
Abstract
Healthcare providers caring for people living with dementia may experience moral distress when faced with ethically challenging situations, such as the inability to provide care that is consistent with their values. The COVID-19 pandemic produced conditions in long-term care homes (hereafter referred to as ‘care homes’) that could potentially contribute to moral distress. We conducted an online survey to examine changes in moral distress during the pandemic, its contributing factors and correlates, and its impact on the well-being of care home staff. Survey participants (n = 227) working in care homes across Ontario, Canada were recruited through provincial care home organizations. Using a Bayesian approach, we examined the association between moral distress and staff demographics and roles, and characteristics of the long-term care home. We performed a qualitative analysis of the survey’s free-text responses. More than 80% of care home healthcare providers working with people with dementia reported an increase in moral distress since the start of the pandemic. There was no difference in the severity of distress by age, sex, role, or years of experience. The most common factors associated with moral distress were lack of activities and family visits, insufficient staffing and high turnover, and having to follow policies and procedures that were perceived to harm residents with dementia. At least two-thirds of respondents reported feelings of physical exhaustion, sadness/anxiety, frustration, powerlessness, and guilt due to the moral distress experienced during the pandemic. Respondents working in not-for-profit or municipal homes reported less sadness/anxiety and feelings of not wanting to go to work than those in for-profit homes. Front-line staff were more likely to report not wanting to work than those in management or administrative positions. Overall, we found that increases in moral distress during the pandemic negatively affected the well-being of healthcare providers in care homes, with preliminary evidence suggesting that individual and systemic factors may intensify the negative effect.
Introduction
Moral distress refers to the emotional state experienced by healthcare providers who face a moral dilemma and are subsequently constrained from pursuing an action in keeping with their values (Campbell et al., 2016; Fourie, 2017; Jameton, 1984). Moral distress includes the emotional reactions that arise when one’s values are challenged or when one experiences injustice or the suffering of others: these have been termed ‘moral emotions’ (Haidt, 2003). The COVID-19 pandemic has created many morally stressful situations, evoking a range of moral emotions in healthcare providers such as anger and guilt, and high levels of moral distress (Riedel et al., 2022).
Moral distress is highly prevalent among people working in long-term care homes (hereafter referred to as ‘care homes’). In a pre-pandemic study, as many as 75% of nursing staff in a care home described experiencing moral distress at some point over the previous year (Pijl-Zieber et al., 2018). Healthcare providers working within the long-term care home environment have also been shown to experience higher levels of distress than their peers in acute care settings (De Veer et al., 2013). Many factors contribute to these high levels of moral distress in long-term care, including power hierarchies, lack of staff autonomy, staff restrictions within a task-oriented environment, concerns about liability, and relationships with family members of the residents (Greason, 2020). The care needs of residents in these settings have become increasingly complex over time (Ng et al., 2020). Residents are of advanced age (with an average of 85 years) and have a high prevalence of dementia, frailty, and multimorbidity (Ontario Long Term Care Association, 2019). Secondary to institutional constraints, workload demands, or conflicting expectations with families, staff may not feel that they can personalize care requirements in accordance with a resident’s wishes or provide the quality of care that they believe to be necessary for that resident. Studies have found that the care home environment is chronically understaffed, which in turn affects a provider’s ability to demonstrate flexibility in scheduling of care to allow the additional time for self-management of care, or provide high-quality person-centred care (Badone, 2021; Carolino, 2021). Within an environment that emphasizes completing tasks related to basic physical care, staff also report distress over the lack of time to adequately meet the emotional needs of residents (Greason, 2020; Pijl-Zieber et al., 2018). Overall, providers working in care homes frequently find themselves in situations where they cannot act in a manner that aligns with their beliefs or their professional or personal core values, giving rise to moral distress.
The COVID-19 pandemic added substantially to the risk of moral distress for healthcare providers of residents living with dementia (Long-Term Care Staffing Study Advisory Group, 2020). Long-term care homes were disproportionally impacted by the pandemic, with residents accounting for more than 80% of all reported COVID-19 deaths in Canada during the first wave (Clarke, 2020). Infection control measures were required for resident safety, including isolating residents within their rooms and suspending recreational and social activities. Many homes reported critical staffing shortages, leading to insufficient staffing levels to help residents with the basic activities of daily living (Office of the Auditor General of Ontario, 2021). Some jurisdictions instituted a ‘single-site’ order that restricted staff to work in only one home, which resulted in an insufficient number of experienced staff to provide an adequate level of care (Office of the Auditor General of Ontario, 2021). The staffing changes and other pandemic rules and restrictions resulted in dramatic reductions in staff autonomy and placed significant constraints upon the actions they could take to maintain their integrity when faced with situations that challenged the congruity between their values and actions, giving rise to moral distress.
There is limited research to date that documents the experience of moral distress amongst healthcare providers caring for people with dementia in care homes during the pandemic, with most studies focussing on end-of-life care (Bolt et al., 2021). While there have been studies on long-term care home staff burnout (Costello et al., 2019; White et al., 2021) these have not addressed moral distress as a specific contributor to burnout. For example, Martín et al. (2021) found that staff working in care homes through the pandemic experienced increased rates of depression, anxiety, and overall decreased quality of life. Our study aims to address the gap in knowledge by examining moral distress in long-term care homes during the pandemic, with the following specific objectives to 1) describe the prevalence of and change in moral distress and associated effects on staff well-being; and 2) examine factors associated with moral distress within the care home environment during the pandemic.
Methods
Study design
We chose an online cross-sectional survey method that ensured respondent anonymity and facilitated accessibility and participation. The survey was programmed and hosted online by the Survey Research Centre at the University of Waterloo. The study was reviewed by the University Health Network Research Ethics Board (REB#20–5866), and the University of Waterloo Research Ethics Committee (ORE#42803).
