
Abstract
The identification of human rights issues has become more prominent in statements from national and international nursing organisations such as the American Nurses Association and the United Kingdom’s Royal College of Nursing with the International Council of Nursing asserting that human rights are fundamental to and inherent in nursing and that nurses have an obligation to promote people’s health rights at all times in all places.
However, concern has been expressed about this development. Human rights may be seen as the imposition of legal considerations for nurses and other healthcare workers to bear in mind, as yet more responsibilities with the consequent fear of litigation. Although a more hopeful scenario is that consideration of human rights is something that is supportive of good practice.
If this more hopeful scenario is to be realised, the role of education will be crucial. As with human rights generally, human rights education is a global phenomenon, a practice-orientated expression of the Universal Declaration of Human Rights, and the goal of human rights education is to build a culture of respect and action for human rights for all.
However, the nature of human rights has long been contested. A ‘mapping exercise’ of the academic literature on human rights identified ‘four schools’ or ‘ideal types’ that have shaped thinking about human rights. This sets out the conceptual context in which human rights problems are defined and solutions are proposed, which is particularly important for human rights education. However, it also complicates the picture. The different approaches taken by the four ‘types’ would likely lead to different outcomes in terms of human rights education.
It is timely to discuss the nature of human rights education and examine its potential for impact on patient care. This will involve identifying the challenges and potential benefits of this approach and analysing the implications for professional practice.
Introduction
The identification of human rights issues has become more prominent in statements from national and international nursing organisations such as the American Nurses Association 1 and the United Kingdom’s Royal College of Nursing 2 with the International Council of Nursing (ICN) 3 asserting that human rights are fundamental to and inherent in nursing and that nurses have an obligation to promote people’s health rights at all times in all places. These assertions are based on the claim that nursing, in common with other healthcare professions, has a statutory framework of self-regulation founded on an ethical code that constitutes a ‘social contract’ with the public so is ‘…in harmony with the defence and promotion of human rights’ (p. 7). 4 If this ‘contract’ is to be maintained, the changing demands that developments in human rights make on practice need to be considered.
However, concern has been expressed about this development: There is a danger that rights may be seen as another bureaucratic imposition and yet another legal consideration for nurses [healthcare workers] to bear in mind, as yet more responsibilities with the consequent fear of litigation. A more hopeful scenario, however, is that consideration of rights is something that is supportive of good practice and will form part of critical reflective nursing [healthcare] practice, with nurses [healthcare workers]working in partnership with patients and colleagues to maximize the efficacy and quality of health care. (p. 232)
5
However, the nature of human rights has long been contested. 8 –11 A recent ‘mapping exercise’ of the academic literature on human rights identified ‘four schools’ or ‘ideal types’ that have shaped thinking about human rights. They are natural scholars, deliberative scholars, protest scholars and discourse scholars that provide a summary of the positions taken. 12 This is helpful as it sets out the conceptual context in which human rights problems are defined and solutions are proposed. This is particularly important for human rights education, which aims to embed human rights norms in core social institutions, such as healthcare services. 7 However, it also complicates the picture somewhat in that the different approaches taken to the issues as informed by the four ‘types’ would likely lead to different outcomes in terms of human rights education 12 for healthcare institutions, nurses, other health care staff and patients.
It is timely to discuss the nature of human rights education and examine its potential for impact on patient care. This will involve identifying the challenges and potential benefits of this approach and analysing the implications for professional practice. With this in mind, this article is divided into two broad sections. First, the findings from a literature review of relevant studies and evaluations of human rights education in patient care are presented. 6 This reports from a broader perspective than nursing and includes material relating to other healthcare workers and patients. This was necessary because the available literature on human rights education is limited. 6 This is followed by a critical discussion of the implications of the findings. The overall focus of this article is to subject the burgeoning trend towards human rights education in health care to critical scrutiny and identify the potential for impact on professional practice.
Literature review
The aim of this literature review was to critically examine a range of literature on human rights education in patient care in order to evaluate why and how it was used and, where possible, to determine its effect on patient care and its implications for professional practice.
Ethical considerations
No ethical approval was required for this literature review.
Methodology
The design was a literature review. Electronic searches were conducted using Ovid MEDLINE, ProQuest, Embase, PubMed and CINAHL databases. The search terms were a combination of ‘Human Rights Education’ OR ‘Human Rights Based Approach’ AND ‘Patient Care’ OR ‘Healthcare’. The Google Scholar advanced search facility was used because it can identify the ‘grey’ literature. Hand searching of the specialist journals Human Rights Education Review and Journal of Human Rights Practice was carried out to ensure that no key papers were overlooked. Database searches and abstract and full-text screening were undertaken between July and August 2019 with no date restriction. The inclusion and exclusion criteria for the search are included in Table 1.
