
Abstract
Background:
Nowadays, effective communication has become indispensable with the increasing prevalence of advanced life-limiting diseases. Goals of care discussion (GOCD) align care with patients’ preferences and improve care quality.
Objectives:
This paper probes deep into the dilemmas and summarizes strategies of medical staff conducting GOCD from the viewpoint of human-environment interaction.
Design:
Qualitative study comprising semi-structured in-depth interviews.
Methods:
Eighteen medical staff (6 doctors, 12 nurses) were recruited from five palliative care units in Guangzhou, China, from December 2023 to March 2024. Data were analyzed by carrying out Braun and Clarke’s thematic analysis and guided by Bourdieu’s theory of practice.
Results:
Three themes and 11 sub-themes emerged: (1) The palliative care environment as a complex and sensitive field characterized by highly sensitive life-related issues, intricate ethical dilemmas, and ambiguous role responsibilities; (2) Multiple forms of capital employed in communication, including informational capital, economic capital, social capital, symbolic capital, and emotional capital; (3) Common communication habitus, including risk aversion, euphemistic expression, emotional restraint.
Conclusion:
By drawing on Bourdieu’s theory of practice, this study offers revolutionary standpoints on the dilemmas in GOCD within palliative care, which underscores the significance of both individual and environmental factors. Grounded in these insights, we recommend implementing the following strategies: fostering a positive ethical climate and a conducive environment for open dialogue; enhancing ethical awareness and sensitivity through tailored training programs; clarifying relational frameworks to bolster team collaboration; improving communication approaches by leveraging diverse forms of capital; and proactively confronting implicit biases that persist in clinical settings.
Plain language summary
Life-limiting illnesses are rising globally. Effective clinician-patient communication, especially goals of care discussion (GOCD) is vital to match care with patient preferences. This study explores dilemmas and strategies for GOCD in China’s cultural context. It uses Bourdieu’s theory of practice to analyze how individuals interact with their environment. We used a qualitative design and interviewed 18 palliative care staff from five units in Guangzhou, selected purposefully. We analyzed the data thematically using Bourdieu’s framework. The study was approved by Guangzhou Medical University. Participants’ anonymity and voluntary involvement were ensured. Three themes emerged in sequence: First, palliative care is characterized as a complex, sensitive communicative field. Second, mobilizable capital (such as relational and cultural capital) is identified as influencing dialogue. Third, shared habitus, including risk aversion, euphemistic expression, emotional restraint, is shown to shape interactions. These themes collectively underscore how organizational ethical climates, individual ethical sensitivity, and capital integration enhance communication efficacy. This study shows that Bourdieu’s theory helps explain GOCD challenges. It suggests two intervention levels: improve organizational climates with both regulation and compassion, and train staff to boost ethical skills and use resources well. This can make communication more culturally sensitive and patient-centered in palliative care.
Introduction
Data from the Chinese Center for Disease Control and Prevention demonstrate a remarkable augment in total cancer-related deaths between 2005 and 2020. This rise notably exceeds the global average and that of high-income countries. 1 As roughly anticipated in relevant studies, the demand for palliative care by 2060 will increase by 87%. 2 Palliative care involves identifying and assessing terminally ill patients and their families. It provides comprehensive and multidimensional support for physiological, psychological, social, and spiritual needs. The research is predominantly intended to elevate the quality of life. Palliative care is a fundamental human right and should be part of people-centered and integrated healthcare services. 3 Effective palliative care requires patient-centered communication. 4 Effective communication permeates every stage of the palliative care journey, playing a pivotal role in accurately discerning and honoring the multifaceted needs and heartfelt desires of both patients and their families. It also supports the development of the most appropriate treatment and care plans.5,6 Goals of care discussion (GOCD) are a practical application of palliative care communication. These discussions allow clinicians to explain complex medical diagnoses and prognoses to patients and their families. GOCD is advantageous for relevant individuals to gather patient preferences, provide support, and facilitate joint decision-making. 7 They have the capacity to enhance patient receptivity, elevate the overall quality of life, diminish the frequency of intensive care unit admissions, facilitate the timely initiation of end-of-life care, and potentially prolong survival durations.8–10 Integrating GOCD into routine cancer care improves patient and caregiver experiences with healthcare, boosting satisfaction with care. 11 These discussions are also beneficial for clinicians to gather crucial information, clarify patients’ values, goals, and priorities, and support smoother decision-making. 12 Nonetheless, associated reports illustrate that fewer than one-third of patients with serious illnesses have discussed their care goals with healthcare providers. Most of these discussions take place late and infrequently during disease progression.7,11,13 In oncology, communication is particularly complex as a consequence of patients’ and families’ beliefs, expectations, emotional states, and difficulty understanding prognoses. These challenges hinder the start and continuation of GOCD.14,15 Hence, it becomes imperative to delve into the specific conundrums encountered and distill the efficacious strategies employed by healthcare professionals during GOCD, thereby fostering a more profound comprehension of GOCD’s applied merit within the realm of palliative care practice.
