
Abstract
Background
During the first wave of the new coronavirus (COVID-19) pandemic, the sudden increase in hospitalised patients put medical facilities in southern Switzerland under severe pressure. During this time, bachelor’s degree programs in nursing, physiotherapy and occupational therapy were disrupted, and students in their second year were displaced. Students experienced the continuous reorganisation of their traineeship as healthcare facilities adapted to a climate of uncertainty.
Purpose
The aim of this study was to investigate the degree of moral distress and the ethical issues most often encountered by physiotherapy, nursing and occupational therapy students enrolled in a traineeship during the first wave of the COVID-19 pandemic in southern Switzerland.
Participants and research context
The sample consisted of 102 participants, and the response rate was 81.6%.
Research design
Based on a pragmatic approach, a mixed-method with a convergent design was adopted. Data were collected between 30 April 2020 and 14 May 2020, via a survey administered to all occupational therapy, physiotherapy and nursing students in their fourth semester.
Ethical considerations
Given that no vulnerable persons were involved, the Ethics Committee of Southern Switzerland waived authorisation. However, all measures were put into place to protect participants by guaranteeing their anonymity and confidentiality.
Results and discussion
The data analysis showed that the main source for moral distress was ‘poor teamwork’ and that the moral issues encountered most often by students were related to the appropriateness of care and working conditions, with a clear reference to students’ own safety and that of their loved ones; the other concerns reported included the loss of learning opportunities and the perceived lack of technical knowledge and skills.
Conclusions
This survey offers a faithful overview of physiotherapy, nursing and occupational therapy students’ experience during the first pandemic wave. This study also identifies some key recommendations for healthcare professions’ education.
Introduction
During the first wave of the new coronavirus (COVID-19) pandemic, southern Switzerland found itself vulnerable, and the healthcare system had to be reorganised. Bachelor’s degree students in nursing, physiotherapy and occupational therapy started their regular second internship on 10 February 2020 when no cases were yet known in Europe.
The educational needs for nursing students with respect to epidemics have been the subject of a recent literature review conducted by Goni-Fuste et al. 1
In the review, five themes that recur in the literature were highlighted: (1) education (maintaining flexible teaching modes by alternating online classes with face-to-face classes), (2) knowledge and concerns about the risk and preventive measures, (3) willingness to serve during the outbreak of an epidemic, (4) emotional impact of the epidemic on students and (5) ethical issues. 1 One of these ethical issues was discussed by Hayter and Jackson 2 in their critical editorial that questioned the appropriateness of employing nursing students during the pandemic, suggesting that it might be better, for the students’ safety, to employ them elsewhere while freeing up more experienced professionals to care for patients affected by the virus. Although they pointed out in their editorial that all students involved in the care of patients with COVID-19 in the UK did so voluntarily, the students may have been more or less explicitly pressured. 2 Hayter and Jackson’s doubts about students’ volunteerism were partly confirmed in a study carried out by Gómez-Ibáñez et al., 3 which aimed to investigate the experience of nursing students during the first wave of the pandemic. From their results, it is clear that the students decided to accept strong social pressure. 3 However, there is not only external but also internal pressure when tension is created and leads individuals to decide to engage in threatening circumstances. In fact, the willingness of colleagues to work in dangerous conditions influences the willingness of an individual.4–7 However, being able to actively contribute during a pandemic can also be the result of genuine motivation that has a positive impact on students. 8 Nevertheless, ethical issues in this respect are not only about whether to employ students to deal with health crises due to epidemics.