Recruitment and consent
Within Ontario, care homes are residential long-stay facilities licensed and funded by the Ministry of Long-Term Care, providing care for people who require 24/7 nursing and personal care support. These facilities are home to older adult residents with complex medical needs, having the highest prevalence of dementia and other select chronic health conditions (Ontario Long Term Care Association, 2019). In Ontario, more than 70% of residents have a formal diagnosis of dementia, with 90% having a cognitive impairment (including individuals with stroke or brain injury who may not receive a diagnosis of dementia) (Canadian Institute for Health Information, 2018). Healthcare provider participants were recruited by distribution of an open survey link through several partner organizations. This allowed us to include a wide variety of care home settings, regional populations (rural to small <30,000, medium 30,000–100,000, or urban >100,000), range of home sizes (fewer than 100 beds, 100–199 beds, over 200 beds), and ownership status (for-profit, non-for-profit, and municipally run homes). Participants included healthcare providers such as nursing staff (including personal support workers), recreational therapists, physicians, and managers and administrators.
Distribution of the survey link took place through the partner organizations' online newsletters, electronic mailing lists, websites, and social media. Participant inclusion criteria included: working in a care home in Ontario during the first wave of the COVID-19 pandemic (either at the front-line or in a management/administrative role); fluency in English, and not currently working for the University Health Network. Survey participants reviewed an online consent form and then provided informed consent by indicating they had reviewed the information and agreed to participate by clicking a button that directed them to the survey.
Survey instrument
The survey collected demographic information about the respondents, the care home where they worked, and their experiences during the pandemic from March 1, 2020. The research team developed the survey in consultation with stakeholders and study partner organizations, and piloted it with five care home staff. After this pilot, we made minor edits to language used (e.g., adjusting terminology to match terms commonly used), improved the clarity of a few questions, and adjusted the formatting of the survey to improve flow.
We adapted the Moral Distress in Dementia Care Instrument (Awosoga et al., 2018) to develop questions about moral distress experienced during the pandemic (Supplementary Material). The instructions provided to respondents were: The following questions are about ‘moral distress'. Moral distress is the bad feelings a healthcare provider gets when they know the right thing to do for a resident but, for some reason, is unable to do it. In these questions, you will be asked about your level of distress, if any, resulting from different situations related to the COVID-19 pandemic
Sample size
Statistical software was used to calculate power - specifically, G*Power (Faul et al., 2007). We determined that a final sample size of 185 would achieve 80% power, and a sample of 213 would achieve 90% power to detect medium effect sizes in Bayesian proportional odds models examining the relationship between respondent or care home characteristics and severity of moral distress (Cohen’s W of 0.30; α=0.05). Cohen’s W measures effect size of associations among categorical variables, where 0.30 corresponds to a medium effect size. The target sample size was set at 300 to accommodate exclusions and incomplete surveys.
Analysis
Bayesian inference was chosen for the accuracy of this analysis given the multiple comparisons and to allow probabilistic interpretation (Bidhendi Yarandi et al., 2020). The interpretation of the Bayesian 95% credible interval (CrI) is that there is a 95% probability that the true (unknown) estimate would lie within the interval, given the evidence provided by the observed data.
The survey results were summarized descriptively by calculating Bayesian 95% CrI of proportions using a Bernoulli likelihood model and then expressed as percentages. We investigated the bivariate (unadjusted) relationships of each respondent and care home characteristic with 1) severity of moral distress, 2) each situation contributing to moral distress, and 3) each symptom related to moral distress. Bayesian proportional odds models were used to estimate the probability distribution of the odds ratio of each category of a characteristic relative to a reference category. Categories were considered to differ from its reference category if the 95% CrI of its odds ratio did not include one. Bayesian analyses started from uninformative priors. Stata 16 was used for statistical calculations. All completed surveys were included in the analysis, and listwise deletion was used for any missing values during analysis.
Respondents also provided free-text responses to open-ended questions, and we followed a deductive approach to identify themes across the qualitative dataset. Authors L.H-L., A.I., A.G., and H.Q. reviewed the text in detail, met to review the text, discuss the coding strategy, and generate initial codes related to the study objectives. As a framework for our analysis, we used the moral emotion model developed by the social psychologist Jonathan Haidt. According to Haidt (2003), moral emotions are those that are “linked to the interests or welfare either of society as a whole or at least of persons other than the judge or agent” (p. 853). Based on this model, moral distress is the result of emotions that are “other-centred”, that is, emotions that are linked to social events or experiences that have a direct impact on others, rather than the self. Moral distress is thus an emotional reaction to witnessing an unjust action done to others and/or the suffering of others. Each segment of text received a conceptual code to classify and organize the information utilizing NVivo® software.
Results
Online survey
Associations between the severity of moral distress and respondent and LTCH characteristics.