Current research on the challenges of these discussions typically fixes attention on dissimilar stakeholder perspectives.16,17 Nonetheless, communication is a bidirectional process. Relying only on subject-based factors and skill training is not enough to bring meaningful change in practice. A holistic approach is indispensable for supporting practice transformation. 18 Practical experience and the clinical environment collectively conduct paramount roles in facilitating effective communication. Understanding how environments impact discussions can offer new insights and solutions, benefiting all stakeholders through supportive communicative practices and shared experiences.19,20 Notwithstanding this, our existing knowledge regarding the nuances of individual experiences and the complexities inherent in clinical environments continues to be relatively circumscribed. There has been little investigation into how the interaction between individuals and their environment influences communication practices. 16 Manojlovich et al. 21 explored strategies to overcome barriers among medical staff by employing qualitative research focused on human–environment interaction. As demonstrated by relevant studies, addressing communication difficulties requires a comprehensive review of practices to understand the factors involved. From the human–environment perspective, examining communication can offer a valuable way to explore challenges and identify strategies.
Bourdieu’s theory of practice is a sociological framework that throws light upon how individuals correlate with their environment. To be specific, it analyzes practice by adopting the formula: “practice = [(habitus) × (capital)] + field.” In this model, individuals use various resources (capital) to develop strategies, which are then shaped and negotiated within a specific environment.22,23 Habitus refers to dispositions drawn from past personal or collective experiences, all shaped by history. Capital, by extension, embodies authority manifested through a spectrum of influential resources. These encompass economic, social, cultural, and symbolic assets, alongside individual competencies. Subsequently, the field can be conceptualized as a vibrant and ever-evolving milieu, comprising diverse forces within a specific domain. It functions as the principal stage where individual endeavors and interactions unfold.22,24,25 This theoretical framework is bound up with palliative care communication practices as it captures three essential characteristics: (1) multiple stakeholders (healthcare providers, patients, families) converge within the palliative care field; (2) dissimilar actors possess and utilize distinct forms of capital; and (3) each group operates according to specific habitus shaped by their professional training, personal experiences, and cultural backgrounds.
For this reason, this study applies Bourdieu’s theory of practice to delve into the practical challenges medical staff encounter when conducting GOCD. In particular, we frame the palliative care setting as a unique social field, delving into how healthcare practitioners’ approaches in GOCD are intricately molded by the dynamic interplay between their professional habitus—the ingrained dispositions, skills, and perspectives shaped by their career trajectory—and the multifaceted forms of capital they command and strategically utilize within this specialized arena. On that account, the study seeks to identify practical strategies to overcome these challenges.
Methods
Design
This qualitative study explored medical staff communication experiences and feelings through in-depth semi-structured interviews. Data underwent a thorough investigation with Braun and Clarke’s thematic analysis. Reporting follows the COREQ 32-item checklist 26 (see Appendix in Supplemental Files).
Guided by Bourdieu’s theory of practice, this study conceptualizes social action as the product of the interaction between field, capital, and habitus. The three constructs were systematically integrated into the research design, data collection, analysis, and interpretation as follows.22,23
(1) Field: Operationalized as the palliative care communication context, examining how this environment shapes and constrains practices. (2) Capital: Defined as resources used during GOCD, analyzing how forms of various capital are accessed, mobilized, and negotiated. (3) Habitus: Refers to clinicians’ ingrained dispositions toward sensitive conversations, investigating how these tendencies influence strategies.
Our thematic analysis was principally designed to identify patterns that correspond to the characteristics of the communication field, the types of capital circulating within it, and the shared habitus of the actors operating in this field.
Sampling and study settings
Purposive sampling was carried out to recruit the participants. This study was conducted in five palliative care units, including oncology wards and nursing homes, in Guangzhou between March and August 2024. Defined as the point when no additional issues are identified and the codebook begins to stabilize, the sample size was determined rooted in the principle of code saturation.27,28
Participants
Participants were selected in line with the following criteria: (1) possession of a valid physician’s or nurse’s license; (2) active engagement in oncology medical or nursing practice; (3) direct involvement in patient care in clinical settings; (4) experience conducting GOCD with patients and their families, including medical, nursing, or care planning; and (5) voluntary participation in the study. This study investigated 18 medical staff who have extensive experience in communication, including 6 doctors and 12 nurses. The sociodemographic data of the participants are shown in Table 1.
Participant demographic characteristics.