Background
The term moral distress was first used in the literature by Jameton; 9 however, its definition has been revisited several times. McCarthy and Deady 10 state that moral distress arises when individuals are unable to act in accordance with their own moral judgement regarding what the right course of action should be. Hamric 11 offers a classification of the constraints that can give rise to moral distress as follows: (a) factors internal to the caregiver (perceived lack of power and lack of knowledge about possible alternatives or the situation); (b) factors external to the caregiver (insufficient staff, lack of administrative support and incompetent caregivers); (c) clinical situations (futile or unnecessary treatments, aggressive treatments that are not in the patient’s best interests, inadequate informed consent and lack of communication of the truth, such as giving false hope). However, the conditions for the moral distress to occur have gained a deeper understanding, broadening the understanding of moral distress as a reaction to constraints of action. Fourie 12 suggests that moral distress can rise in the case of moral conflict and uncertainty. Morley et al. 13 suggest that in order to occur, moral distress needs a causal relation between necessary conditions that are an experienced moral event and the experience of psychological distress.
Nursing students are not exempt from the phenomenon of moral distress. Sasso et al. 14 asserted that in addition to all of the above-quoted constraints that can provoke moral distress, there are situations related to the role of a student. Additionally, moral distress is exacerbated by the lack of resources and their questionable allocation, hierarchical structures and the feeling of not being able to influence the course of events. 14 In their qualitative research, Wojtowicz et al. 15 asserted that the main sources for moral distress among mental health nursing students were the lack of nursing staff’s awareness of the reasons underlying nursing intervention, strong hierarchy, especially with respect to physicians, and the feeling of being left alone by their instructors. 15 Unfortunately, there is a lack of literature on occupational therapy and physical therapy students.
Aim and research question
The aim of this study was to investigate the intensity and frequency of moral distress and the major moral issues encountered by physiotherapy, occupational therapy and nursing students during the first wave of the COVID-19 pandemic. Understanding their experiences might help improve healthcare students’ education, providing them with actualised support and knowledge.
Research question: What were the major sources of moral concern and distress among nursing, physiotherapy and occupational therapy students during the first wave of the pandemic?
Research design
Inspired by the pragmatic approach, we opted for a convergent design, including quantitative and qualitative data, which were collected and analysed simultaneously and had equal priority in the analysis. 16
Data acquisition
Data were collected through an online questionnaire, which combined sociodemographic questions, the Moral Distress Scale-Revised (MDS-R) by Hamric et al., 17 validated and translated version in Italian (I-MDS-R) 18 and additional questions derived from the available literature and issues reported in the media. Given that the I-MDS-R 18 is not specific to moral distress experienced in the context of COVID-19 and that it has a narrow understanding of moral distress, the authors decided to add specific questions to confer the consistency among the objectives of the study, the tool and the findings.
The questionnaire was created on the LimeSurvey platform (https://www.limesurvey.org/) and consisted of closed and open questions: • Three sociodemographic questions (gender, age and course). • Eight questions related to the last internship experience: (1) Were you infected by COVID-19? (2) Did you have to stay in quarantine? (3) During your last internship, did you work in a service that treated patients affected by COVID-19? (4) Were ethical issues related to COVID-19 discussed within the team? If yes, could you please specify these situations? (5) Were ethical issues regarding the materials, logistics, etc., related to COVID-19 discussed within the team? If yes, could you please specify these issues? (6) In the case that you discussed ethical issues within the team, could you please describe how these discussions took place (e.g. were they structured, unstructured or left to the individual initiative or to the team)? (7) Did you discuss COVID-19-related ethical issues that you encountered during your internship outside of the service in which you worked? (8) Did you take part in any discussion concerning advanced directives of patients with COVID-19? If yes, how did you experience these discussions? • The MDS-R by Hamric et al.
17
and validated and translated version in Italian (I-MDS-R).
18
The MDS-R can be administered to various healthcare professionals. 17 The authors produced a single scale applicable to all. The Italian version is composed of 14 items and uses a 5-point Likert scale (from 0 to 4). Total scores range from 0 (which is equivalent to no moral distress) to 16 (maximum intensity).
Data analysis
Quantitative analysis
Descriptive analysis was carried out to describe the sample and to understand the internship experience of the students. Further variance analyses were performed using nonparametric tests, specifically the Kruskal–Wallis test and the Mann–Whitney U test.
