
Abstract
Background
Moral distress is a well-recognized term for emotional, cognitive, and physical reactions of professionals, when facing conflicts between perceived obligations and institutional constraints. Though studied across medical roles, limited research exists among physiotherapists.
Research Question
What factors contribute to Moral distress among physiotherapists and how do they cope?
Objectives
To develop and test a multifaceted model of Moral distress and gain an in-depth understanding of the phenomena.
Research Design
A 2017–2022 mixed-methods study: (1) Survey of 407 physiotherapists quantitatively testing a literature-based model analyzing relationships between Moral distress, Moral sensitivity, Locus of control, Self-efficacy, Ethical climate perceptions and demographics, analyzed by descriptive and inferential statistics, multiple comparisons and structural equation modelling (SPSS26, SAS, AMOS); (2) Semi-structured interviews with 21 physiotherapists examining Moral distress experiences using meticulous phenomenological analysis.
Participants and Context
Israeli physiotherapists from various occupational settings recruited via professional networks.
Ethical Considerations
The Haifa University Ethics Committee authorized the study. Informed consent was obtained for the anonymous survey and before interviews regarding recording, and quote use.
Findings
Quantitative results showed moderately high average Moral distress, significantly higher among women and paediatric physiotherapists, positively correlating with Moral sensitivity. Qualitative findings revealed intense emotions around Moral distress experiences, inner conflicts between care ideals and constraints, and coping strategies like reflective skills. Senior therapists, despite higher self-efficacy and moral sensitivity, still reported persistent high distress.
Discussion
Moral distress has complex links with moral sensitivity, self-efficacy, perceived professional autonomy and organizational support. A renewed framework emerged explaining relations between moral distress and personal, professional and organizational factors.
Conclusions
Multidimensional insights help identify Moral distress causes and coping strategies among physiotherapists, advancing theory. Conclusions can shape ethics training programs and competencies.
Introduction
Moral Distress is a phenomenon associated with ethically complex situations 1 , p. 6. 40 years of research yielded new definitions, including: “One or more negative self-directed emotions or attitudes that arise in response to one’s perceived involvement in a situation that one perceives to be morally undesirable” 2 , p. 67. Research revealed Moral distress is a physical, emotional, and cognitive phenomenon,3,4 which over time accumulates and intensifies. 5 Moral distress can lead to disengagement, compassion fatigue, decreased quality of care, and burnout.6–8 Alongside negative effects, there are positive aspects to this phenomenon, serving as a valuable catalyst for moral progress by implementing ethical and moral reasoning into daily clinical decision-making, 9 and thus contributing to moral maturation and ethical competence. 10
Moral distress remains an underexplored phenomenon in physiotherapy compared to other health professions like nursing,11–15 despite increasing recognition of its impacts on provider wellbeing and quality of care.8,16–19 Available data indicates physiotherapists experience issues like compassion fatigue, burnout, and poorer care attributed to unresolved Moral distress. 8 As hands-on providers integral to patient recovery, understanding, and addressing Moral distress is critical for physiotherapists to optimize practice and outcomes.
Yet few studies have thoroughly investigated Moral distress within this population. A research gap persists around the drivers and mediating factors of Moral distress among physiotherapists across personal, professional, and organizational realms. Examining discipline-specific influences on distress manifestation can tailor interventions to support clinicians’ ethical practice and resilience. This study helps address a need for population-specific inquiry by surveying Israeli physiotherapists regarding moral behaviors and environments, then qualitatively probing on barriers and supports regarding distress.
Given physiotherapists’ central patient care role and risk for adverse outcomes from Moral distress, discipline-specific study is critical. By examining drivers and mitigating factors of Moral distress in physiotherapist across personal, professional, and organizational domains, this study provides an opportunity to inform tailored interventions and coping skills within this population. Ultimately, the goal is to promote ethical practice and clinician well-being through evidence-based supports matching the needs of this group.
Method
Several factors have been found relevant to the understanding of Moral distress: “Self-efficacy,”
20
“Moral sensitivity,”21,22 “Locus of Control,”
28
[] and “Perceived organization ethical climate.”