Data collection
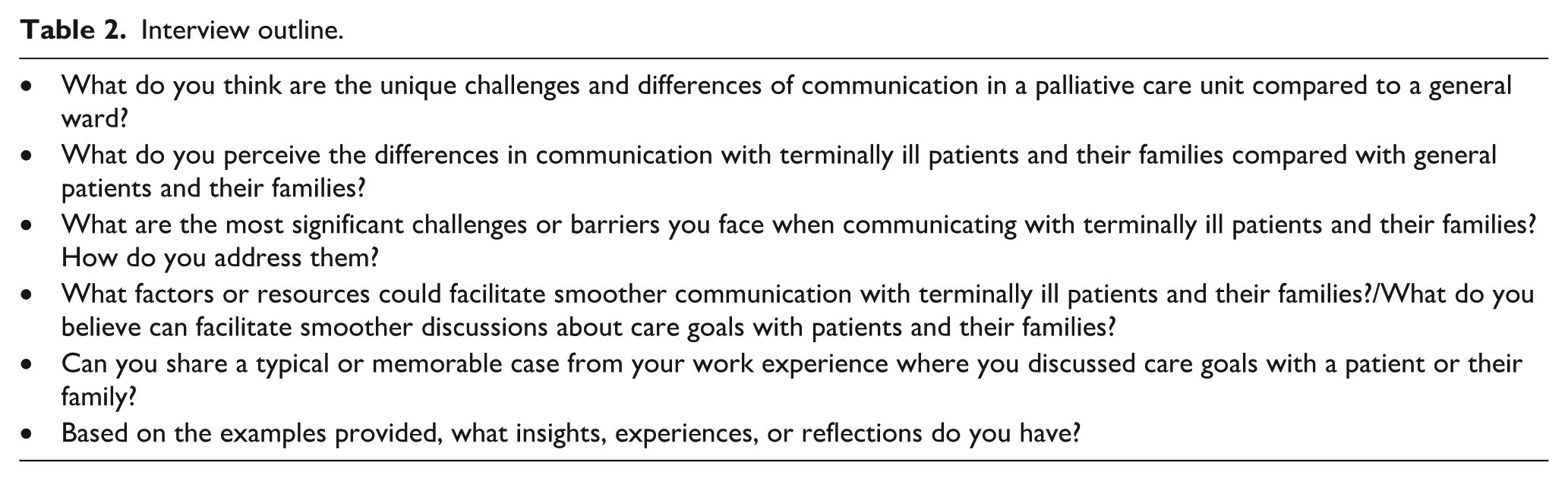
Each interview session lasted 30–45 min and was scheduled in accordance with participants’ preferences. Developed through literature review and group discussions, the interview guide was explicitly informed by Bourdieu’s theory of practice. The questions were designed to elicit information about participants’ experiences within the palliative care field, the resources (capital) they draw upon in GOCD, and their ingrained professional dispositions (habitus) that shape communication practices. Key interview questions are provided in Table 2. Two researchers conducted semi-structured, face-to-face, and in-depth interviews with respondents. Interviews were arranged beforehand and took place post-daily work in a tranquil, cozy room inside the department. Before the formal interview began, the researcher introduced himself, explained the purpose, content, and significance of the interview, and collected general information about the interviewee. The researcher ensured privacy by replacing names with serial numbers, explained the recording process, and obtained written consent. During the interview, one researcher led the conversation while the other recorded the session. The interviewer listened attentively, maintained a neutral attitude, and applied appropriate interview techniques. The recorder noted changes in the interviewee’s tone, demeanor, mood, and movements, documenting these as memos.
Interview outline.
Data analysis
Data analysis was supported by the software NVivo 14.0 and followed Braun and Clarke’s six-phases thematic analysis 29 : (1) familiarization with the data, (2) coding interesting features, (3) searching for potential themes, (4) reviewing themes, (5) defining and naming themes, and (6) drafting the preliminary paper.
Audio recordings were transcribed by a third-party service, with transcripts subsequently verified for accuracy by replaying the corresponding audio files. To guarantee a comprehensive analysis of the data, the transcripts underwent several rounds of review. H.L. independently coded the data using NVivo 14.0, adopting an inductive and iterative method rooted in Bourdieu’s theory of practice. Potential themes emerged through exploring similarities and relationships among codes, which were iteratively refined to accurately reflect participants’ perspectives.
The lead authors (H.L., S.T., Y.H., and H.D.) held regular debriefing sessions to align their understanding and deepen the interpretive process. Emerging findings were shared with the broader co-author team and participants. 30 In cases where coding agreement fell below 90%, two researchers (Y.L., Y.H.) reassessed the relevant segments. 31 This feedback mechanism bolstered data interaction and reinforced trust in the ultimate interpretations.