Moral Distress Scale-Revised analysis was performed in a stratified manner based on gender, study cycle membership and direct contact in the care of COVID-19 patients. In addition, to define high levels of moral distress, quartiles were used. Finally, ANOVA was used to compare participants with high levels of moral distress and intention to drop out of the internship or training. Exploratory factor analysis was performed to simplify and condense complex datasets based on the analysis of the correlations between variables in the questionnaires. The data shown in the tables refer to the factors with the higher explained variance and factor loading.
Qualitative analysis
The qualitative analysis followed the method of reflexive inductive thematic analysis by Braun and Clarke 19 using the Atlas.ti software. Thematic analysis allows the identification of commonalities in the ways in which a phenomenon is viewed by participants and allows data organisation, offering insight into patterns of meanings (themes) across datasets. 19 This method consists of six phases: (1) familiarising yourself with the data; (2) generating initial codes; (3) searching for themes; (4) reviewing potential themes; (5) defining and naming themes; and (6) producing the report. Each of these phases was carried out by two researchers who had previous experience with this method. 19
Integration
The integration step was guided by a simultaneous bidirectional framework for data-merging analytics, as suggested by Moseholm and Fetters. 20
Population, recruitment and sample
The population and the sample in this survey overlap. In fact, the population of interest to us is composed of nursing, physiotherapy and occupational therapy students in their fourth semester who experienced the first wave of the pandemic during their internships (lasting from 10 February to 17 April 2020) in southern Switzerland.
Recruitment was promoted during a plenary lecture where the study was presented to the students (14 days after the end of their internship); additionally, on the same day, an email containing the link was sent to all the students.
The choice of giving all the students the chance to participate promoted the sample’s representativeness, which was achieved by defining the population, ensuring that everyone had an equal chance to participate and recruiting an appropriate sized sample. 21 These criteria were met by descriptively testing the distribution of variables in the sample.
Sample.
Most students were in the age group 19–29 years (90.2%), followed by 30–39 (8.8%) and 40–49 (1%).
A total of 28.4% of students (N = 29) worked in a service that treated patients with COVID-19 during their last internship, specifically 28.8% (N = 19) of nursing students, 38.1% of physiotherapy students (N = 8) and 13.3% (N = 2) of occupational therapy students.
Ethical considerations
Given that no vulnerable persons were involved, the Ethics Committee of Southern Switzerland waived authorisation; however, this study was reviewed positively by the boards of directors for the bachelor’s degree courses in nursing, physiotherapy and occupational therapy at the University of Applied Sciences of Southern Switzerland. Informed consent was requested twice, before accessing the online questionnaire and before submitting the completed questionnaire. Measures were put in place to protect confidentiality and anonymity of the participants.
Findings
Ethical issues and sources for moral distress during the first wave of the COVID-19 pandemic
We asked the students which were the most often encountered moral issues during their internships. Their responses and the data analysis revealed the following: (a) appropriateness of delivered care; (b) working conditions in general with a clear reference to their own safety and that of their loved ones, the student’s status and gaps in technical knowledge.
Causes of moral distress in bachelor’s degree program.