23
Few Studies have empirically tested multi-variate models,
24
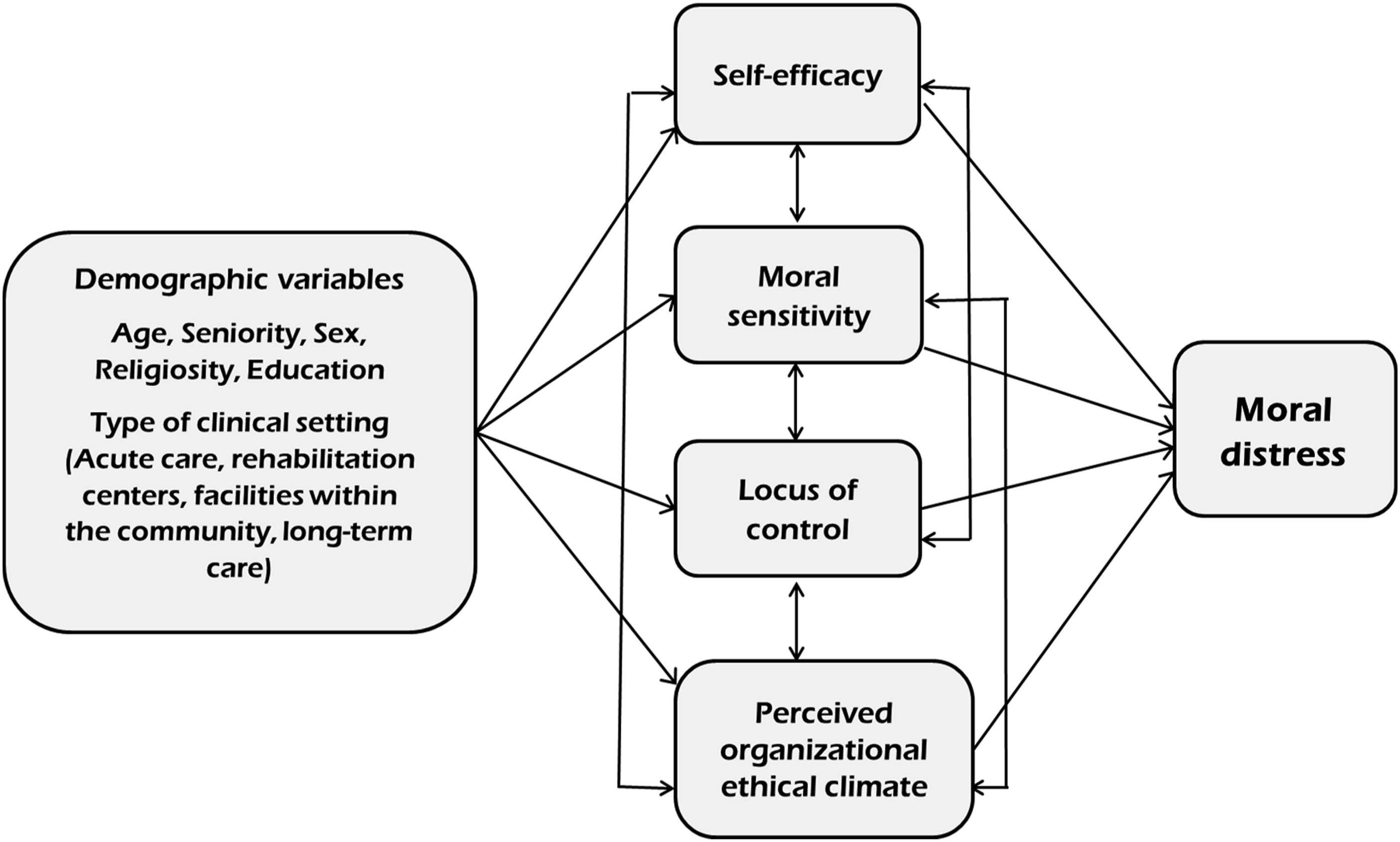
but none have included these factors in a comprehensive model. These four variables were selected for inclusion given evidence from prior literature pointing to their potential explanatory power regarding Moral distress. The corresponding instruments chosen to measure them have established validity and relevance for healthcare professionals. Together, these four variables—representing personal, interpersonal and systemic factors—construct an integrated conceptual framework for studying Moral distress. (Figure 1): (1) (2) (3) (4) Conceptual Model of moral distress.
In this article, we will first describe the quantitative phase of the research (method and results), followed by the qualitative phase. The discussion section will provide an integrative interpretation of key findings from both phases with references to relevant literature.
Phase 1: Quantitative
After obtaining ethical approval from the Haifa University Ethics committee, a purposive and snowball sampling within professional networks was used, recruiting practicing physiotherapists via email and social media to participate in an online survey. Inclusion criteria entailed being a currently certified, practicing physiotherapist in Israel. Students were excluded from the study. Based on published guidelines,
31
we disseminated a web-based survey. Four-hundred and seven Israeli physiotherapists (68% response rate) provided consent (online required answer) and completed questionnaires addressing the models’ variables: (1) (2) (3) (4) (5)
Data was analyzed using SPSS26 for descriptive statistics, SAS for analysis of variance and linear regression, and AMOS for structural expression modeling (SEM).