Data collection and analysis were conducted concurrently and iteratively, enabling constant comparison between new themes and existing categories. Data saturation was achieved when additional interviews yielded no new thematic insights. 31
Rigor
Rigor was maintained through credibility, reliability, and transferability.32,33
Prior to the interviews, researchers interacted with participants to establish rapport, creating an atmosphere conducive to candid conversation. During the study, researchers kept comprehensive analysis memos to record insights, guaranteeing clarity in the analytical approach. Trained extensively in qualitative research, all authors bolstered credibility by thoroughly reviewing interview transcripts. 29
Reliability was achieved by interviewing participants with diverse communication backgrounds and adhering strictly to data analysis protocols. Pre-interviews were conducted to refine the researchers’ skills in interview techniques, data collection for semi-structured in-depth interviews, and analysis methods. The semi-structured interview guide was iteratively refined with expert input to ensure validity.
Transferability was enhanced by offering an all-round description of the study findings, enabling replication in similar palliative care contexts. This detailed documentation supports the applicability of the results to other settings.
Ethical considerations
Approved by the Institutional Review Board of Guangzhou Medical University (Reference number 202312003), all participants provided written informed consent prior to participation. The lead researcher notified the Nursing Department Chair and secured written approval from all participants. To ensure confidentiality, participants were assigned unique identifiers, and their responses were anonymized to prevent linkage to individuals. The research team treated all participants with respect, valuing their opinions and ensuring their right to withdraw from interviews if they felt uncomfortable.
Results
The following results are systematically organized around the three core constructs of Bourdieu’s theory of practice, revealing the characteristics of the palliative care communication field, the types of capital circulating within it, and the habitus manifested by healthcare practitioners. Table 3 displayed detailed themes, subthemes, and corresponding strategies.
The theme, subtheme, and strategy of GOCD based on Bourdieu’s theory of practice.

Palliative care is a complex and sensitive communication field
Life-related issues are highly sensitive
Patients are highly sensitive at the end of life and topics related to end-of-life management. When communicating with patients about life issues, medical staff often find themselves in a dilemma, experiencing a significant psychological burden characterized by concerns and worries. They often hope to engage in profound exchanges with patients to understand their inner world but worry that their words and actions might trigger negative emotions. P3: “I really want to ask patients these (end-of-life) questions, but I’m afraid it may impact them negatively, possibly leading them to spend their last days in sadness.” N12: “I’m quite scared to communicate with them because they are also quite sensitive, sometimes afraid of saying something wrong.”
Multiple ethical issues are intricately interwoven
In particular, numerous ethical conflicts arise when conversing with terminally ill patients and their families. Interviewees pointed out that medical staff feel conflicted, needing to repeatedly weigh the pain they cause against their potential benefits. P2: “What he (the family member) demands is for me to do nothing, just not let him die at home. . . His goal contradicts our usual professional requirements and medical ethics.” N4: “In communication and decision-making, we must adhere to both legal and emotional considerations.”
Ambiguity in roles and responsibilities
Notwithstanding the fact that medical staff must adhere to professional boundaries, they normally have to undertake tasks beyond their duties on account of clinical circumstances. As these tasks do not fall within the traditional scope of medical and nursing duties, and they frequently place medical staff in difficult situations, this is especially applicable when dealing with more personal issues like resolving internal family conflicts among patients. N4: “Although some family psychosocial work might exceed the scope of doctors and nurses, considering operational issues, these tasks still have to be shared by doctors and nurses.” N1: “It’s actually quite hard to mediate because some involve family conflicts, and then we are only responsible for medical care, it’s not appropriate for us to interfere with their family’s internal conflicts.”
Communication capital available for use
Informational capital: The navigator of decision-making
Medical staff possess a power of medical information, including diagnostic results, treatment plans, and prognosis, which when conveyed to patients and their families can facilitate smoother communication. P1: “From a medical perspective, there are some misunderstandings, like whether getting excessive injections is harmful or if taking painkillers brings about addiction. These are misconceptions about medical treatment and medication that can be clarified.” N8: “Some family members tend to be self-centered. . .we need to explain our intentions clearly, which helps improve communication.”
As noted by some interviewees, effective communication and decision-making require medical staff to have a comprehensive understanding of the patient and their family, gathering information from multiple sources (patients, family members, caregivers, etc.) and across various aspects, including personal, familial, psychological, and social dimensions. N2: “It is essential for us to grasp some personal and family situations of the patients, communicate with them and family members, and even understand from nursing assistants.” N8: “It’s not just about revolving around the disease itself but also about the overall condition of the patient, family situation, and psychosocial factors to provide more integrated care.”
Economic capital: The foundation of decision-making
Economic factors conduct a principal role in medical decision-making. As the primary payers for medical care, family members are the main holders of economic capital and significant negotiators in communication. Their agreement is vital for implementing decisions and is an essential target in decision-making communication. N8: “In the later stages, certain nutritional support is also necessary, but some family members might possibly consider it from an economic perspective and reject it. . .In this situation, we do not have any effective measure.” N1: “Many family members are primarily concerned about the economic aspect, what benefits they can gain, and how it can alleviate their burdens.”