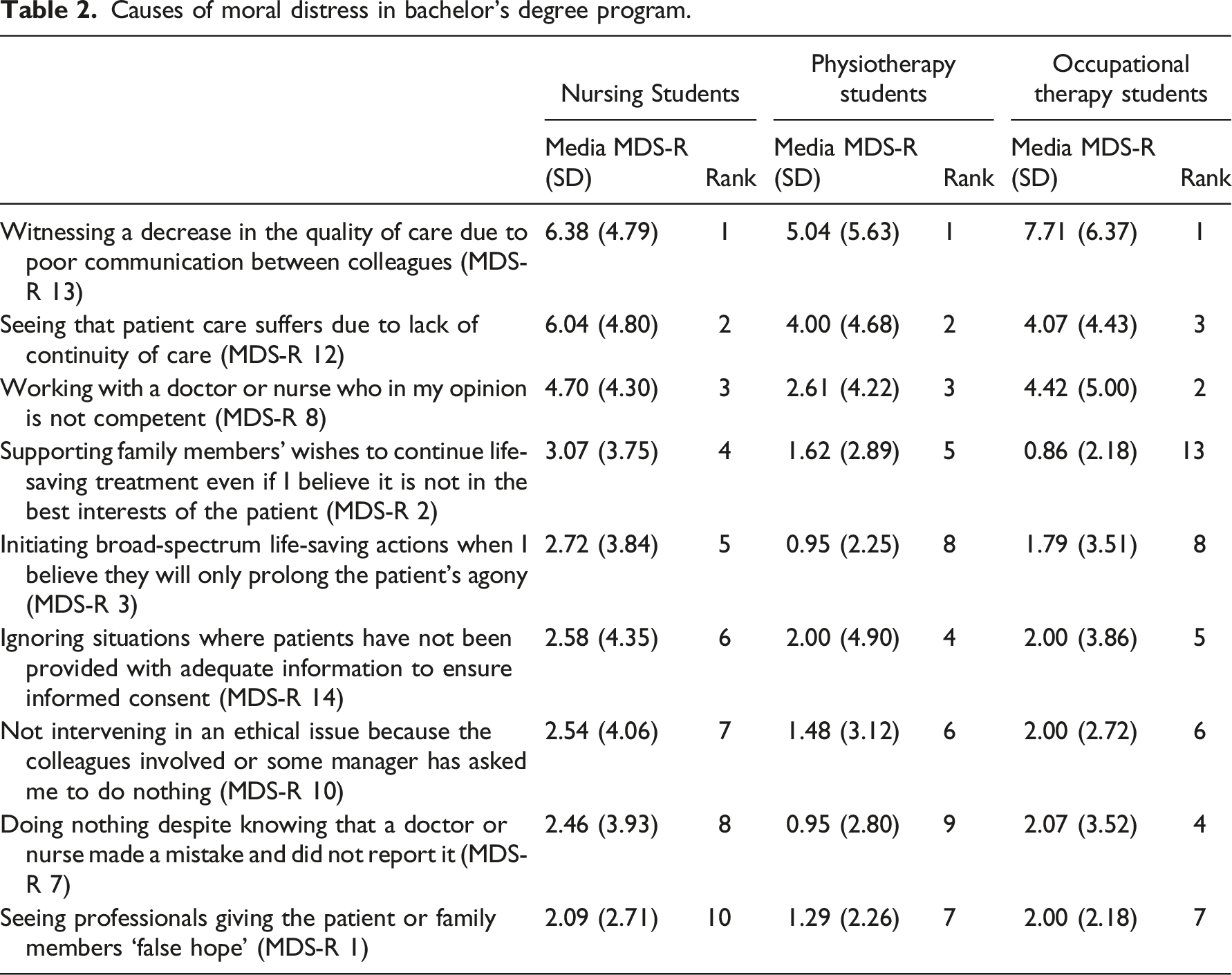
Regarding the analysis by bachelor’s degree program, the Kruskal–Wallis test, with p = 0.015, shows that the distribution of the total score of the MDS-R is not the same among the bachelor’s degree programs. Specifically, the test indicates that the two groups ‘Bachelor in physiotherapy’ and ‘Bachelor in nursing’ differ significantly (z = 2.798, p = 0.015). Attending the nursing bachelor’s degree program shows a moderate effect size with r = 0.30 22 compared to the students attending the physiotherapy bachelor’s degree course program (p < 5%).
There were no statistically significant differences in the gender-segregated analysis or for students who worked in a COVID-19 department or had not directly cared for patients with COVID-19.
According to the analysis of the I-MDS-R, witnessing a decrease in the quality of care because of poor communication among colleagues was the highest ranked item across all programs and for both genders. This finding was corroborated, and its understanding was deepened by the qualitative analysis that follows.