Inclusion and exclusion criteria.
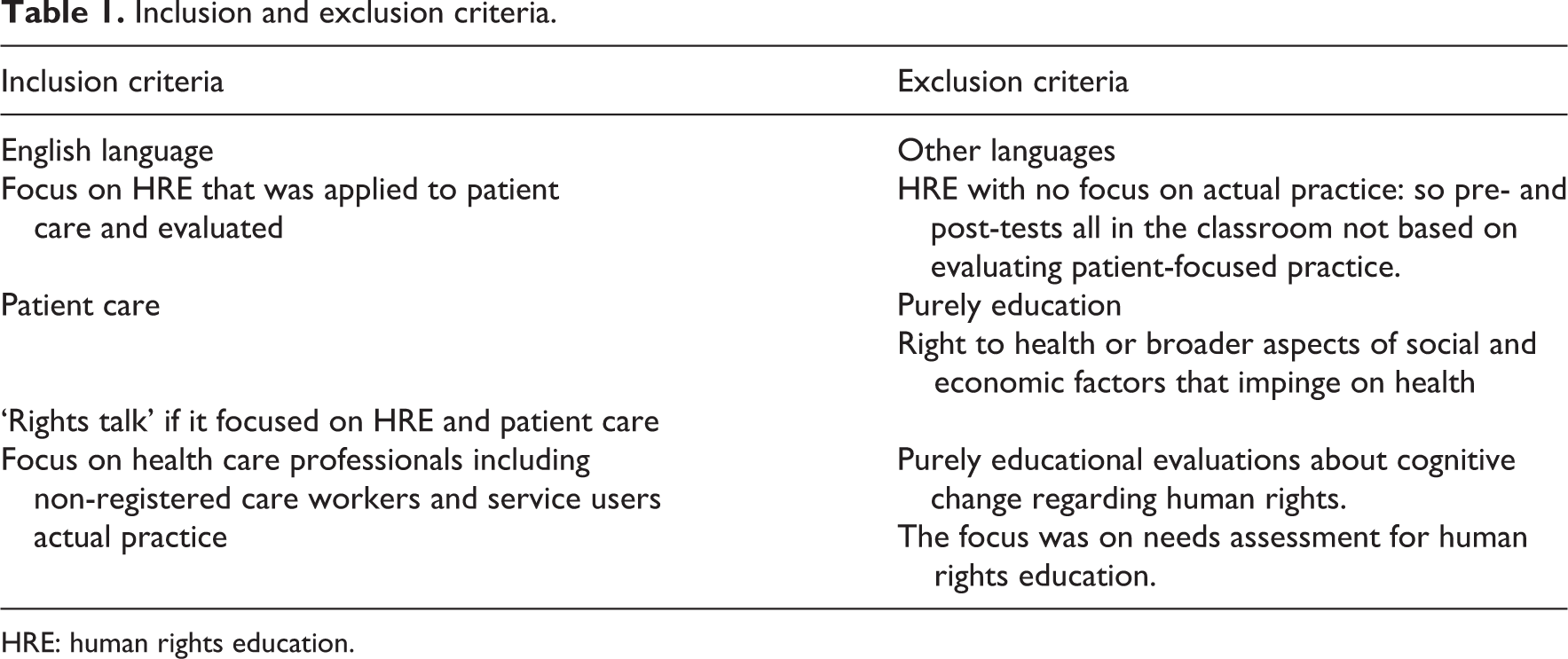
HRE: human rights education.