Quantitative results
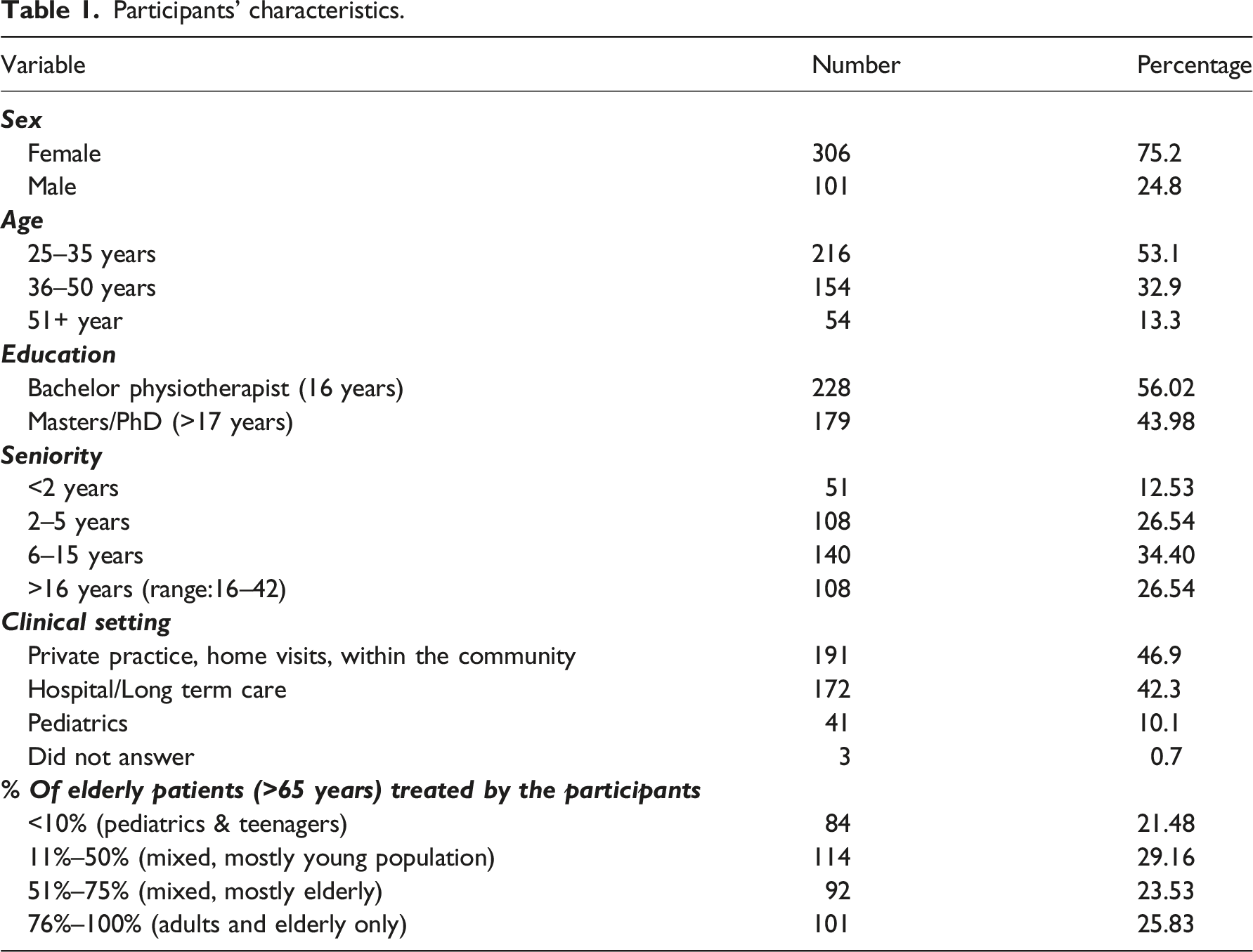
Participants’ characteristics.
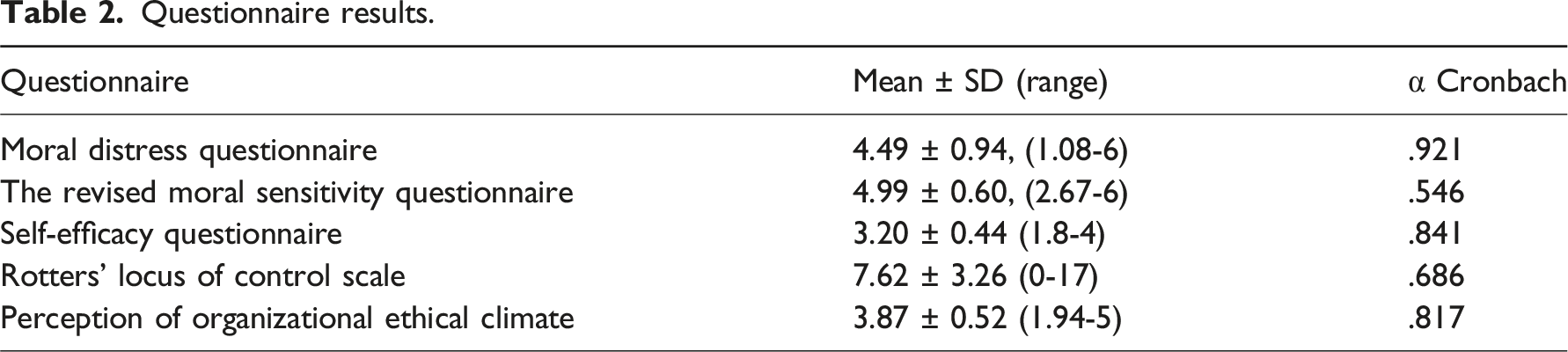
Questionnaire results.
Sample size was determined based on the common “rule of thumb”—at least 20 observations per independent variable. With 13 explanatory variables examined in the conceptual model, the minimum required sample was 260 participants. More complex formal sample size calculation methods were considered but could not be implemented reliably given a lack of prior variance estimates from similar studies. Therefore, the simple “rule of thumb” was deemed most appropriate. The final sample obtained was 407 Israeli physiotherapists, exceeding the minimum threshold and providing adequate statistical power for the planned analyses.