Appropriateness of provided care during the pandemic
Other major issues reported by students included the following: appropriateness of provided care together with the appropriateness of the information given to patients and their relatives and the degree of involvement in therapeutic decisions leading to patient isolation and loneliness.
Regarding the appropriateness of care, students reported concerns about the instructions given by physicians with respect to resuscitation or to diagnostic tests, such as swab testing, in suspected positive patients. They also reported the lack of specific medicines, the implicit rationing of intensive care beds and situations when they could not agree with the decision to continue intensive care procedures on elderly patients or patients particularly compromised from a health perspective. The central problem was taking care of DNR patients. We were told that patients over 80 years old were all to be considered DNR. This put us in very difficult situations because decisions were made for the patient without even involving him or her in the decision.
The appropriateness of care was also questioned with respect to the decision to suspend services that students considered essential, such as occupational therapy and physiotherapy. Students questioned the definition of essential and if occupational therapy or physiotherapy were nonessential. The main question was whether it was right to keep the occupational therapy clinic open and especially whether it was correct to let high-risk clients attend our clinic or if we should tell them to stay home. This was when lockdown had not yet been put in place and the risks of the virus were not yet well known.
The reorganisation of inpatient facilities and the increased hygiene measures also introduced in home care led to concerns about the quality of care provided. Access to patient rooms and other parts of the medical facilities was restricted for hygiene and security reasons. This gave some students the impression that some patients were neglected (a term used by some students) or at least not given the necessary care because of isolation; they had the impression that little effort was made to find alternatives.
Students also reported situations where due to isolation, patients were not allowed visitors even at the end of their lives. What the students reported to be at the heart of the concern was whether such an incisive and irretrievable decision was appropriate and whether there were no alternative measures to the total ban. There were discussions about allowing dying patients to have visitors and whether it was right for patients to die alone.
Working conditions in the pandemic
Students reported a concern with respect to addressing increased hygiene measures and patient isolation. A lack of knowledge about these procedures among students in the wards and services increased their sense of insecurity. In addition, some students reported situations in which isolation could not be implemented because of patients’ mental and/or cognitive condition or even because the infrastructure of the institution did not allow it.
A total of 65.7% (N = 67) of participants declared that they experienced fear and feelings of insecurity with respect to personal safety, personal protection equipment and logistics.
One of the issues that emerge with great assiduity among the results is that of one’s own safety and that of loved ones.
There was an uncertainty about the correctness of the measures put in place with respect to their own protection. For example, students reported discussions about the appropriateness of maintaining distance in the canteen when this could not be guaranteed in the ward, wearing the same surgical mask for 8 h, or even on the choice to entrust the prehospital triage to students. The discussion about protocols seems to have been quite a recurrent theme: What protection to use, how often to change devices, how close to be to the patients and what patients had to wear. We questioned the effectiveness of the orders.
Only 51% of students (N = 52) reported that ethical issues of care related to COVID-19 were discussed within the team, and within this number, only 5.8% (N = 6) reported that they were able to discuss moral issues in a dedicated time and space. The remaining students asserted that this happened mainly during breaks or in the corridors. Only 4% (N = 4) of the students had the opportunity to participate in discussions on advance directives for patients with COVID-19. We also asked students with whom (outside the work environment) they shared their moral concerns. Only 13.7% (N = 14) of the students had not discussed these issues with anyone. The students discussed these issues most often with family/friends (77.5%) and with classmates/schoolmates (61.8%). A total of 27.5% of the students spoke with other health professionals, and 14.7% of them spoke with teachers at school. Only 5.9% of the students stated that they had contacted professionals such as psychologists and counsellors, while 2% stated that they had contacted other professionals.
Discussion
The first fact worth discussing concerns the high response rate, which was 81.6%. The decision of whether to take part in a survey depends on two factors, according to Wijnen et al. 23 : personal involvement with the survey subject and personal sensitivity to the survey subject. These assumptions can be a plausible explanation for the high response rate to this survey.