Eligibility: inclusion and exclusion criteria
Data evaluation
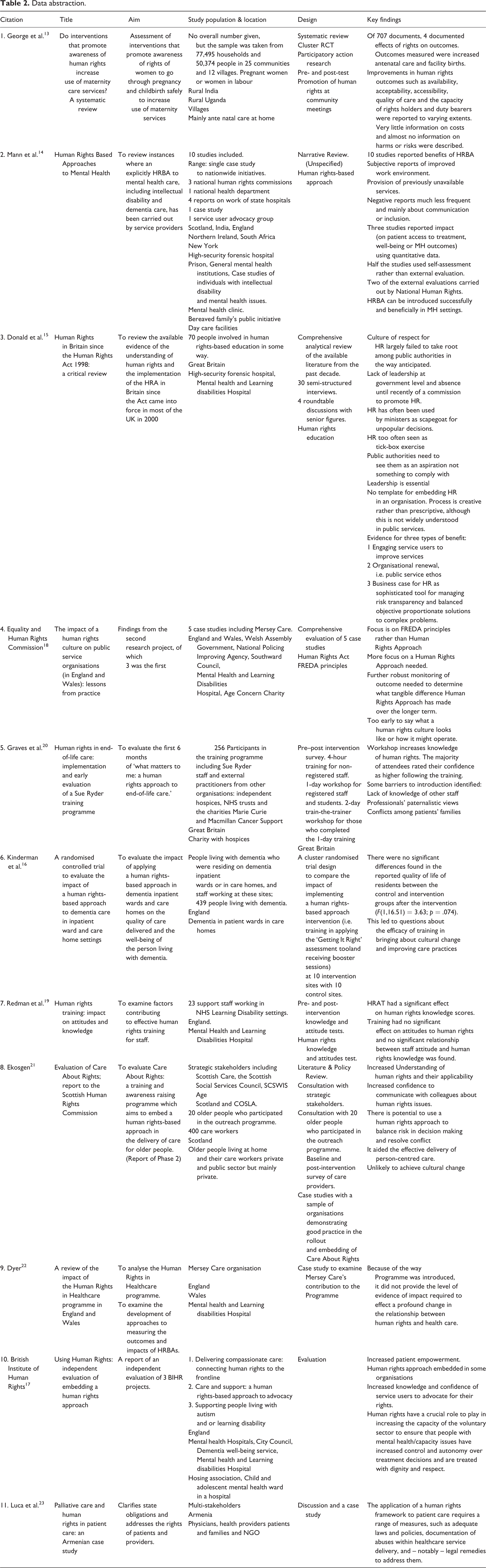
The study design and/or the approaches taken in each of the papers are summarised in Table 2. No papers were excluded on the basis of quality because of the limited number of relevant papers found, and there was no date restriction set in order to maximise the likelihood of finding relevant studies. All papers were reviewed independently by two reviewers for relevance and quality.
Of the 11 papers, 3 were reviews. 13 –15 Of the eight remaining papers, one reported a randomised controlled trial, 16 two were evaluations, 17,18 two were non-randomised uncontrolled pre- and post-test service evaluation studies, 19,20 one was a mix-review case study and interview-based evaluation 21 and two were case studies conducted as service evaluations. 22,23 Only the systematic review and randomised controlled trial described the methodologies used in detail. Of the 11 papers included, only one was a primary research study, and research ethics approval was reported as a registered trial. 16 The remaining papers were reviews or service evaluations which did not report research ethics approval.
The randomised controlled trial was of very good quality when examined using the Critical Appraisal Skills Programme (CASP) RCT 24 checklist. The systematic review was also deemed to be of good quality based on the CASP systematic review 25 checklist. The lack of randomisation and control in the pre- and post-tests weakened their rigour as did the low level of post-test completion. The reviews were carried out independently of the organisations that delivered the human rights education programmes.
Data analysis and synthesis
The analysis involved a critical review synthesising the findings presented in the papers. A thematic approach was used. Data from all the papers were extracted, coded and iteratively compared for similarity of topic, interpreted and grouped together under more general themes and relationships between the themes identified. Finally, conclusions were drawn to produce an integrated picture of human rights education in healthcare.
Results
From a total of 854 potential papers identified by electronic searches, 489 were selected based on their title, 200 on the abstracts and 10 following review of the full-text versions. The Google Scholar advanced search tool identified four studies. Hand searching of Human Rights Education Review and Journal of Human Rights Practice produced no further papers. A total of 11 articles were identified for inclusion in the review. The PRISMA flowchart 26 framework was used to report the search and retrieval element of the review (see Figure 1). Table 2 includes a summary of the type of papers and studies including the geographic location of the work reported. Studies were conducted in a variety of areas and settings ranging from homes in rural villages, public mental health hospitals, public and private acute hospitals, to charities and NGOs (see Table 2).