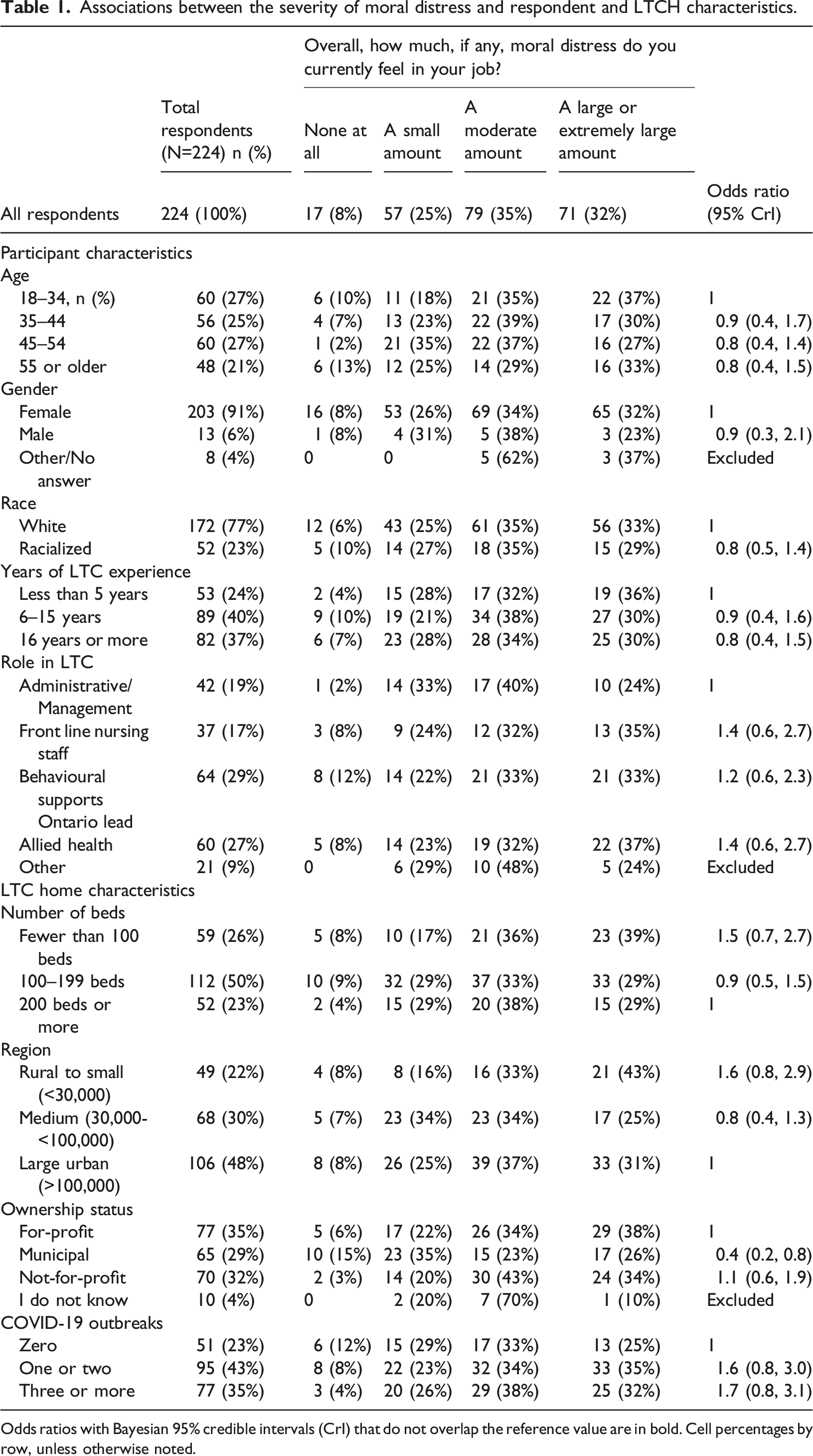
Odds ratios with Bayesian 95% credible intervals (CrI) that do not overlap the reference value are in bold. Cell percentages by row, unless otherwise noted.
The most common situations contributing to moral distress are illustrated in Figure 1. The impact of lack of activities and family visits on resident care and quality of life caused a large to an extremely large amount of distress in 60% (95% CrI 53%–66%) and 61% (95% CrI 54%–67%) respectively, across all respondents. Insufficient staff (49%, 95% CrI 42%–55%) and high staff turnover (34%, 95% CrI 28%–40%) were also associated with higher levels of moral distress. The need to follow COVID-19 policies that appeared in conflict with a resident’s best interest correlated with higher levels of moral distress in 35% (95% CrI 29%–42%) of respondents. Some situations were rarer but did contribute to higher levels of moral distress in a subset of respondents. These included: feeling unsafe when providing care to aggressive residents (19%, 95% CrI 14%–24%), observing poor care due to lack of communication (13%, 95% CrI 9%–18%) or lack of medical support (14%, 95% CrI10%-20%) and observing poor symptom control for residents (13%, 95% CrI 9%–18%). A small number of respondents (4%, 95% CrI 2%–8%) endorsed having encountered a situation where they witnessed but did not report neglect or abuse. Situations contributing to moral distress related to dementia care in LTCH during the COVID-19 pandemic.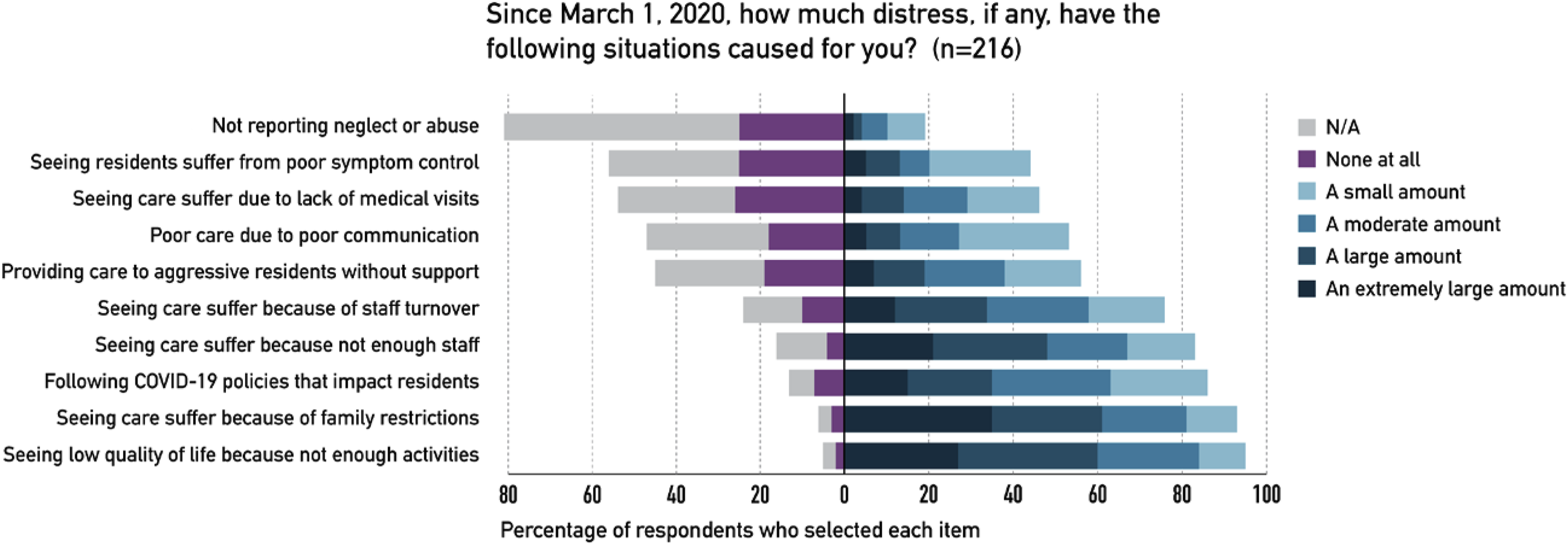
Associations between situations contributing to moral distress and respondent and LTCH characteristics.