Average Moral distress levels were moderately high (mean 4.49 on a 1-6 scale) in the overall sample. Moral distress levels were significantly higher among women (mean 0.37 points higher than men) and physiotherapists treating children (compared to those treating mostly adults). A weak positive yet significant correlation (r = 0.224, p < 0.001) was found between Moral sensitivity and Moral distress—as Moral sensitivity levels increased (mean 4.99 on a 1–6 scale), Moral distress levels also rose. Self-efficacy (mean 3.20 on a 1–4 scale) positively correlated with Moral sensitivity (r = 0.356, p < 0.001) but was not directly linked to Moral distress. Longer seniority was weakly related to higher self-efficacy (r = 0.190, p < 0.01) and Moral sensitivity (r = 0.248, p < 0.01), however, senior therapists still reported high Moral distress. Several factors together explained 8% of the variance in Moral distress scores, pointing to the complexity of influences on this phenomenon. MANOVA (Hotellings’ trace) highlighted significant differences between age groups [F (12,784) = 3.615, p < 0.001], particularly in their perception of professional autonomy, a factor within PEC [F (2,395) = 4.735, p = 0.009]. Physiotherapists aged 23–35 reported more professional autonomy than those aged 51+. Younger physiotherapists (23–35) have significant lower scores of Moral sensitivity than older physiotherapists (51+), [F2,395) = 10.122, p < 0.001].
A significant MANOVA model [F (18,1172) = 3.127, p < 0.001] revealed that senior physiotherapists (16+ years of practice) perceive themselves as highly competent professionally (Self-efficacy), highly morally sensitive, yet bounded by low professional autonomy. As for Moral distress, a significant main effect was found [F (2,395) = 4.331, p < 0.05], with higher levels of Moral distress among physiotherapists who treat children, as opposed to those who treat mostly adults.
Regression analysis revealed that the only predictive demographic variable for Moral distress was sex (β = −0.170, p = 0.001), indicating that women are somewhat more susceptible to Moral distress than men (explaining only 3%). Moral sensitivity and Self-efficacy were also found to be predictive variables of Moral distress [β = 0.253, p < 0.001; β = −0.108, p = 0.015, respectively], explaining only 8% of the variance, pointing to the complexity of the phenomenon.
Path analysis (Figure 2) via structural equation modeling (SEM) showed satisfying indices of fit: χ2 = 85.17, p < 0.01, CFI = 0.95, NFI = 0.94, RMSEA = 0.077. Yet the analysis yielded only a partial explanation of Moral distress: Self-efficacy and Moral sensitivity were found to be correlated with seniority and Moral distress—as seniority rises Self-efficacy is higher, and Moral distress is diminished. At the same time, as seniority rises Moral sensitivity and Moral distress are higher. This contradiction left many unanswered questions. Furthermore, the literature stresses the connection between Moral distress and PEC, although our data did not. The conceptual model–path analysis.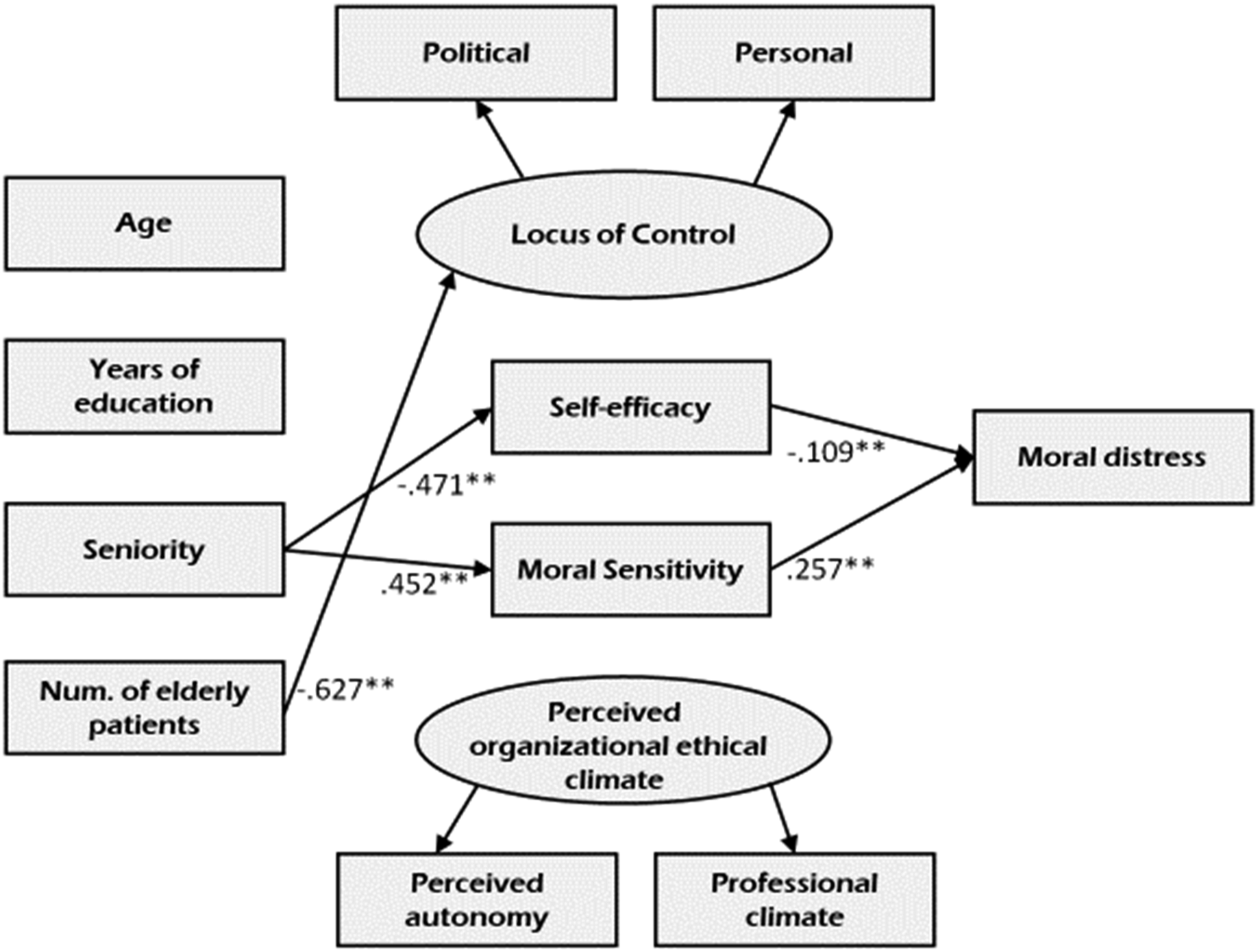