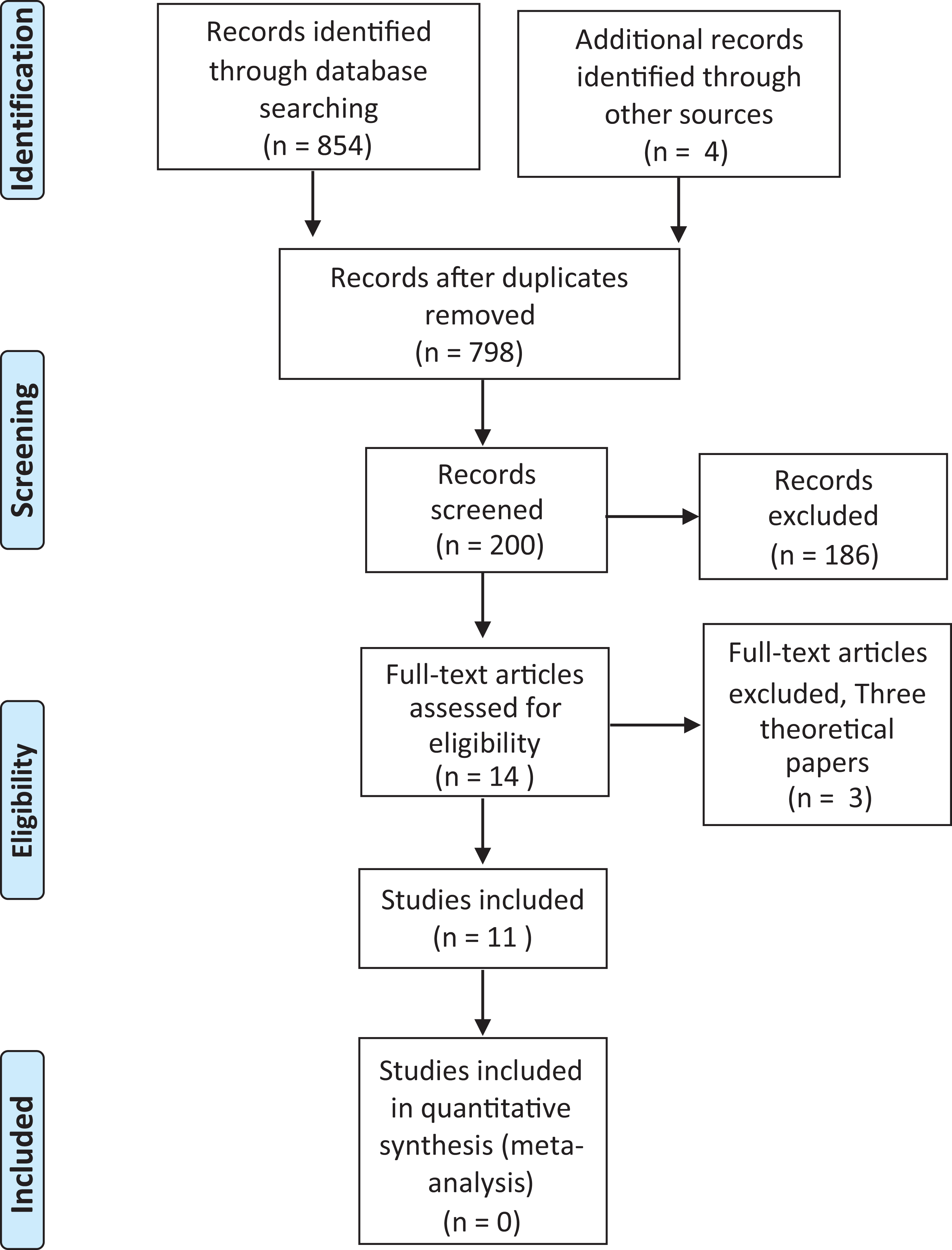
PRISMA flowchart of the integrative literature review. From: Moher et al. 26 For more information, visit www.prisma-statement.org
Data abstraction.
Four themes were found: embedding a human rights culture; developing the decision-making skills of staff; developing assertiveness of patients to improve services, and barriers to implementing an human rights education approach to patient care. These are discussed below.
Embedding a human rights culture
Two papers referred to the moral nature of human rights thought necessary for human rights to be embedded in healthcare practice and that this was a reason for recourse to human rights education.
14,15
One study claimed that the moral nature of human rights in practice was important even if it resulted in no change in outcomes because ‘human rights are fundamental pillars of justice and civilisation’ (p. 263).
14
An example of the moral importance of human rights education was where human rights were linked to the idea of a ‘public service ethos’, which for health care workers could plausibly be understood as a moral ethos defined in the paper concerned as [the]: ‘Ethos of caring in social work, the Hippocratic Oath for medical professionals and ethical standards in local government’ (p. 62).