Social capital: The collaborative network in decision-making
Teamwork constitutes the most prevalent form of social capital among medical staff. In terms of internal collaboration, interviewees noted frequent information flow and mutual cooperation and support networks from junior nurses to senior nurses, head nurses, and attending physicians. N12: “If any information is obtained, it is generally passed on to the senior nurses or the head nurse, and then to the attending physician.” N1: “Whenever I encounter something I cannot handle or have not encountered before, I definitely need to consult with senior nurses and the supervising doctor.”
External collaboration mainly manifests in interdisciplinary cooperation. When patients encounter psychological or social challenges, medical personnel can coordinate interventions with other specialists, like nursing aides and social workers, ensuring a collaborative effort in patient care and support. N2: “If we really notice any psychological issues, we will also ask social workers to follow up and pay more attention to the patient’s psychological dynamics.” P3: “The influence of nursing assistants on them may sometimes be deeper than that of their family members in the later stages. Having nursing assistants show more care and talk with them is also very important for solving their psychological problems.”
Symbolic capital: The adhesive in decision-making
In front of patients and their families, medical staff can establish a professional and authoritative image by demonstrating professional knowledge and skills. This image enhances the trust of patients and their families in medical staff, playing a significant role in promoting effective communication and decision-making. N8: “By showing our professionalism, they will trust us greatly, which makes many subsequent matters considerably easier to handle.” N10: “It’s pivotal to let them know you are using your competence (to help them) and can solve practical problems; this is a tremendously significant factor in facilitating communication.”
Emotional capital: The driving force in decision-making
Medical personnel can engage with patients and their families through various means, such as organizing family conferences, attentively addressing their needs and worries, and offering unwavering emotional backing. This interaction strengthens the trust relationship between both parties and promotes more effective communication and cooperation. N8: “His daughter actually needed someone to talk to emotionally; every time she came, we would sit on the sofa outside and listen to her talk about her recent life situation and what help she needed, which made her more proactive in contacting us.” N10: “I concentrated on the emotions of the family members; she was quite anxious. . . We held a family meeting for them, and many emotions that might not have been expressed in front of the patient were actually vented during the meeting.”
Common habitus of communication
Risk aversion
In handling medical care decisions, medical staff members place remarkable emphasis on avoiding potential disputes over decisions and maintaining conspicuous self-protection awareness. This risk-averse habit is manifested in communication practices through cautious actions, an emphasis on detailed assessments, and the search for responsible parties or guarantors for decisions. This disposition can be understood as a product of a defensive medical culture and past negative experiences, which collectively shape a cautious habitus. P5: “After all, if these final medical decisions are not handled well, they could lead to considerable safety risks later on.” P4: “When facing something dispute, protecting ourselves is also very important.” This widespread tendency to avoid risks seems to originate from the palliative care field’s profound ethical sensitivity, along with possible doctor-patient tensions, and further mirrors a pronounced sense of self-preservation among Chinese healthcare professionals, given that medical disputes can frequently lead to substantial career repercussions.
Euphemistic expression
When dealing with sensitive topics such as death, medical staff tend to express themselves more euphemistically to avoid causing discomfort or touching on taboo subjects for patients and their families, which primarily centered around discussing the topic just enough to convey the main points. This habitus of indirect communication is a practical adaptation to the powerful doxa (taken-for-granted beliefs) within the Chinese socio-cultural field, which often forbids direct talk about death and dying, viewing it as inauspicious or uncomfortable. N6: “Sometimes I dare not say too much because many of them are actually quite superstitious about death; you can’t be too direct with them, nor delve too deeply. I just bring up the main points briefly, to the point where they can understand the meaning.” N7: “If said directly, might make everyone feel somewhat uncomfortable.” This pattern of euphemistic a multitude of questions about palliative care expression represents a habitus shaped by cultural norms within the Chinese healthcare field, where direct discussion of death is often considered inappropriate, combined with the need to maintain harmonious relationships with patients and families in the emotionally charged palliative care environment.
Emotional restraint
On an emotional level, healthcare professionals often maintain a certain emotional distance from patients and their families, fearing that excessive empathy could result in emotional fluctuations or moral dilemmas for themselves. This habitus of emotional restraint is shaped by professional norms that prioritize clinical objectivity and self-protection against burnout, which sufficiently demonstrates how the field of medical practice disciplines emotional responses. N6: “I dare not delve too deeply because sometimes I feel like I might empathize too much, and I fear that talking more would make me cry.” N3: “I dare not advise too much; saying more feels like there’s a sense of unfilial psychological suppression weighing on my heart.” N2: “As a woman and a mother myself, I can empathize with her, but when conversing, I dare not empathize too much.” The tendency of healthcare professionals to maintain emotional distance from patients is nothing more than a personal choice. On the contrary, it also represents a habitus shaped by the professional medical field’s long-standing emphasis on “rationality” and “objectivity” in clinical practice. This emotional restraint serves as a coping mechanism to prevent burnout and avoid the moral dilemmas that can arise from over-identification with patients’ suffering in the demanding palliative care environment.