The team was a place where ethical issues could be discussed, and on the other hand, unsatisfactory teamwork was the greatest source of moral distress in all three categories of students.
The fact that the team can represent both a safe place within which sensitive issues are informally addressed and a source of distress is not surprising based on the literature. 24 What definitely characterises and influences this experience is the sense of belonging. 24 For nursing students, the sense of belonging to the team during their internship is fundamental for the whole learning process. 25
If, on the one hand, the sense of belonging to the team is favourable to the well-being and learning of students, on the other hand, it can also be a source of suffering, as demonstrated in this survey, where the subscale ‘Poor teamwork’ recorded the highest value.
What the scale does not assess, but which emerged clearly in the open-ended responses as a concern, is physicians’ involvement of patients or their loved ones in the decision-making process, particularly regarding the order not to resuscitate. In 2006, Van Delden et al. 26 carried out a comparative study among six European countries with the aim of assessing how widespread DNR orders were in healthcare facilities and how this decision was made. Switzerland was included in this study. In the case of competent patients, in 17% of cases, the decision not to resuscitate was made unilaterally by the doctor without involving other people; in the case of incompetent patients, this percentage rose to 28%. Even if this study dates to 2006, it suggests that this DNR decision-making practice is not unique to the pandemic situation; however, it can be hypothesised that there was an increase in this practice during the COVID-19 outbreak. This hypothesis is partly confirmed by Fins, 27 who warns against a recrudescence of the paternalistic attitude that characterised medical practice in the past. Indeed, he traces his experience as a clinical ethicist at a large New York City hospital during the first wave of the pandemic, warning of a perceived resurgence in physicians’ unilateral decisions regarding DNR orders. Switzerland has also periodically updated its guidelines ‘Pandemic of COVID-19: Triage of intensive care medicine treatments when resources are scarce’ (vers. 3.1). 28 This document is a complement to the more general guidelines ‘Measures in intensive care medicine’. 29 In these documents, guidance is given with respect to treatment indications in intensive care medicine. Both documents focus on the patient and his or her chances of successfully benefiting from the care provided.29,30 To assess the benefits of intensive care treatment in a situation of scarce resources, the abovementioned guidelines indicate criteria and aspects that should be considered, such as the patient’s wishes, the presumed wishes of patients unable to express themselves, the involvement of the therapeutic representative, the clinical picture and the short-term survival prognosis.29,30 The patient’s wishes and therefore self-determination and the principle of autonomy are at the core of the guidelines. However, the guidelines do not prevent a physician from making an autonomous decision on the most appropriate care for the patient, especially in urgent situations. Therefore, it cannot be excluded that in some circumstances, decisions considering the age of the patients have been made. This may also be due to the closeness to Italy, where as reported by May and Aulisio, 31 when the first wave of the pandemic was at its peak, the access to intensive care was denied to patients older than 65 years and to patients with severe comorbidities.
What was reported by the students who took part in this study can be traced back to the lack of shared decision-making. This can often be a cause of discontent within the healthcare team; indeed, it has been shown that shared decision-making between all members of the healthcare team and with the patient has positive effects such as increased motivation among caregivers, a positive impact on the clinical process and better outcomes for patients. 32 However, in a context characterised by uncertainty and rapid evolution, a more widespread use of advance directives by patients could have supported healthcare professionals’ decisions about the intensity of care to provide.
Strength and limitations
The speed with which a pandemic evolves, and in particular this COVID-19 pandemic, does not allow for an overall real-time vision of the problems of students. One of the major limitations of this work is the temporal delay in producing results compared to the current situation. However, it allows us to develop prospective reflections reinforcing what has already been done and suggesting possible areas for improvement. The quality criteria for this study followed those indicated by Creswell and Clark, 33 who explicitly state that in the case of a mixed-method, the criteria are the validity (internal and external), reliability, trustworthiness and credibility.