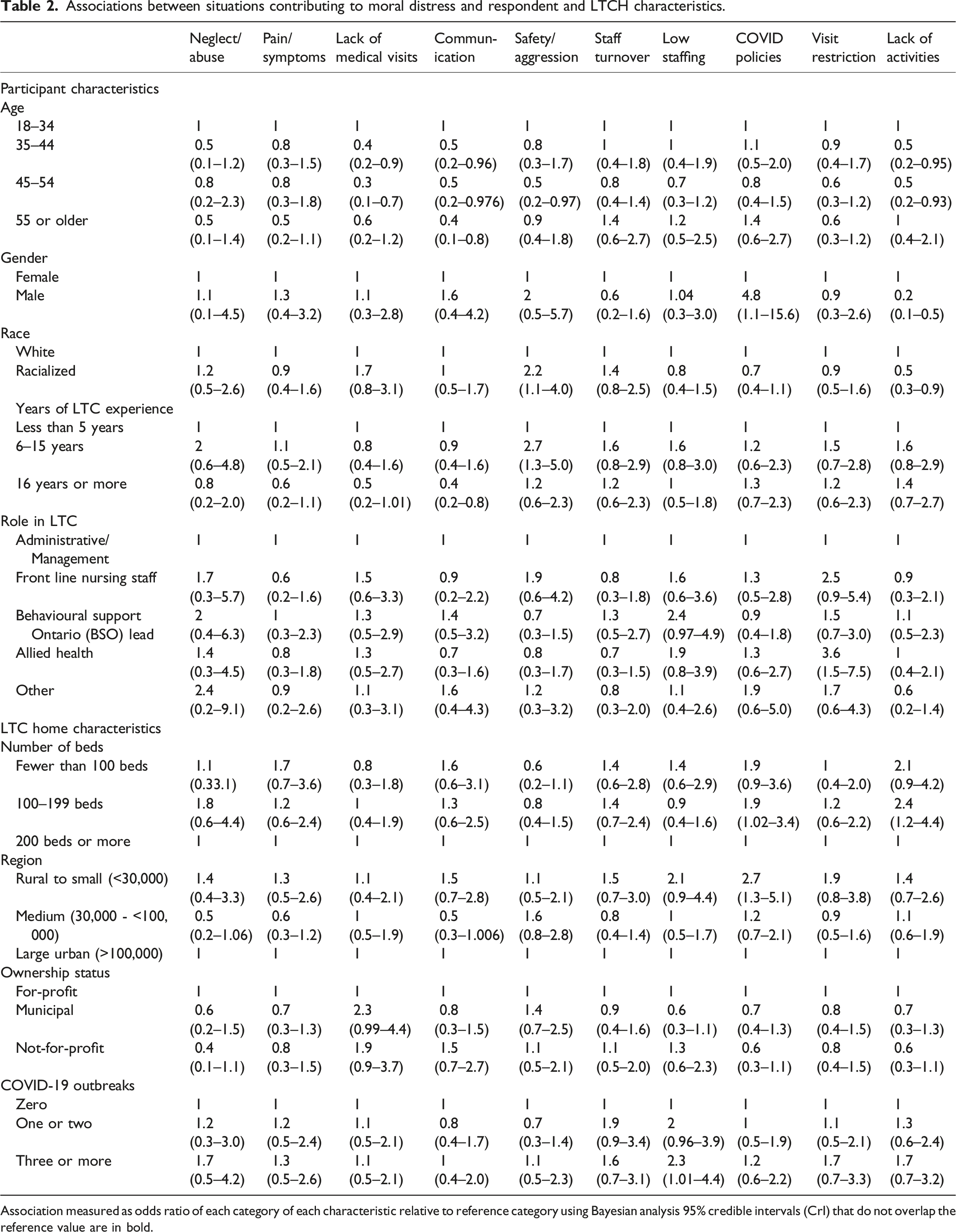
Association measured as odds ratio of each category of each characteristic relative to reference category using Bayesian analysis 95% credible intervals (CrI) that do not overlap the reference value are in bold.