Discussion
Creating a positive organizational ethical climate and enhancing individual ethical literacy
As evidenced by the above research, palliative care settings frequently present complex and sensitive ethical dilemmas. These ethical dilemmas often stem from various aspects, including the legal complexities of end-of-life care, advance care planning, the inappropriate application of medical interventions, and symptom-specific concerns, among others. 34 Rosa et al. 35 emphasize the importance of recognizing and communicating ethical requirements. As already suggested by certain studies, the communication ability and humanistic care are correlated with the organizational ethical climate, which plays a mediating role when individuals face dilemmas and indirectly affects individual behavior. 36 As members both shape and are influenced by their organization’s climate, the field of palliative care serves as the practical context in which these factors interact.23,24,37 There is evidence that the ethical climate affects decision-making and behavior when facing ethical dilemmas. 38 A positive ethical climate is a positive predictor of professional competence and can reduce medical errors, while a negative ethical climate increases the possibility that the care provided does not meet the wishes of patients and their families, thereby reducing the quality of care.34,39,40 As relevant studies suggest, bolstering hospital resource allocation to bolster nurses’ ethical decision-making capabilities can motivate nurses to fully leverage their moral autonomy.41,42 As a consequence, robust organizational ethical climate in hospitals is essential for enhancing nurses’ goal communication, safety, and professional growth, which necessitates both educational reforms and leadership-driven strategies. To be more specific, Aloustani’s et al. 43 study advocates incorporating ethical leadership and dilemma management into nursing curricula to equip students for future challenges. Similarly, Goldman and Tabak’s 36 highlights the chief nurse’s critical role in fostering an ethical workplace by implementing cohesive strategies that promote teamwork and address staff needs, thereby building a robust ethical foundation. More importantly, hospitals can create supportive environments that enhance nurses’ confidence, job satisfaction, and patient care quality, which can be materialized by embedding ethical leadership in education and empowering chief nurses to drive cohesive, team-oriented strategies.
On top of that, it has been validated that ethical sensitivity is strongly positively correlated with caring efficacy and conducts a partial mediating role in how an ethical climate correlates with caring efficacy (accounting for 50% of the total efficacy). 40 Caring practices begin with an awareness of patients’ suffering and vulnerability, namely, ethical sensitivity. 44 It is particularly noteworthy that ethical sensitivity is crucial for clinical decision-making and delivering high-quality care. GOCD is chiefly designed to identify and address patients’ needs, ensuring care aligns with their values. Both ethical sensitivity and GOCD share this objective and mutually reinforce each other in practice.15,45 By fostering empathy and enabling medical staff, favorable ethical sensitivity enhances communication among patients to better understand complex issues, identify patient concerns, and incorporate their values, preferences, and goals into care decisions.46,47 In family interactions, particularly in the current era where there is an increasing emphasis on family-centered end-of-life care, higher ethical sensitivity improves relationship management through effective communication.46,48 Apart from that, ethical sensitivity correlates positively with job embeddedness and satisfaction. Notably, significant ethical sensitivity enables staff to adeptly address ethical challenges, make informed nursing decisions, and gain a sense of professional fulfillment, which demonstrates enormous potential to reinforce job identity. 45 In stark contrast, mishandling ethical issues can bring hesitation and apprehension, causing job burnout.46,49–51 As a result, targeted training in ethical knowledge and skills should be conducted in accordance with the characteristics of ethical issues in the field of palliative care, to strengthen ethical literacy and promote the transformation of habits of implicit expression. For instance, through engaging in in-service training programs that integrate interactive workshops and ethical symposia, nurses can significantly deepen their comprehension of hospital-specific ethical guidelines and fortify their perception of a salubrious ethical milieu within the workplace. 52
Clarifying the relationship structure and boosting team collaboration
Our research underscores the ambiguity in the roles and responsibilities of healthcare providers during communication processes, which can bring about communication breakdowns, exacerbating issues such as ineffective interactions, disordered protocols, and reduced satisfaction among patients and families. 53 In the communication process, the ambiguity and conflict of role not only exert a disadvantageous influence on the doctor–patient relationship but may also affect the decision-making process.34,36 Typically, physicians lead GOCD and rarely involve nurses in delivering bad news, particularly in final decisions involving life-sustaining technologies. 14 Nevertheless, as the healthcare professionals with the closest patient contact, patients and their families normally turn to nurses as a primary and trusted source for therapeutic and care-related information.12,54 Although nurses frequently feel capable and willing to initiate such discussions and provide decision-making guidance, they often lack authority, autonomy, or sufficient institutional support within hospital ward cultures to address cancer-related topics like diagnosis or prognosis.54,55 Consequently, nurses might shun discussions, often perceiving challenging topics as beyond their purview and refraining from divulging health-related details owing to ambiguities in care strategies. 14 Role clarity is vital for effective GOCD and decision-making, involving expanding nursing roles, clearly designating responsible healthcare providers, and coordinating service delivery. 56 As evidently suggested in studies carried out by Peereboom and Coyle 12 and Baer and Weinstein, 14 when oncology nurses possess strong communication skills and lead the GOCD, they play a pivotal role in adhering to care plans, enhancing patient and family satisfaction, and overall clinical outcomes. By strengthening the role of nurses and fostering skilled, it can better align care delivery with patient needs.