15
Similarly, human rights education can ‘…reconnect staff with their original motivation for taking up their profession’ (p. viii).
15
A participant in the study, presumably a social worker, stated: [R]ather than seeing human rights as yet another regulatory burden social workers on the ground are enormously excited once they start to see what it could mean. It very much resonates with the care professionals’ idea of what their job is all about. (p. 63)
15
It was argued that to embed a human rights culture in health care organisations, human rights need to be made contextually meaningful to practitioners and patients. 17,21,22,25 In several of the studies included in this review, participants (both professionals and patients) commented that the examples used in human rights education were relevant and beneficial, enabling them to make connections between what was taught and their own experiences. 14,17,19,20 In some cases, it was the moral principles of FREDA or PANEL that participants found particularly relevant to practice and reported using them rather than the articles of human rights law. 13,15,22
To embed a culture of human rights using human rights education in patient care organisations, high-level management support was required 15,18,21 –23 even if healthcare professionals took the lead and managed implementation. 23 For example, in Armenia, the Ministry of Health developed national standards for palliative care. Without such support, or where support is intermittent, efforts to embed human rights education are likely to fail. 18,22,23
In the United Kingdom, reviews of studies conducted before 2015 22 suggest that despite human rights education, human rights had not been embedded in public authorities (public authorities defined here as those with statutory powers, such as the NHS or the Police, in contrast to ‘hybrid’ arrangements, where private and charitable organisations provide a public service). Two reasons for this are offered by way of explanation. First, in the decade following the ratification of the UK Human Rights Act in 1998, there was a lack of leadership from government and so an opportunity was missed to use the Human Rights Act as a tool to improve delivery of public services (p. iii). 22 Second, although there were some government-led initiatives to embed human rights in public services in England and Wales, which led to small but important changes, overall, there is a lack of evidence of the effectiveness of HRBAs, including human rights education, in health services (p. 120). 14,19,22 Similarly, where there seems to be some evidence of effectiveness, it is acknowledged that it can only be an indication that human rights education may be successful because of its limited nature. 14,19,22 In one paper, human rights were not explicitly mentioned even though they seem to have been used via other terminology and laws. 13
Although embedding human rights is the focus of this theme, it is difficult to consider it without discussing the impact of human rights education. Embedding human rights through human rights education involves continuing change if long-term effectiveness, in terms of placing human rights at the centre of healthcare, is to be achieved. All the studies claimed that human rights education increased healthcare professionals’ or carers’ knowledge of human rights values or/and (for UK studies) the Human Rights Act. However, this did not necessarily have an effect on staff attitudes or behaviour. One study found no significant statistical change in attitudes and/or relationship between a change in attitude and knowledge of human rights following human rights education. 19 (The pre-test score for attitudes was high and the training focussed on cognitive rather than emotional change, which may explain the limited change). A randomised controlled trial involving 439 participants found no difference in patient care resulting from an human rights education programme, which questions the efficacy of human rights education in bringing about cultural change, even when there is a positive change in attitudes and an increase in knowledge (p. vi). 16 In contrast, a qualitative synthesis of mental health care indicated that there was both a positive change in staff attitudes and improved outcomes, including increased patient satisfaction and a reduction in the use of seclusion following an human rights education programme, although it was noted, there was a need for more rigorous research to investigate the impact of human rights education on these outcomes. 18 A review which examined the effect on health outcomes of human rights interventions in maternal health found that four studies reported local improvements in care (3 of the 4 in rural India and 1 in Uganda) but not all the findings were statistically significant. 13 Also, there was no significant impact on the health system in the form of changes in legislation, policies, protocols or guidelines (p. 13). 13
Developing the decision-making skills of clinical in staff
All the studies reported an increase in knowledge of human rights among participants. Some also reported that the healthcare professionals and patients involved developed more confidence to use them in practice, with some participants reporting feeling able to communicate with colleagues about how human rights can improve the delivery of care. 14,16,17,20 However, some respondents in one study reported a reluctance to challenge colleagues’ views because they lacked confidence in their knowledge of human rights. 20 human rights education interventions, particularly those focussed on human rights values, can increase care workers’ confidence to balance risk in decision making. For example, 86% of 82 post-test respondents in one study reported they felt that a human rights approach could help them resolve disputes between the needs of different service users (p. 5). 21 Similarly, a pilot study designed to empower frontline mental health/capacity practitioners to deliver ‘rights respecting care’ found that the respondents believed: ‘A human rights-based approach [human rights education] has given us a process by which to make decisions in messy and difficult situations. Teams are just doing this naturally now’ (p. 7). 17