Considering these findings, we asked: Why do physiotherapists from the field of pediatrics report higher levels of Moral distress than others? Which factors might explain the gap between novice and senior physiotherapists in their perception of professional autonomy? What is the role of PEC in the occurrence of Moral distress? These questions and more were addressed in the qualitative phase of the study.
Phase 2: Qualitative
Among online survey respondents who gave their online written consent to be interviewed and left their personal contact information, we reached out to physiotherapists from different fields of practice, women and men, secular and religious, from different regions of the country, who treat patients across various age groups. The goal was to achieve maximum possible diversity. 35
An interview guide was constructed based on the results of the quantitative phase. Twenty-one semi-structured in-person interviews were conducted, lasting 60–90 min each. Interviews took place in a quiet and discreet location, according to the choice of the interviewees (in their homes or workplace). All interviews were audio-recorded, transcribed verbatim, and analyzed using thematic analysis through multiple stages of coding to identify key themes and subthemes. Analysis began early in parallel to interviews to check for saturation. Several steps were taken to ensure credibility and trustworthiness: the interview guide was carefully developed based on the quantitative results; maximum variation sampling of participants; awareness of researcher biases; dual analysis with research supervisors; maintaining an audit trail through data analysis stages. Key aspects supporting quality and rigor include the fit of semi-structured interviews for the research aims, transparent processes for sampling, data collection and analysis, and presentation of an evidence-based “thick description” so readers can judge credibility. Content and thematic analysis, with special attention to empirical coding and examination of commonalities and differences, exposed themes with relations to the conceptual framework. 35 New themes, concepts, and definitions were discovered which led to the elaboration of the model.
Qualitative results
Interviewees (Table 3) were eager to talk about experiences they have never shared before. This was an unexpected, meaningful result by itself. Interviews were emotional in content and expressive in gestures, such as passionately speaking, crying, whispering, sharing what was described as “private secrets,” and more. For example: Usually I repress… just now, talking to you, I realize that. It was hidden all this time. I guess it’s been burdensome … I’m sure I have more examples (of Moral distress), but I repress these experiences, I don’t talk about them, not even with myself. (I) Interviewees’ characteristics.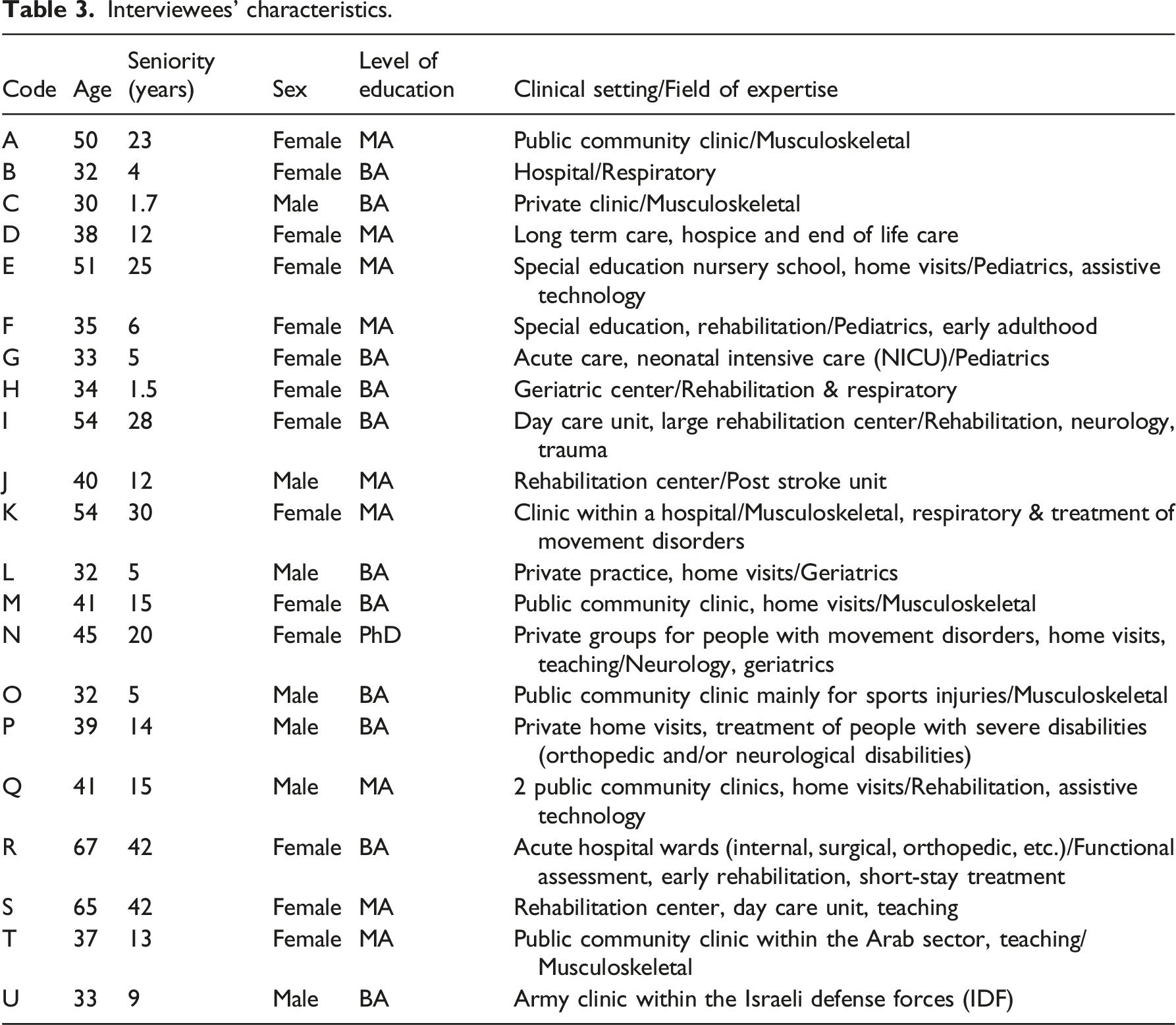
All reported they had encountered ethical dilemmas, and all had multiple examples of experiencing Moral distress, giving insight into a range of issues evoking it. Moral distress and futility was a rich subtheme, exposing the inner conflict between a rehabilitative professional identity and the understanding that compassionate, prolonged non-rehabilitative care is also needed:
Today I feel proud […] before I say I’m a physiotherapist, I say “I work in a geriatric long-term care facility.” But some days I feel my presence is useless, my work is futile, they suffer anyway, they die, so why bother? Those are days of severe moral distress. (D)
Sub-theme
You know, working in rehab centers, I was frequently asked – “Will I walk again?”, “Will my hand regain function?” and I used to lie, not really lie, but avoid the truth, saying “I don’t know,” “we’ll see” … Those were morally distressing moments. (N)
Sub-theme
We are unable to perform everything we learned due to lack of time and manpower. Sure, one learns to prioritize. But sometimes you really need those extra 5 minutes with a patient, to let him feel you are attentive, not thinking about the next patient and your busy schedule. It’s a terrible conflict! You see many patients, but it’s superficial. You end your day feeling you did your very best, but it still wasn’t beneficial
Other sources of Moral distress were
Participants who considered themselves highly sensitive to moral issues described frequent encounters with Moral distress. Senior interviewees felt less autonomous in their practice, with highly perceived Self-efficacy, yet burdened by Moral distress, compassion fatigue, noting lack of organizational support. On the other hand, physiotherapists who felt that their opinions were heard and considered by their superiors articulated internal LOC, better PEC and a clear view of their responsibilities when encountering dilemmas. The analysis highlighted that physiotherapists with high Self-efficacy incorporate efficient coping strategies when dealing with morally distressing situations and revealed the intensity of the struggle with Moral distress for those with low Self-efficacy.
Physiotherapists treating children of all ages particularly expressed persistent high Moral distress, regardless of seniority or any personal changes: “Just like the joy of seeing a toddler walk for the first time doesn’t fade, moral distress doesn’t change over time, maybe even intensifies. You just can’t get used to it.” (E).
With regards to
We need someone from the field of ethics to guide small group discussions, in a compassionate atmosphere, without personal ramifications. To allow therapists to share difficulties without judgment. To practice moral deliberation. It must be done. We need to dedicate time for conversations like this one. (D)
Triangulation led to better understanding of our prior assumptions (models’ components): Physiotherapists are highly aware of their patients’ needs, familiar with professional protocols and organizational policies. Self-efficacy rises with seniority, yet experience has a negative impact on their perception of professional autonomy. Physiotherapists show high levels of Moral distress, yet their experiences are rarely spoken of, coping tools do not include ethical knowledge, gradually weakening their ethical competence.