Aside from that, strengthening team cohesion and breaking down rigid role boundaries serve as a paramount factor for delivering consistent and patient-focused care. 57 Limiting simulation training to only physicians or advanced practice nurses may miss opportunities for broader team collaboration. 58 Multidisciplinary teams equipped with relevant training, skills, and resources can better deliver appropriate and goal-oriented care to patients. 59 Fostering dialogues and sharing insights on communication tactics among team members significantly boosts coordination efficacy and the refinement of care planning processes. 56 Coordinated palliative care teams enhance GOCD by fostering team alignment with mutual support, ensuring consistent messaging to patients and families, aligning services to meet patient goals, empowering patients to focus on living with greater control over their end-of-life processes.56,58,60 To be specific, a 3-month inter-professional training program enhanced participants’ cross-professional collaboration in complex goals of care dialogues by reinforcing individual roles and acknowledging the contributions of other professionals. 61 Likewise, the Team-Based Serious Illness Care Program has been proven to efficiently distribute workload burdens, schedule discussions on the basis of patient needs, highlight the unique value of non-physician team members, and foster team coordination. 53 Such interventions underline the significance of dissimilar roles and team-based models in optimizing communication and care delivery for patients with life-limiting illnesses.
Optimizing communication strategies and enhancing capital integration
As evidently demonstrated by our research findings, the main capital in communication can be mobilized, including economic, informational, social, symbolic, and emotional capital. In accordance with Bourdieu’s theory of practice, capital is a tool of practice.23,24 Temporal and spatial resources are indispensable for us to conduct relevant dialogues required, which constitute pivotal parts facilitating the improvement with regard to the effectiveness of guiding GOCD among medical staff.19,62 If available capital is limited, it will damage the development of relevant dialogues and mass communication opportunities, thereby elevating the potential risk of medical care that does not match patients’ values and goals.19,63,64
In economic capital, evidence suggests that communication about finances is an important aspect of decision of cancer treatment. 65 The communication attribute of cost-related health literacy refers to the ability of cancer patients to communicate effectively with the medical care team. It can not only better patients’ and families’ understanding and awareness of treatment costs, but also facilitate shared decision-making on the basis of informed consent, while a deficiency of this literacy can lower confidence and comfort in communication and increase the occurrence of financial toxicity.66,67 Under such circumstances, improving patient and family cost-related health literacy is also a paramount approach to mobilizing and integrating economic capital to quicken the development of communication.68,69 Information is the basis for making high-quality decisions aligned with patient values and needs. Meaningful dialogue is essential to foster profound mutual comprehension and strengthen interpersonal rapport.11,60 Hence, it is crucial to open communication channels, effectively absorb, and transmit informational capital.7,70 With reference to social capital, palliative care not only involves physical, psychological, social, and spiritual aspects, but also requires a multidisciplinary team framework. 3 As revealed in a qualitative study carried out by Gradwohl et al., 71 severe illness care projects on the basis of teams have unique advantages in integrating dissimilar perspectives, knowledge, and abilities of professional and non-professional team members. Collaboration among team members can invite more favorable outcomes for complex issues. More importantly, it can function as a remarkable facilitator for goal-concordant care. 58 The team should coordinate and integrate professional and non-professional team members, promote knowledge sharing and effective collaboration, and integrate social capital.
Professionalism is an important factor affecting communication dialogues and is a crucial aspect of enhancing and advancing communication. 12 The archetype of a compassionate and erudite physician exerts a compelling allure, fostering trust with patients and families alike and constituting a pivotal element of informal communication dynamics.12,18 Medical staff should reasonably present symbolic capital and make the medical side approachable while reinforcing the professional image. From emotion, goal communication content is filled with emotional stress from making difficult decisions, entailing frequent involvement with emotional issues.19,56 When patients’ emotions were effectively handled, they can develop a more profound comprehension of disease and prognosis with less suffering, benefiting the progress of communication and improving satisfaction. 72 As a result, the emotional response knowledge and experience can be enriched by periodically conducting communication case discussion meetings and experiencing sharing sessions, 16 and promote medical staff shift from emotional restraint habits to emotional exploration and enhance the ability to use emotional capital.