However, this was not the case in all settings. An RCT found that staff in the intervention group, who had received human rights education, resorted to hierarchical decision making and referred issues to senior staff for action, only slightly less often than those in the control group. 16 This indicates that despite claims staff made about their decision making being more person-centred, there were no changes in their actual behaviour that supported such claims. In addition, the intervention group rated hierarchical decision making second in the frequency of decision-making strategies used, behind team-working/talking to other staff. Erdman 27 points to a power differential between the patient and professional as a barrier to behaviour change, but the same could occur between professions and professionals. The authors recommend the findings be treated with caution as there may have been some conflation of hierarchical decision making and teamwork, also it was found that human rights education had a limited impact on practice. 16
Finally, the studies in this review contain little detail about how participants’ decision-making skills improved, even though examples from case studies showing changes in practice were included. 14,17,18,20,21
Developing the assertiveness of patients to improve services and care
A stated aim of a number of the human rights education projects reviewed, particularly those focussed on mental health, 14,17,19,21 older people, 19 palliative care 17,23 and gender inequality and women’s rights, 13 was to foster the development of assertiveness on the part of patients. This in turn was intended to enable them to improve services by identifying when their rights were not recognised or upheld. As with the reports of human rights education involving healthcare professionals and care workers, one study found that service users reported they had learned something new about human rights and how they related to care (p. 53). 21 Although the participants had not used their learning for a specific purpose, they had discussed their experience with family, friends and community networks. 21 This study also found that the human rights education developed an understanding of proportionality (p. 54) among advocacy workers who intended to use their new knowledge to improve their skills in helping patients express their needs, though no evaluation of the actual impact of this intention was undertaken.
In one review (of the experience of women in rural India and Uganda), a lack of reported conflict or challenge was seen as surprising because empowerment of individuals through human rights education is meant to foster challenge of power relations and change the status quo (p. 13). 13
Some organisations ensured that patients and family members were given human rights education and payment to enable them to work with managers and staff at all levels and at all stages of the programme (p. 117). 22 This may have had the effect of minimising conflict by reducing power differentials. In a postal survey of 236 patients and family carers, 94% stated that being involved in decision making showed a positive difference to them as a person and 61% reported that they were more involved in decisions about their care and treatment than they had been in the 3 years prior to the programme. 22 Positive benefits in terms of the mental health were also reported (78% patients; 79% family carers) (p. 117). 22 However, although a number of putative benefits were reported, all the studies highlighted challenges involved in delivering human rights education in patient care.
Barriers to implementing human rights education in patient care
Even with high-level policy support for embedding human rights in healthcare through human rights education from, for example, the Scottish Human Rights Commission, the Department of Health, NHS England, and the Armenian Ministry of Health, there were significant organisational, cultural and systemic barriers that hampered progress.
18,20,22,23
One review
15
identified three types of barriers in specific organisations, and four barriers in the public sector as a whole. In specific organisations, the first barrier was identified as contrasting professional and organisational cultures, the second was lack of trust and autonomy of staff and the third was initiative overload leading to inertia (p. 92). The first and second barriers reflect the conflict between a professional ethos of public service for the good of the patient and organisational imperatives driven by a market culture and an emphasis on financial efficiency (discussed below). The third is about the slow rate of organisational change where organisations adopt a wait and see approach in the form of ‘passive non-implementation’ (p. 99).
15
One example from a local authority organisation was …the avoidance of adverse publicity which might come from ‘actively promoting policies on behalf of unpopular cause’ (in this case, Travelling people). (p. 99)
15
A more general lack of interest and engagement in a human rights approach among the elected members of the organisation had an adverse effect on support for front line staff. In addition, and related to the first two barriers, was the implementation of specific improvement schemes within organisations resulting in ‘initiative overload’ and competing demands (p. 100). 15
In the public sector more widely, the four barriers were: lack of information about legal and non-legal remedies for perceived human rights concerns and inadequate independent advocacy; ‘silos of state’, which inhibit governmental cross-department working exacerbating initiative overload; the commissioning process which prioritised cost reduction over human rights considerations and lack of integration of human rights principles into professional training curricula and codes of practice. These systemic barriers are more difficult for individual organisations to address alone. 15
Finally, a further barrier to implementing human rights education in health and social care is the need for evaluation of impact to demonstrate a cause-and-effect relationship or at least being able to show that changes were driven by human rights education. 16,20,22 This is claimed to be ‘…an essential prerequisite for any profound changes in the relationship between human rights and healthcare’ (p. 120). 22 Commissioners of health services may only be persuaded to support human rights education in patient care if it can be ‘proven’ they make a difference and improve the quality of services and that they are ‘equally if not more cost effective than other interventions’ (p. 121). 22 Demonstrating a linear ‘cause-and-effect’ relationship in such a complex area of practice is inherently problematic and is explored further below.
