among cyclists.
Data Collection and Research Expansion
Expanding research on the epidemiology of abdominal injuries due to RTAs can help improve the understanding of injury patterns, enabling more accurate predictive models for preventive strategies. Collecting detailed national and regional data on RTAs and trauma outcomes is crucial for developing targeted injury prevention strategies. Public health organizations should prioritize longitudinal studies that assess the impact of traffic safety interventions, allowing for the continuous improvement of road safety measures. Researchers should also examine the long-term impact of RTA-related abdominal injuries, focusing on post-trauma care and the socioeconomic costs associated with such injuries.
Integration of Technology for Traffic Management
The use of intelligent traffic management systems can play a vital role in preventing RTAs and reducing fatalities. Advanced traffic monitoring technologies, including surveillance cameras, speed detectors, and real-time traffic updates, can help control traffic flow and detect dangerous driving behaviors in real-time. Additionally, the incorporation of vehicle safety features such as collision detection systems and autonomous braking can mitigate the severity of injuries during an accident. As technology continues to evolve, cities should prioritize smart city initiatives that leverage digital solutions to enhance road safety.
Promote Safe Driving Culture
The promotion of a safe driving culture is essential for reducing fatal injuries caused by RTAs. Public education campaigns should emphasize the importance of responsible driving, particularly regarding the risks of speeding, distracted driving, and driving under the influence. Driving schools should integrate safe driving principles into their curricula, ensuring that new drivers are adequately trained to understand the legal, social, and health consequences of unsafe driving. Moreover, insurance companies should incentivize safe driving practices by offering discounts or benefits to drivers who maintain a clean record.
Policy Advocacy for Vulnerable Road Users
Governments and non-governmental organizations (NGOs) should advocate for policies that prioritize the safety of vulnerable road users (e.g., pedestrians, cyclists, and motorcyclists) in road planning and design. Ensuring that laws and regulations are tailored to protect these groups can have a profound impact on reducing RTA fatalities. Additionally, collaboration with urban planners, engineers, and community leaders is necessary to implement community-based interventions that create safer streets for all.
Footnotes
Acknowledgments
The Nairobi city mortuary management should allow access to the morgue and facilitate the autopsies.
Authors’ Contributions
Wangai Kiama conducted the autopsies, collected the data, analyzed the data, discussed, and recommendations. Moses Obimbo, Edward Muge, and Julius Ogengo contributed to the alignment of the results to the literature review, discussion and recommendations.
Availability of Data and Material
All data generated or analyzed during this study are included in this published article.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Approval for the study was sought and granted by the Kenyatta National Hospital Ethics and Research Committee (REF: KNH/UON-ERC/A/196). Authority to conduct the study was sought from the Medical Officer of Health (MOH), Nairobi City Council, and permission was obtained from the Superintendent and pathologist in charge of the City Mortuary. Autopsies were conducted with adherence to ethical procedures that included consent from the relatives and confidentiality of the information gathered. Coding of the information was done to delink the samples from the source. The Datasheets were handled confidentially.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.