Discussion
Integration of quantitative and qualitative results identified areas of convergence, overlap and divergence between phases. For example, Convergence—The qualitative data supported and provided insights into the key quantitative finding that Moral distress levels are significantly higher for pediatric physiotherapists. Interviews revealed the complexity and amplification of distress treating children due to emotional responses and personal identity as mothers; Overlap—For loci like Moral sensitivity, Self-efficacy, and autonomy, qualitative data helped explain statistical relationships with Moral distress. Discussions of sensitivity as essential “moral compass” clarified the moral distress connection. Accounts of mediating roles of Self-efficacy and autonomy provided nuance around quantitative correlation strengths; Divergence—Lack of statistical relationships for factors like LOC and ethical climate contrasted with interview examples showing connections tied to control and autonomy. Our data highlighted that physiotherapists experience Moral distress levels ranging from moderate to high. This appears comparable to intensities reported among physicians, versus typically higher distress found in nursing populations.19,26,27 Perceived professional autonomy inherent to the role may buffer distress intensity relative to other provider groups.
The lack of clear conceptualization of Moral distress influences research, ethics education, and organizational policy development. 36 In our study, we deliberately avoided defining Moral distress, allowing participants to express their understandings, and explain Moral distress in their own words. Our qualitative results shed light on Campbell, Ulrich and Grady’s 2 definition of Moral distress (as quoted in the Introduction). We found that “negative self-directed emotions” refers to shame, concealed emotions, and repression; “perceived involvement” was described in our cohort as what physiotherapists think they ought to do in ethically challenging situations, while acknowledging professional borders, organizational expectations, and their ability to act as moral agents. They attribute high value to their profession and capabilities and to the collective goal to achieve beneficence, yet they stand alone when coping with ethical problems. Their obligations towards patients, colleagues, and employers enhance their Moral distress. We realized that Moral distress gradually evolves from a progressing dissonance between personal understanding of morality, perceived ability to act morally, non-optimal organizational support, and the expression of these factors in routine daily practice.
As opposed to the widely established empirical connections between Moral distress and PEC among nurses, 23 our results question the accuracy and adaptability of questionnaires across healthcare disciplines. While statistical relationships were not established, interview data provide compelling examples of how reduced organizational autonomy amplifies moral distress. This highlights the key role of perceived autonomy in shaping the ethical climate. The discrepancy between weak statistical interconnections and rich qualitative data suggests that specific, sectorial, tailor-made data collection tools are needed.37,38 Our results highlight that in pediatric settings, physiotherapists are exposed to higher Moral distress than those treating other age groups, emphasizing the need for another layer of specificity. Similarly, although locus of control did not statistically link with Moral distress, interviews reveal a connection where internal locus aligns with greater distress. Participants describe fluctuations in internal/external control perceptions over time and situations, challenging locus of control as a fixed trait.
Previous researchers have argued over the question—should we strive to minimize Moral distress, or should we accentuate the positive sides of this phenomenon?5,10 Our data shows that Moral distress is an integral component of humane care, linked to compassion and moral contemplation [“If I had less distress, I wouldn’t be a good therapist” (U)]. Yet physiotherapists are in definite need for coping methods. Accumulating experiences of unresolved Moral distress can erode resilience. 9 It seems that empowering the individual, linking between Moral sensitivity, internal LOC, and sense of accountability might not diminish the experience of Moral distress, but could provide solid ground for developing coping strategies. Analysis of the qualitative data interestingly led to the understanding that there is a great need for developing and nurturing reflective abilities as an indicator for coping with Moral distress. The complex dissonance of low confidence when facing ethical challenges—mostly due to lack of ethical knowledge and scarce opportunities for moral deliberation—may undermine one’s professional identity, motivation, and diligence. Based on the work by Donald Schon (1983) who coined the term “reflective practitioner,” we highlight the need to integrate reflective processes with practical-ethics knowledge. Intervention plans should teach how to shift from “Technical rationality to Reflection-in-Action,” 39 p. 50. So far, little has been empirically studied and clinically assimilated among physiotherapists.