Discussion
Human rights education for professionals, care workers and service users in patient care is intended to prevent human rights abuses and inform better and person-centred care, 13,14,17,20 –22 and this review suggests that the evidence to support such assertions is mixed. The discussion is organised into three main sections: the ethical norms of healthcare professionals, decision making, and leadership and management.
Human rights education, the ethical norms of human rights and the ethos of healthcare professionals
Two studies in this review emphasised the importance of the moral nature of human rights 14,15 irrespective of outcomes 14 and as a public service ethos understood in moral terms such as caring and the Hippocratic Oath for medical professionals (p 62), reconnecting staff with their original motivation for taking up their profession (p viii). 15 Therefore, in this view, rather than human rights education being new, it provides a renewed moral emphasis or lens on a global perspective, which transcends national nursing cultures. This is consistent with the broader human rights education literature which asserts that it can ‘…reconnect staff with their original motivation for taking up their profession’ (p. viii, emphasis added) or help with a ‘re-moralisation of healthcare’ (p. 7, emphasis added). 7 This assumes that healthcare professionals have lost or become disconnected from their ethos. Yet the professional ethos can itself be a barrier 7,22,27 to human rights education. When human rights education focuses on human rights principles (FREDA and PANEL, for example) rather than being recognised as confirmatory and enabling re-connection with professional motivation, it may be regarded as unnecessary because practice is already guided by legislation and standards set by regulatory bodies consistent with these principles. Furthermore the ‘protest’ school of human rights 12 would contend that there is a need to breech such standards and question legislation, and clearly such ‘activism’ would question healthcare professionals’ roles, particularly in countries where serious breaches of human rights are uncommon.
Decision making
A related but more specific concern about what human rights education adds to the normative concerns of healthcare professionals such as nurses is that of moral decision making and the fact that some moral decisions generally and in healthcare practice in particular can be difficult. This review has found that healthcare professionals and care workers frequently claim that human rights education, with its emphasis on law, has improved their decision-making skills in clinical practice.
14,17,20,21,27
Some studies go so far as to suggest that human rights are helpful in making concrete decisions or the best decision in the circumstance, and/or objective and proportionate decisions, unlike moral decision making.
17
However, it is important to note that healthcare professionals who have experience of the ‘general’ law do not always apply it in particular cases despite the claims about the legal process providing clear answers in such circumstances.
27
This is sometimes contrasted with moral decision making as being subjective with regard to what is morally right or wrong and characterising moral decisions as the expression of ‘mere’ personal opinion. As one participant put it It [Human rights education] gives us a shared language and an objective, values-based framework and gets away from people’s personal opinion about what is right and wrong. (p. 7)
17
The claim in this review that human rights law, unlike morality, has helped decision making may be a conflation of a criterion of right or good or law with actual decision making.
28
–30
The criterion of morality is contested and so is the law.
28
Where it is not presumed to be so contested then the law simply stipulates what its criterion is. Therefore, for example, in human rights education, its legal emphasis is the articles of the Declaration or those of the ‘International Bill of Rights’. But an important point is that the practical use made of human rights education in patient care is often difficult as interpreting and applying human rights law can be for judges. As one study emphasises The provisions of international human rights treaties…are written in open and broad language, and mere knowledge of them rarely if ever provides clear-cut answers to the real conflicts health providers face in practice. Human rights, like all law, require interpretation. (p. 6)
27
Human rights education in patient care founded on the ‘protest’ perspective of human rights 12 and developed as a ‘transformational’ form of human rights education 32 has the potential to change the way oppressed or people lacking justice think by empowerment through knowledge. For example, to be treated with respect is not something they should have to hope others will provide but something they can morally and legally demand. Advocates of this approach suggest it could transform the professional patient/service user relationship from one of ‘beggar’, being reliant on professionals’ promise, charity or mercy, to one of ‘chooser’ based on an entitlement to care. 33 Such approaches may blur professional and personal boundaries depending on the level of ‘protest’ or ‘activism’ involved.