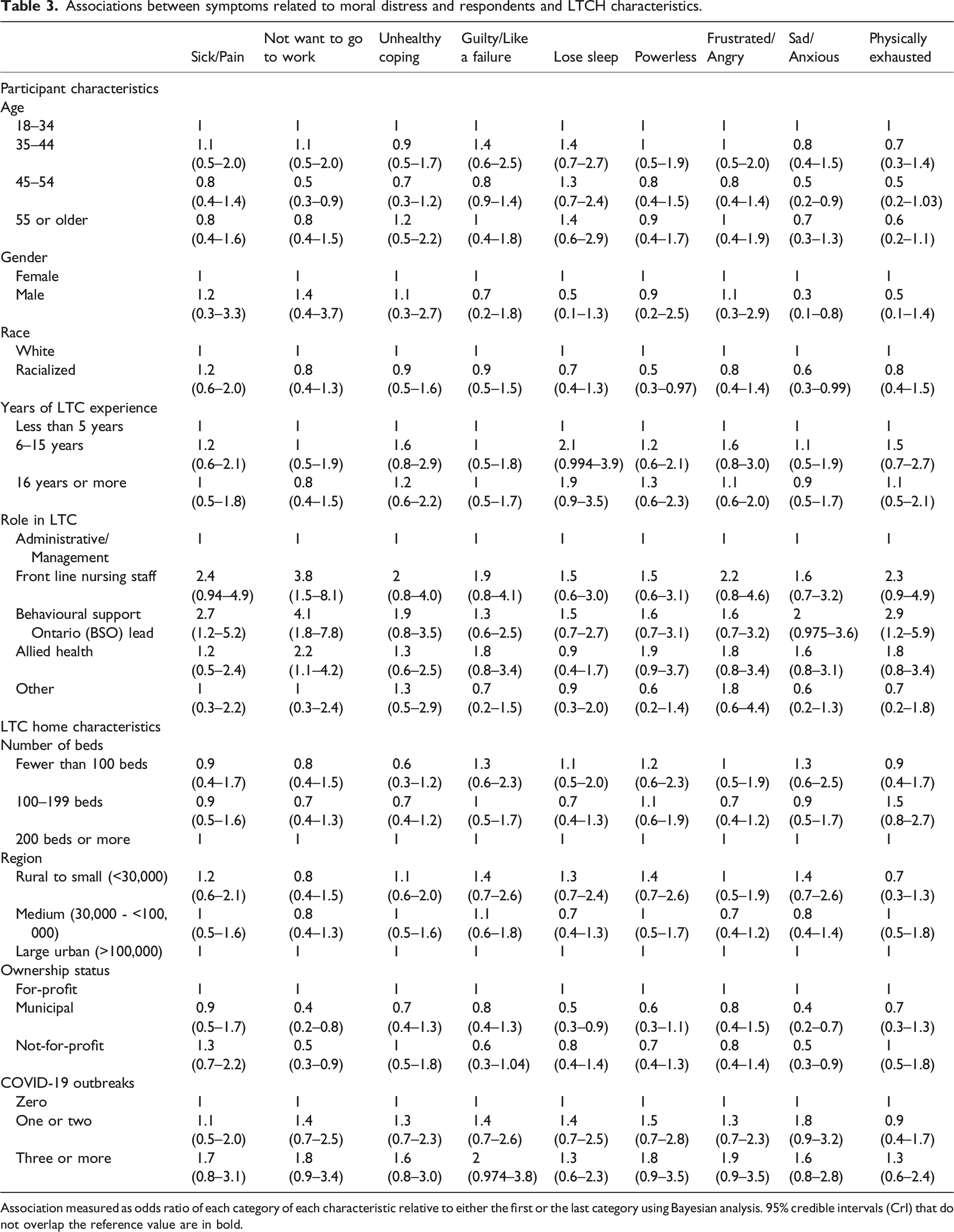
The impact of moral distress on staff well-being is illustrated in Figure 2. Physical and emotional symptoms related to moral distress were frequently experienced more than once a week, with the most common being physical exhaustion (55%, 95% CrI 48%–62%), powerlessness (39%, 95% CrI 33%–46%), sadness/anxiety (38%, 95% CrI 32%–45%), frustration/anger (31%, 95% CrI 25%–38%), and difficulty sleeping (33%, 95% CrI 27%–40%). The relationships between respondent and care home characteristic and symptoms of moral distress are examined in Table 3. Men were less likely than women to report feelings of sadness/anxiety (OR 0.3, 95% CrI 0.1–0.8). Compared with white participants, racialized participants were less likely to report sadness/anxiety (OR 0.6, 95% CrI 0.3–0.99) and powerlessness (OR 0.5, 95% CrI 0.3–0.97). Front-line nursing (OR 3.8, 95% CrI 1.5–8.1), Behavioural Support Ontario Lead (BSO) (OR 4.1, 95% CrI 1.8–7.8) and allied health staff (OR 2.2, 95% CrI 1.1–4.2) were more likely to report not wanting to go to work compared to administrative/managerial respondents. Finally, employees of municipal and not-for-profit homes were less likely to report sadness/anxiety (municipal OR 0.4, 95% CrI 0.2–0.7; not-for profit OR 0.5, 95% CrI 0.3–0.9) and not wanting to go to work (municipal OR 0.4, 95% CrI 0.2–0.8; not-for profit OR 0.5, 95% CrI 0.3–0.9) compared to those working in for-profit homes. Impact of moral distress on LTCH staff well-being during the COVID-19 pandemic. Associations between symptoms related to moral distress and respondents and LTCH characteristics. Association measured as odds ratio of each category of each characteristic relative to either the first or the last category using Bayesian analysis. 95% credible intervals (CrI) that do not overlap the reference value are in bold.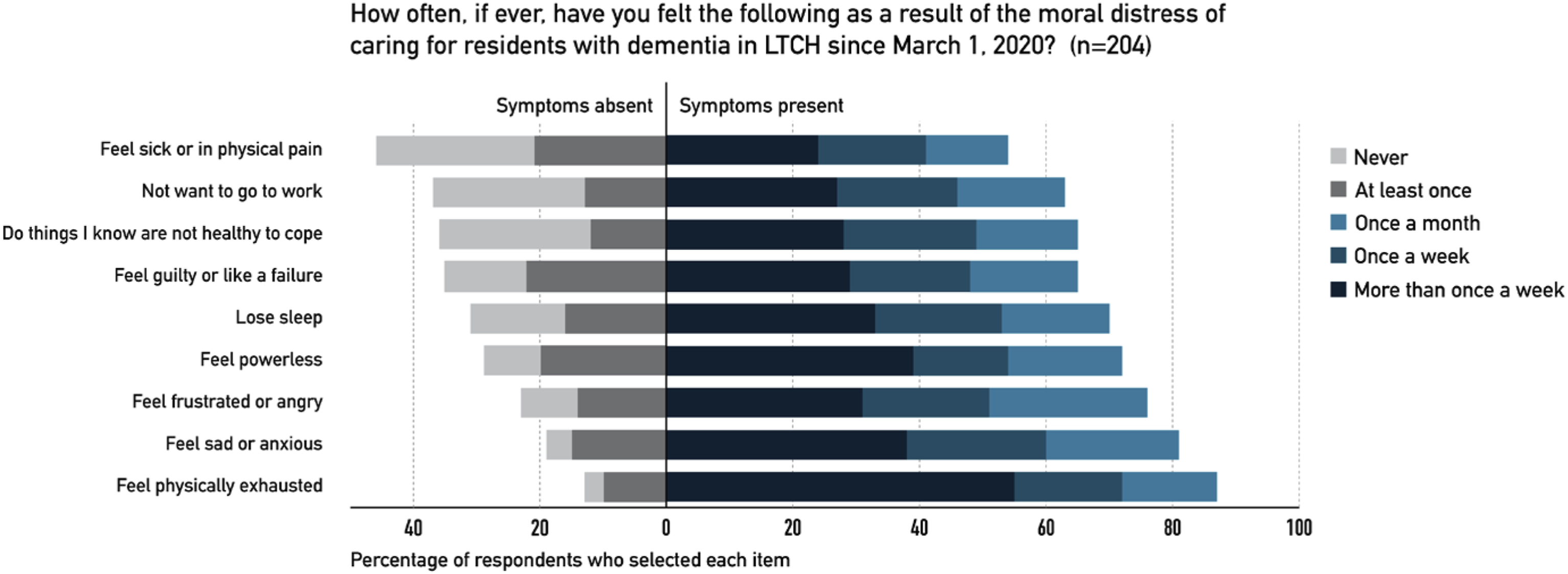
Qualitative analysis of free text
A total of 36 respondents (16%) provided free-text responses that described how pandemic protocols changed care delivery and the resulting emotional impact on staff. The four categories of moral emotions as described by Haidt (2003) were used as a framework for analysis: “other-condemning” emotions, “self-conscious” emotions, “other-suffering” emotions, and “praising” emotions (Haidt, 2003; Jiménez-Herrera et al., 2020).
Condemning emotions include anger, distrust, and contempt and these were the most common emotions shared in the open text responses. Narratives coded within this category expressed frustration about the healthcare system and hierarchies in the care home setting that were perceived as barriers to moral action. Staff reflected on ageism and discrimination: “I feel that long-term care is a microcosm that reflects societal values in general. That is what I find is distressing. It seems that we do not, in fact, value the lives of older adults to the degree we say that we do” (physician, #3849, age 35–44). Anger was apparent when reflecting on a lack of resources and the impact on residents: “I am so