This study makes several contributions to furthering understanding of Moral distress, including providing empirical evidence to support recent theoretical definitions from the literature. The findings reveal Moral distress arises from negative self-directed emotions tied to perceived involvement in morally troubling situations, aligning with current conceptualizations. Additionally, the data point to positive aspects of Moral distress as potentially catalyzing moral growth and professional identity formation. Such multidimensional insights led to proposing an expanded conceptual framework (Figure 3). The integrated explanatory model offers a new framework incorporating significant influencing factors from quantitative results and qualitative insights. Practical recommendations center on developing ethical competence and distress coping capacities among physiotherapists, based on three clusters: personal, professional, and organizational. Each cluster contains variables empirically found in this study to be connected to Moral distress, and new variables—qualitatively identified. Further research is needed to empirically test this model, aiming to achieve the following: (a) a better understanding of factors that increase or decrease Moral distress; (b) a clear definition of the barriers for effective coping with Moral distress; (c) a list of components needed to create positive ethical climate in different work settings, promoting and supporting ethical deliberation. For these to be accomplished, we emphasize the need for further development of specific quantifying tools for Moral distress and interconnected factors, alongside in-depth inquiry of this multi-layered phenomenon. New conceptual model.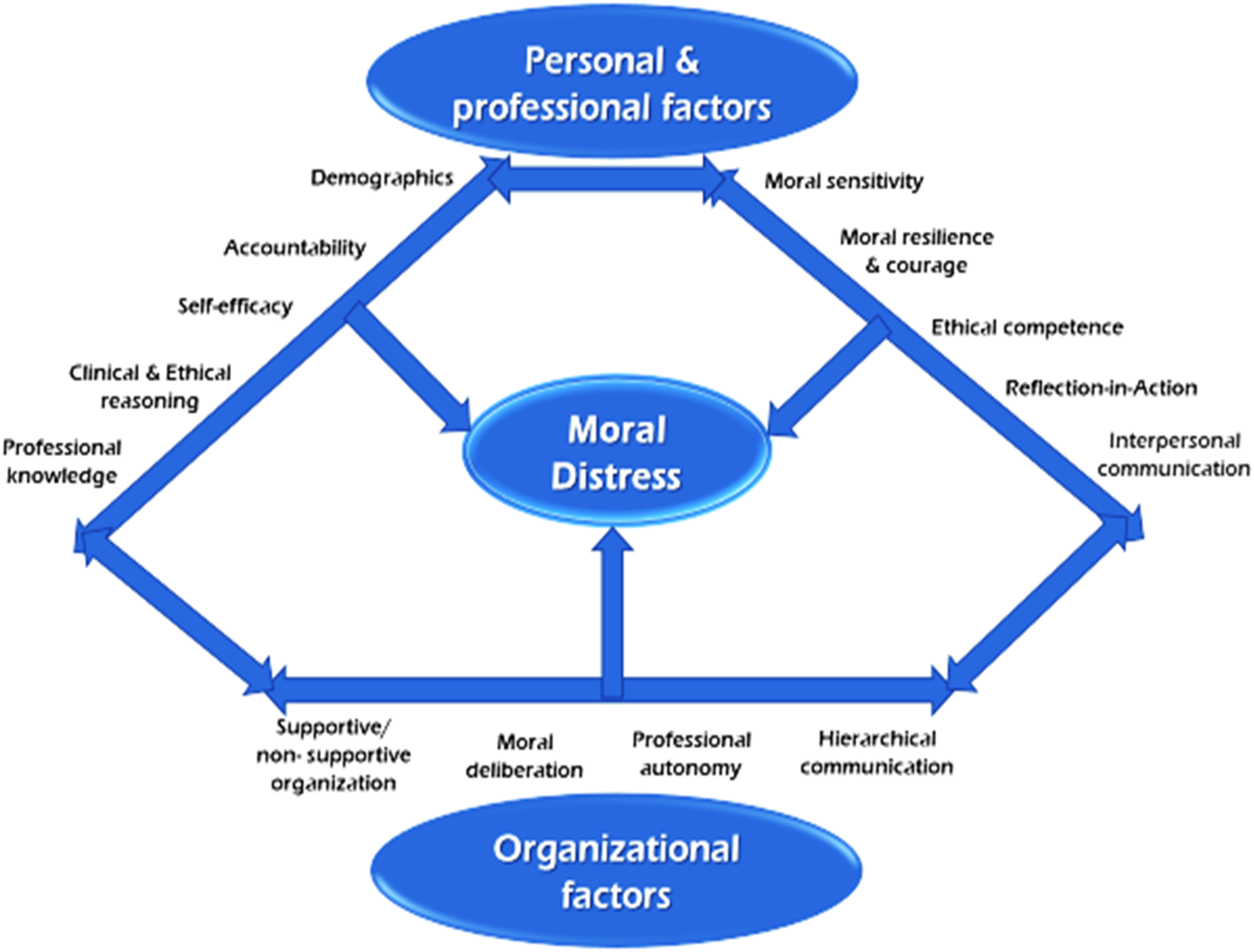
Conclusions
Moral distress is an intriguing phenomenon. Physiotherapists, scarcely studied, show moderate to high levels of Moral distress in different work settings, significantly in the field of pediatrics. Coping efficiently with Moral distress derives from personal, professional, and organizational factors, thus, intervention plans should address all three components. Healthcare organizations should strive to create working environments where one can express professional competence and act as a moral agent.
We suggest implementing training programs for ethical counselors. Alongside professional roles and responsibilities, they will provide ethical guidance to their colleagues, identify morally distressing situations, initiate moral deliberation, allow personal consults, and form trans-professional collaboration. We suggest that the ethical committee of each profession educate, qualify, and accompany those who undertake the role of ethical counselors, helping them to raise awareness, disseminate up-to-date knowledge, take an active part in the establishment of professional ethical standards, and collaborate in research projects.
Ethical considerations
The Haifa University Ethics Committee authorized the study. Participants received written information about the study purpose, confidentiality commitments and researcher details. Informed consent was obtained for each research phase: As an obligatory question in the web-based survey, and before interviews regarding recording, privacy and anonymous quote use. Identifying details were coded and protected during third-party transcriptions.
Limitations
Survey participants and interviewees took interest in this study of ethics, which could create a bias. A possible influence of the researchers’ internal point of view led to the following steps: precise coding definitions and clear coding procedures were shared with two external research experts, allowing a thorough check of the researchers’ interpretations against raw data; data sets and descriptions were rich enough so that peer debriefing could help judge the findings’ credibility.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.