Although healthcare professionals might recognise human rights abuse in practice, they sometimes do nothing to help prevent it despite knowing it is wrong. 34 An explanation of such inaction can be found in the literature on the ‘dual loyalty’ of healthcare professionals. This a feeling of conflicting obligations to their employing organisation and to their patients. 14,35 This dual loyalty, or perhaps fear more than dual loyalty, can place healthcare professionals in situations where they witness torture or other abuse. Yet even though they believe they would not and should not carry out such actions themselves, they refrain from acting to prevent such torture or abuse. 27,34 However, when such risk to themselves or others would be high, for example, when torture is state-sanctioned, involving healthcare professionals or otherwise, and where intervening to prevent it carried a high probability of death or torture to themselves, even moral reasoning generally holds that one is not obliged to help at such cost.
Human rights education is also implicit in professionals’ decision making. The findings from this review indicate that embedding a human rights culture is often supported by existing legislation, for example, in the United Kingdom, by the introduction of legislation such as the Mental Health Act 2007 and the Care Act 2014. 17 In this way, the legislation enhances the advancement of human rights by enshrining their principles, with which professionals should comply. 17 In this way, adhering to such legislation is consistent with upholding patients’ human rights. 22,27
The foregoing discussion may be taken to suggest that the current focus on human rights is misguided. However, an incident reported in one paper indicates it remains an issue of concern. 17 A patient detained under the UK Mental Health Act who had no access to a bathroom and was given a bucket to use for toileting and was expected to clean it. A patient advocate raised it as a human rights concern with clinical staff who agreed and resolved the situation immediately. The good thing is of course that this practice was stopped. However, it does raise questions about the clinical staff involved and the culture of professional working and institutional practices in the setting. The clinical staff surely knew that, from a moral perspective (professional morality or otherwise), what they were doing was wrong, and it only requires minimal moral acumen to recognise this, so why was it necessary to invoke human rights to stop this practice? Even if threats of legal sanctions alter the professional patient/service user relationship, it is puzzling indeed why national laws that are designed to protect patient and human agency, such as laws of consent or negligence or laws related to mental health, are not sufficient to warrant the prevention of such practice and why the use of human rights law should make the difference.
Moral requirements such as not to make patients use and clean buckets for toilets can be demanded just as legal requirements can be demanded. The latter, if a breach of human rights, however, may trigger large financial and possibly criminal sanctions. The relationship between the nurses and the patient is however altered when it takes such sanctions to change behaviour, as described in detail in the work of Edmund Pellegrino and David Thomasma 36,37 and is reflected in the concern about human rights education and nursing stated in the introduction and remains relevant to much healthcare practice. That we want healthcare professionals to intrinsically care about our good and not do so because of external imposition and threats of sanction; we want healthcare professionals to care for us well even when ‘no one else is looking’.
Leadership and management
Most of the papers in this review suggested that there was a need for good leadership if a culture of human rights was to be embedded in practice. 14,15,18,22,23 This involves leaders publicly promoting and displaying the core institutional values of the public service concerned. However, managers and leaders in public sector organisations are under pressure in an era of global market forces to act in ways that may not be consistent with these values. Where the manager or leader is also a healthcare professional, tension is also created between roles reflected in the concept of dual loyalty. 35 However, professional bodies and/or professionals, often in partnership with NGOs such as Human Rights Watch including Physicians for Human Rights, can role model advocacy of medical care 7,27 and provide support for cases of dual loyalty.
Limitations
Of the relatively small number of studies found which examined human rights education in health care, most were carried out in Great Britain and drew on a limited number of the same empirical studies. The evaluation reports included in this review were for the most part conducted independently by evaluators who were not involved in the provision of the human rights education programme concerned.
Conclusion
It is likely that human rights education in patient care meets neither of the concerns of healthcare professionals about applying human rights in practice. Human rights education need not be seen as being based on litigious threats. The content of much human rights education is embedded in existing statute and case law, national policies and guidelines and moral and professional norms which poses the question do we need human rights education? Despite the evident enthusiasm for and purported benefits of human rights education in patient care, the distinctiveness of human rights education interventions needs to be made more explicit in order to better identify their impact. It is part of critical reflective nursing 7 to examine this because human rights education has become such a prevalent global force and the claims that it can improve the provision of patient or person-centred care need to be rigorously examined before its wider adoption.