
Abstract
In India, autopsy of bodies brought to mortuary are conducted by medical officers or by forensic medicine experts. During autopsy, doctors usually preserve all objects found on or in the body of the deceased, which may have anything to do with the cause of death, or which may furnish clues useful in the apprehension and conviction of the assailant. However, in difficult situation regarding cause of death, mode of death and manner of death, the dead body is referred to the Department of Forensic Medicine and Toxicology (FMT) to conduct autopsy. In firearm injuries, bullet retrieval from the body and determination of the missile trajectory may also be useful to for judicial authorities, security forces. We present a case where the body after partial autopsy was referred to FMT in want of retrieval of projectile, and thus highlighting the role of forensic medicine expert and practical knowledge of FMT at the peripheral level.
Introduction
The word ‘Autopsy’ is derived from two terms ‘autos’ that is self and ‘opsis’ that is examination (self-examination). 1 Traditional autopsy has changed little in the past century and consists of the external examination, evisceration and dissection of major organs with identification of macroscopic pathologies and injuries and histopathology if needed. All deaths of unnatural (homicide, suicide, accident) manner, suspicious deaths and unexpected deaths necessitate a legal investigation, which includes an autopsy as a portion of the evidence-gathering process. 2 Gunshot injuries to the spine make up the third most common cause of spinal injury 3 Postmortem radiography is an essential component of firearm injury examination. Anteroposterior and lateral radiographs assist in determining the location, nature and path of projectiles in the body, 4 and the lodged evidence can be collected and handed over to investigating agencies.
Brief History
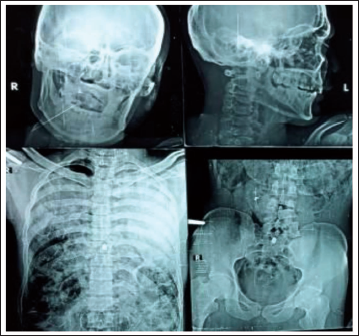
An autopsy was conducted in reference to application by the police personal with alleged history of firearm injury, at subdivisional hospital by board of medical officers. The body was opened from anterior and posterior aspect for retrieval of projectile from the spine area. However, when bullets could not be retrieved, the case was referred to the Department of Forensic Medicine and Toxicology (FMT) with the remarks that both bullets cannot be traced so needs forensic expert opinion, and there is no expert or surgeon to recover the bullet from the dead body for evidence purpose, for maintaining law and order situation. In the Department of FMT, digital X-ray were conducted which showed the presence of two projectile and marks of opening of body of vertebrae. The findings on postmortem were as under and both the bullets thus recovered were sealed and handed over to police.
Case Findings
We received a dead body of male individual wrapped in a transparent plastic sheet and white cloth; the dead body was wearing a blackish colour and greenish floral design underwear with elastic waist line around the waist, and a black colour tagdi around the waist. Along with the body following clothes were lying loosely: a grey colour lower with greenish border at margins and lateral aspect was lying loosely over the body; a bluish white colour full-sleeved shirt with two front pockets on either side with buttons intact. On the right front region aspect, two holes with inward edges of size 1.2 cm X 1 cm respectively were located at level of 17 cm and 34 cm from lower margin. The shirt was smudged with blood at places. The holes were corresponding with the firearm injury marks on the body.
The anterior part of the chest wall and the abdominal wall was stitched for a length of 41 cm extending from the mid-chest region till the supra pubic region (Figure 1). On the posterior aspect over the spinal region, a stitched area of length 38 cm extended from the mid-scapular region till the lumbar area with 14 stitches with white thread. Neck was not dissected. Skull was not dissected (Figure 2); on dissection of the body, the whole of the thorax viscera below the tracheal bifurcation was eviscerated and lying loosely; further below the diaphragm the abdominal organs were eviscerated. All the organs were jumbled up and body was devoid of blood. The organs were further arranged in anatomical position. On examination of vertebrae, in thoracic level T-8 vertebrae, was broken in multiple pieces, and the first sacrum vertebrae were fractured at multiple places (Figure 3). The body was subjected for X-ray to locate the metallic fragment (Figure 4).
Anterior Aspect of Body with Stitch.

Posterior Aspect of Body with Stitch.

Chest Cavity with Broken T-8 Vertebrae.