disgusted by the way long-term care is being run in the pandemic, I feel that staff ratios are horrendous” (recreation/life enrichment, #1764, age 35-44). Several respondents expressed frustration with funding models: “it seems that an already broken system has now become more broken, yet profits are still being made” (recreation/life enrichment, #2953, age 35–44). Finally, a growing distrust with leadership was evident: “administration is behind closed doors causing a lot of distrust and dislike amongst the staff” and “management blames everything to their staff while they just sit in their offices” (BSO staff, #3289, age 35–44).
Self-conscious emotions include shame, embarrassment, or guilt that come from experiences where an individual feels that they have violated a norm, failed to live up to standards, or caused someone else harm. The respondents tended to focus more on systemic rather than individual failings, thus these emotions were relatively rare. An example of this theme is when a respondent shared “it is very hard to watch people stare at walls all day when it is your actual job to prevent this” (recreation/life enrichment, #2063, age 45–54). Other respondents described the experience of letting down the residents: “our residents deserve much more then what we are able to provide on a daily basis” (BSO staff, #369, age 18–34) and “we are failing our seniors and we continue to do so, and that fills me with despair” (recreation/life enrichment, #404, age 45–54).
Empathy and compassionate emotions are defined as those responses “that stem from another’s emotional state or condition and is congruent with the other’s emotional state or condition” (Haidt, 2003). These narratives reflected emotions experienced by staff observing the suffering experienced by residents. Many staff shared that it was “really difficult”, “extremely tough”, and “really sad” to watch the residents connect with family members through balcony or window visits. The perceptions of resident solitude weighed heavily on many staff: “residents respond to touch and not allowing families to touch their loved ones is hard on everyone” (recreation/life enrichment, #3364, age 55 or older). Lastly, a provider reflected that “I tear up thinking how time was spent providing basic care to residents with dementia, and perhaps could not grasp the nature of this emergency, and who never got to see or be with their loved ones again” (BSO staff, #2493, age 35–44).
Praising emotions are positive emotions, demonstrating gratitude and elevation. In this type of narrative, staff conveyed a sense of gratitude or described ways to find meaning and value within their work. One staff member articulated the concept of elevation – where one desires to become a better person: We do it because of our moral compass, compassion, ethics, values, etc. We are there, doing all the time, the front-line providers. We are in the trenches with the residents, trying to be everything to them, without any thought to ourselves (recreation/life enrichment, #404, age 45–54).