The high response rate to the online questionnaire made it possible to collect and obtain a great wealth of data. It can therefore be concluded that the sample was very representative for the students of physiotherapy, occupational therapy and nursing curricula. Switzerland embraces the standards of the European Higher Education Area, being involved in the Bologna process; 34 thus, in some respect, these results may be representative for Europe. Nevertheless, it should be considered that the pandemic has hit countries and regions with different violence and intensity, and responses of the healthcare systems have been different among countries. The R-MDS is a validated tool for measuring moral distress among healthcare professionals, and open questions were derived from the available literature.
The reliability and credibility of the results regarding the qualitative parts were ensured through meticulous description of the analysis process and inclusion of extracts of responses that corroborated the results. In addition, the responses were coded by two researchers, and their results were compared. Disagreements between the researchers on the coding or definition of the themes were approached by discussing and analysing the procedure and the reasons for disagreement until the two researchers reached a consensus supported by the data. For the quantitative analysis, a similar process was put in place for the statistical analysis, which was cross-referenced by two researchers.
Recommendations
First, we recommend including health profession curricula content about infectious diseases, prevention of communicable diseases and personal protection as well as elements of clinical epidemiology. This intervention aims to better prepare students to deal with potentially infectious patients. This recommendation is widely supported in the literature.35–39 Studies show that good preparation of students makes them more likely to agree to serve in the event of a pandemic and helps them face the challenge with a greater confidence and peace of mind.35–39
For the relief of moral distress, debriefings have been suggested to be promising.9,40 Debriefings can be carried out in a variety of forms, ranging from a meeting as a group or one on one 40 or setting up a dedicated hotline 41 to writing a diary that will then serve as a basis for meetings. 42 This heterogeneity among forms of debriefings was highlighted by Morley and Shashidhara 43 who discussed the lack of academic literature in this regard. The fact that there is a lack of consistent literature on measures aiming at reducing moral distress also emerged in the literature review by Imbulana and Davis, 44 who invited the scientific community to carry out larger randomised controlled trials to evaluate multifaceted interventions. However, as pointed out by Morley and Horsburgh 45 carrying out research, especially on the efficacy of debriefings, presents several methodological issues and potential sources of bias. Nevertheless, based on their experience, structured debriefings carried out by clinical ethicists are appreciated and provide positive benefits to participants.
As long as the situation is unresolved from an epidemiological point of view, it will be necessary to provide extra preparation for students who are engaged in clinical internships. Not only theoretical knowledge but also practical knowledge, such as dressing and proper use of personal protective equipment 39 and hand hygiene, 46 should be integrated and reinforced during training.
Conclusions
This survey offers a faithful perspective on the experience of physiotherapy, nursing and occupational therapy students involved in the first pandemic wave. Students found themselves carrying out their second internship in a delicate, unforeseen situation, and no one would have imagined that it could evolve so abruptly.
This study aimed to understand what ethical issues were of most concern to students and whether these were shared and with whom. Furthermore, this study aimed to measure the level of moral distress by gender, course of study and direct contact with patients with COVID-19. However, this study had no ambition to explain the whole experience of students during their internship, and in some respect, its results indicate difficulty in providing a clear dichotomy between psychological experienced distress and moral distress. Nevertheless, the study results deserve some consideration.
This research revealed the importance and ambivalence of the team, which, on the one hand, is support for discussing ethical issues related to COVID-19 during practical training, but, on the other hand, it represents the main source of moral distress in students across programs. With regard to moral distress, a higher relative risk was found among students in the Bachelor of Nursing program than other courses. In contrast, there were no statistically significant differences in the gender-segregated analysis or for students who worked in a COVID-19 ward or service or who had not directly cared for patients with COVID-19.
We recommend that future research should study a larger population representing all health care professionals, evaluate the effectiveness of recommendations implemented and aim to understand the reasons behind the higher levels of moral distress found among male and female students in the nursing program compared to other courses of study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by the University of Applied Sciences of Southern Switzerland, Department of Business Economics, Health and Social Care.