X-ray Showing Projectile in Chest and Sacrum.
Injuries
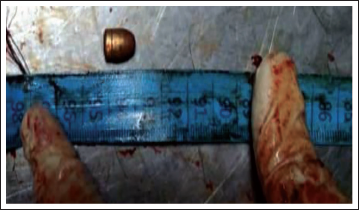
An entry wound of firearm of size 1.2 cm × 0.8 cm with abrasion collar around was present on the anterior right chest wall situated 129 cm from the right heel, 5 cm right to midline and 3 cm below and lateral to the right nipple (Figure 1). On dissection, it was fracturing the 7th rib in midclavicular line, lacerating the pleura, perforating the lower lobe of right lung, entering the heart at right ventricle and existing right atrium, to reach 8th thoracic vertebrae where fractured ends showed reddish infilteratiion of blood in exposed trabeculae. However, on dissection a yellow-coloured metallic bullet of size 1.2 cm × 0.6 cm was recovered (Figure 5). The track of the wound was directed upwards, medially and posteriorly. The fractured ends showed reddish infiltration of blood.
An entry wound of firearm 1.6 cm × 1 cm with abrasion collar was present on the right lower half of abdomen on its anterior aspect situated 107 cm from right heel, 8 cm right to midline and 10 cm above and medial to the anterior superior iliac spine (Figure 1); on dissection it was penetrating the peritoneal cavity, rupturing the large intestine in the ascending region, further entering into the right kidney lacerating it through and through, to reach till the sacrum and fracturing the sacral promontory into multiple pieces, in the body a deformed metallic yellow-coloured bullet was lodged of size 1.2 cm × 0.6 cm. The track of the wound was directed downwards, medially and posteriorly. The fractured ends showed reddish infiltration of blood.
Bullet Recovered from T-8 Level.
Internal
Scalp healthy and skull was healthy and intact. Meninges and vessels were intact. Brain was pale. Vertebrae and Spinal Cord were described. Pharynx & Oesophagus were described. Neck and Thyroid were healthy. Hyoid bone was intact. Larynx and trachea were healthy. Chest wall, ribs, Sternum and cartilage were right side described, left healthy. Pleura/pleural cavity were right side described, left healthy and Pericardium was ruptured due to bullet track. Right lung showed the track of bullet on its lower aspect and was lacerated. Left lung was intact. Heart as described. Coronary Arteries & large blood vessels were empty. Peritoneum, Retroperitoneum was described. Stomach and its contents contained 100 cc of undigested yellowish food material, preserved for chemical analysis. Small Intestine and its content contained semidigested food material and gases, preserved for chemical analysis. Large Intestine and its content contained faeces and gases, preserved for chemical analysis. Liver and Gall Bladder were pale, preserved for chemical analysis. Spleen was pale, preserved for chemical analysis. The pancreas was autolysed. The right kidney was described. The left kidney was pale and preserved for chemical analysis. The urinary bladder was empty.
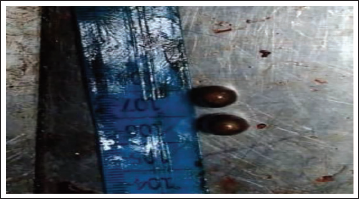
Cause of death is firearm injury as described and its complication. However, viscera have been preserved for chemical analysis, probable time between death and postmortem was 12–24 hours, both the projectiles were collected and handed over to the police (Figure 6).
Both Bullets Recovered from Thorax and Sacrum Area.
Discussion
The postmortem examination is the final service that a physician can render to a human being approaching the hospital premise. Its purpose is not just to establish medical diagnoses, but to provide facts in the service of the judicial process and the public interest. Its main tasks are the definitive ascertainment of death, determination of the cause of death and assessment of the manner of death. 5 While doing autopsy, it is mandatory that all the cavities need to be explored and collect the forensic evidence material and to preserve it. A doctor is often either unaware of or has a rather lax attitude toward the potential medicolegal ramifications and significance of the autopsy report. 6 Doctors balance workload burdens of autopsies with substitute like external examinations, partial autopsies and other limited variants for complete autopsies, as observed in this case. However, the quality of forensic autopsy activity is always questioned in courts of law; incorrect assessments are dangerous because they can jeopardise the validity of a criminal investigation and thus affect the outcome so that a real culprit may be acquitted or an innocent person convicted. Nonconformities also discredit the professionalism of the specialist who performs the autopsy. 7 Partial autopsies, by definition, do not provide complete descriptions of the extent of disease and nature of any injuries. A time-honoured aphorism is relevant: ‘Partial autopsies provide partial answers’. Will the partial answer be sufficient? 8 As was observed in this case, and thus the metallic projectiles could not be retrieved due to lack of basic human anatomy and autopsy skill, as different levels of vertebrae were dissected to search for the bullet. Only advantage is that they can be completed more quickly—the examination of the body takes less time, as was done in this case. Thus, an evidence-based approach guided by three forensic autopsy goals—statutory duty, the creation of a minimal dataset for societal and governmental inquiry, and maintenance of practitioner competency—ensure the completeness of any one postmortem examination. 9 Following observation was made by the Honourable Court ‘the service rendered by the Forensic Medicine Experts in this regard is unique and deserves for admiration, but the real state of affairs remain that medicolegal cases are handled in this country by the nonforensic experts and none could be blamed in this regard’ 10 as was observed in this case.
Conclusion
Though a fresh medical undergraduate is anticipated to come out from the institution with the knowledge in clinical and surgical areas of medical science, yet, he/she should not be lagging behind in the field of FMT. Further, the knowledge of medicolegal aspect on the part of medical officers is of utmost significance for Justice Delivery System. Thus, National Medical Commission, 11 statutory body for formulating guidelines in Medical Education in India, has made internship mandatory exclusive in the Department of FMT, which will be a stepping stone in further enhancing the medicolegal knowledge in budding doctors at peripheral level.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.