Discussion
In an online survey of people working in long-term care homes throughout Ontario, Canada, we found that more than 80% reported an increase in moral distress during the pandemic, and 67% described moderate to extreme amounts of moral distress. Many pandemic-related situations contributed to this distress in staff, particularly the loss of activities and contact with family. Moral distress impacted staff well-being, with 33%–55% of staff reporting symptoms of physical exhaustion, sadness and anxiety, frustration or anger, and difficulty sleeping related to moral distress. The severity of moral distress was similar across all demographic categories. However, some association was found between the participant characteristics of age, years of experience, gender, ethnicity, and role, as well as the different situations that contribute to distress, and the symptoms of distress. The severity of moral distress was also similar across care home characteristics, although there were some differences between rural and urban homes and between those homes run for-profit versus municipally-run or not-for-profit homes. Free-text responses reflected staff sentiments of frustration with the system, distrust in leadership, and their emotional reaction to the situation at hand. These results are consistent with previous findings that moral distress impacts attitudes, job satisfaction, and burnout (De Veer et al., 2013; Lamiani et al., 2017).
The COVID-19 pandemic both created new and exacerbated pre-existing factors contributing to moral distress in long-term care homes. Prior to the pandemic, low staffing ratios and staffing shortages were among the most significant contributors to moral distress in care homes (Pijl-Zieber et al., 2018), and the pandemic worsened these problems. Pandemic protocols significantly increased staff workload, as the staff needed to change the model of care to meet the needs of so many isolated residents (e.g., no communal meals or activities), and staff were required to frequently screen the entire care home population for symptoms of COVID-19 (Chief Medical Officer of Health, 2021; Long-Term Care Staffing Study Advisory Group, 2020). Additionally, the burden of an increased workload was exacerbated by staffing shortages due to staff-related COVID-19 illness. Situations where providers feel they are ‘spread too thin’ or perceive that the care model requires ‘trade-offs’ to meet care needs are ripe for moral distress (Spenceley et al., 2017; Varcoe et al., 2012). Existing staffing shortages became critical during the outbreaks, as the workforce were exposed, symptomatic, or infected and unable to work. This was consistent with our finding that working at a care home with more than three outbreaks was associated with staff reporting higher moral distress related to low staffing.
In general, the degree of moral distress was not influenced by whether participants worked at a care home that had experienced an outbreak, suggesting that staff experienced moral dilemmas based solely on having to follow the pandemic-related organizational directives. For example, people working at rural homes, where there was less community spread and risk of COVID-19 in Ontario, reported increased moral distress due to COVID restrictions that may have felt unnecessary or excessive. Staff were asked in a very short time frame to shift their perspectives from a person-centred focus of care, to a public health focus that safeguarded the community and placed limits on the movements and activities of residents (Iaboni et al., 2020). Spenceley et al. (2017) found that care home staff feel ‘unavoidably complicit’ in care that they perceive to be inadequate, and expressed moral distress in particular with provision of care that conflicts with a resident’s wishes. Although the pandemic isolation protocols were important for infection control, staff experienced conflict over whether they were in the best interests of individual residents.
Notably, working in a municipally-run care home was associated with less moral distress, and those working in municipally-run or not-for-profit homes reported less sadness/anxiety/insomnia and were less likely to not want to go to work due to their moral distress, compared to for-profit homes. Municipally-run homes in Ontario, in general, have supported their staff during the pandemic by providing pandemic pay, hiring and redeploying other municipal staff, and using municipal funds to improve ventilation, and provide protective equipment and antigen testing (Rider, 2021). It is an important finding that these supports were associated with less moral distress in staff. Research has shown that for-profit homes had poorer outcomes during the first waves of the pandemic, in particular larger outbreaks and more deaths, which may have had an impact on staff morale in these settings (Braun et al., 2020; Ibrahim et al., 2021; Stall et al., 2020). Previous work has found an association between for-profit status and lower quality of care, although few studies have specifically examined the relationship between for-profit care and moral distress in staff (Hillmer et al., 2005; Winblad et al., 2017). Future studies should explore in more depth the impact of profit-seeking in the context of aged care, and the constraints imposed by cost-cutting practices and inadequate funding, on staff moral distress.
Age, years of experience, gender, race, and role within the setting were associated with different experiences of moral distress. Older staff were less distressed about lack of communication and physician support. Moral distress was more common in situations where providers felt unsupported by colleagues, where there was poor physician-nurse collaboration, and when providers felt they were excluded from decision-making (Corley et al., 2005; Hamric & Blackhall, 2007; Sauerland et al., 2014). Younger staff may have felt a need for an explicit source of direction from those with more experience, or connection to those with the power to make decisions, whereas the older staff may have felt better equipped to face the unpredictability of situational challenges. Another notable finding was that racialized staff reported more moral distress related to feeling unsafe when facing aggression from residents without support. Workplace violence is under-reported but common in care homes, as is racially charged abuse of staff in these environments (Berdes & Eckert, 2001; Dodson & Zincavage, 2007; Xiao et al., 2021), and there may be scope for future studies to examine the relationship between moral distress and gaps in support for the harms related to racism in this setting. Finally, those in front-line roles were more likely to endorse not wanting to go to work compared to those in management or administrative roles. This role differentiation has been reported in the literature, with staff closer to the bedside experiencing more moral distress (Pijl-Zieber et al., 2018). Nurses often perceive that those in leadership positions do not understand the reality of care in a care home environment (Spenceley et al., 2017) and several respondents in our study expressed distrust of leaders. Overall, our findings highlight the need to support young staff, address inequities in this largely racialized and gendered workforce, and find a way to address a sense of abandonment by leaders of those at the front-lines to prevent burnout and staff turnover settings. Moral resilience can be strengthened by development of an environment which allows clinicians to practice in a manner that reflects their intentions, character, and integrity (Rushton, 2017).
The impact of the pandemic and subsequent restrictive protocols invoked a range of moral emotional responses from staff. The most prominent were condemning emotions – contempt, anger, and disgust. Although generally viewed to be negative, these emotions signal a perceived violation of a resident’s rights and fairness, disrespect, and duty (Rozin et al., 1999). Staff articulated disappointment in the care home system structure and how they felt the system was “failing” the older adult population, with a particular focus on the contributions of staffing shortages to moral distress (Greason, 2020). Several respondents highlighted suffering emotional reactions – empathy and compassion. Healthcare providers were affected by witnessing the impacts of isolation on residents. Prolonged experiences of empathy can lead to moral distress, burnout, and loss of trust in the healthcare system (Riess, 2017). Despite this, many participants found ways to remain resilient. Staff articulated pride in their work, recognition that residents needed them, and statements about finding fulfillment in their work. Finding meaning in one’s work can be an ‘antidote’ to moral distress, as resilience is strengthened when staff are able to connect back to their primary intentions (Rushton, 2017). An area for future research would be to identify interventions that support resilience, such as education and training, mental health interventions, and peer and social support (Ontario Agency for Health Protection and Promotion (Public Health Ontario), 2021). Studies have found the relationships between staff and residents build emotional connections, and create a sense of accountability to the residents (McGilton et al., 2007; Spenceley et al., 2017). As demonstrated through their emotional narratives, staff did have empathy and compassion for the residents, with many sharing that they ‘tried their best’ to be present for the residents when families were unable to visit.
A strength of the study was that it included a range of healthcare staff in various roles, including nurses, support workers, recreational therapists, management/administration, and all levels of expertise within the long-term care home environment from across Ontario. The study also had several limitations. First, our smaller than anticipated sample size reduces the power of the study and increases the margin of error in our quantitative results. Second, participants self-selected into the study; thus, it is important to be cautious when generalizing from this sample to the broader population of care home staff. The main survey instrument asked questions specific to the moral distress experienced by staff while providing dementia care. However, it is possible that staff reflected on their broader experience working in long-term care during the pandemic in answering some of the questions. Third, most survey items used structured responses, which may have narrowed the range of responses from staff, although this was mitigated by providing an open-ended question. Further qualitative studies are needed to explore this topic in greater depth.
Long-term care home settings are characterized by high levels of employee moral distress. Although we found moral distress was exacerbated by the pandemic crisis, this is a historic and ongoing area of concern given the fundamental structural issues, inequities, and constraints faced by those employed in care homes. Long-term care home organizations face the challenge of creating an ethical environment that delivers high-quality, person-centred care to its residents, and supports the well-being of providers by encouraging supportive teamwork, empathetic leadership, and validation of providers’ efforts (Phoenix Australia – Centre for Posttraumatic Mental Health and the Canadian Centre of Excellence – PTSD, 2020). Future research is needed to study promising interventions designed to support moral resilience in staff by helping to recognize and resolve moral conflicts and take actions that preserve moral integrity.
Supplemental Material
Supplemental Material - Prevalence, causes, and consequences of moral distress in healthcare providers caring for people living with dementia in long-term care during a pandemic
Supplemental Material for Prevalence, causes, and consequences of moral distress in healthcare providers caring for people living with dementia in long-term care during a pandemic by Lynn Haslam-Larmer, Alisa Grigorovich, Hannah Quirt, Katia Engel, Steven Stewart, Pia Kontos, Arlene Astell, Josephine McMurray, AnneMarie Levy, Kathleen S. Bingham, Kevin Rodrigues, Alastair J. Flint, Colleen Maxwell, Andrea Iaboni in Dementia
Footnotes
Acknowledgments
We would like to thank the Survey Research Centre at the University of Waterloo for the expert administration of the Dementia Isolation Toolkit survey.
Authors Contributions
Authors AI, AG, PK, AA, and AJF conceived the current study. The survey was designed and developed by authors AI, CM and HQ and reviewed with substantial input from AG, PK, KB, KR, AA, and AJF. The quantitative analysis was completed by AI, SS, and HQ, and LHL, AG, HQ, and AI completed the qualitative analysis. KE, AG, PK, JM, AL, KB, KR, AA, AJF and CM contributed to the interpretation of the analysis. The manuscript was written by LHL and AI and substantially revised by HQ, KE, AG, PK, JM, AL, KB, KR, AA, AJM and CM, and all authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author A.J. Flint discloses grant support from the U.S. National Institutes of Health, Patient-Centered Outcomes Research Institute, Canadian Institutes of Health Research, Brain Canada, Ontario Brain Institute, AGE-WELL, and the Canadian Foundation for Healthcare Improvement. The remaining authors have no conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funds from the Province of Ontario Rapid Access COVID-19 research grant; the Walter and Maria Schroeder Institute for Brain Innovation and Recovery; an Academic Scholars Award from the Department of Psychiatry, University of Toronto (AI); and the Neuropsychiatric Symptoms team (Team 11) of the Canadian Consortium on Neurodegeneration in Aging, which is supported by a grant from the Canadian Institutes of Health Research with funding from several partners. Funders had no role in the design, data collection, analysis or preparation of this manuscript for publication.
Availability of data and materials
The survey data used in this study is provided in an aggregate form as supplementary material. The raw survey datasets generated and/or analysed during the current study are not publicly available as they contain information which could be used to re-identify participants, but the data are maintained in an institutional data repository and are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The study was reviewed by the University Health Network Research Ethics Board (REB#20–5866) and a University of Waterloo Research Ethics Committee (ORE#42803). All survey participants provided informed consent to participate by clicking a button that indicated they had reviewed the consent information and agreed to proceed to the survey.
Consent for publication
Participants provided consent for the publication of anonymized data
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.