Specific tools, such as the NURSE framework, Ask-Tell-Ask, Tell Me More, and Situation-Background-Assessment-Recommendation (SBAR), are effective in deploying these capitals, enhancing emotional responses, information sharing, and collaboration. 73 Training in these tools is recommended to optimize communication outcomes.
Damming the doxic undercurrent in the communication
As our findings reveal, palliative care communication is permeated by a powerful doxa—risk aversion, implicit expression, and emotional restraint. The unspoken and taken-for-granted beliefs regarding death, dying, and familial responsibilities as noted by Sudhakar et al. 74 This aligns with studies by Ibrahim and Harhara,75,76 which evidence that public discussions of death may be seen as disrespectful on account of cultural and religious sensitivities, leading doctors to avoid openly sharing prognoses for advanced diseases with patients. This doxa encompasses cultural taboos and norms, such as avoiding direct talk about death and upholding filial piety, acting as an invisible yet influential undercurrent that shapes interactions.77,78 For instance, Western societies place emphasis on individualism and the inviolability of private property, giving rise to medical ethics that prioritize patient autonomy. 79 In contrast, Eastern cultures often adopt family-centered and collectivist perspectives, where strict truth-telling and individual autonomy can be viewed as burdensome or isolating for dying patients.77,80 These disparities underscore the imperative for a more nuanced investigation into the ways cultural variables shape communicative behaviors.
Furthermore, characterized by euphemistic language and emotional restraint, the habitus of healthcare professionals represents a practical adaptation to this doxic framework. By communicating indirectly and suppressing their emotions, clinicians navigate unspoken rules to prevent violating core cultural beliefs and sparking conflicts. Empirical evidence corroborates this, revealing that a majority of healthcare professionals perceive non-disclosure of diagnostic details—especially regarding suspected or confirmed malignancies—as standard practice rather than an anomaly. 76 To address this, effective communication training and interventions must extend beyond mere skill-building to incorporate critical reflection on these doxic structures. Raising these tacit beliefs to conscious awareness is an essential first step in challenging them and fostering a more open communication environment.
Notwithstanding the aforementioned contributions, this study has several limitations deserving further investigation in the future. First and foremost, while our interview protocol was theoretically informed, it may not have sufficiently explored the deep historical and cultural factors shaping professional habitus. A more narrative interview guide would have helped participants to narrate concrete situations in detail—describing what they did in a specific interaction, why they chose that strategy, and how other actors (e.g., patients, family members) influenced the process. This would have provided richer data to explicate the dynamic interplay. On top of that, our analysis failed to cover the complex power dynamics between physicians, nurses, patients, and family members within the communication field. Moreover, the study was conducted solely in China, which may limit transferability to other contexts. On that account, it is critical for researchers to employ interview techniques specifically designed to explore practitioners’ motivations and historical formation of dispositions, incorporate multiple stakeholder perspectives (including patients and families), and examine communication practices across diverse cultural and healthcare settings to a more comprehensive understanding of the palliative care communication field.
Conclusion
This marks the inaugural application of Bourdieu’s theory of practice to examine ethical dilemmas within GOCD in palliative care contexts. As our research findings reveal, palliative care is a complex, sensitive, and ambiguous communication field. The main behavioral habits formed are risk aversion, implicit expression, and emotional restraint. It is particularly noteworthy that the most common capitals are economic, information, social, symbolic, and emotional capital. To solve the communication dilemma, we should create a positive organizational ethical climate, continuously improve the ethical sensitivity, delineate relational structures to enhance team collaboration, and improve the ability to integrate and mobilize diverse resources. Aside from that, it is also imperative to facilitate the negative habits into more open, exploratory, and collaborative habits.
Supplemental Material
sj-docx-1-pcr-10.1177_26323524251400803 – Supplemental material for Navigating goals of care discussion in palliative care: A qualitative study applying Bourdieu’s theory of practice
Supplemental material, sj-docx-1-pcr-10.1177_26323524251400803 for Navigating goals of care discussion in palliative care: A qualitative study applying Bourdieu’s theory of practice by Haiyang Lin, Shiyong Tan, Yufei Huang, Haojie Duan, Yumei Li and Yanping Hao in Palliative Care and Social Practice
Footnotes
Acknowledgements
We are grateful to physicians and nurses in Guangzhou for their willingness to participate in the study. In addition, we sincerely thank Guang Shi, Shengdi Chen, and Jinyu Chen for their invaluable contributions during the revision stage of this paper. Under their expert guidance and support, the quality of the manuscript has been significantly enhanced.
Ethical considerations
This study was approved before data collection by the Institutional Review Board of Guangzhou Medical University (Approval number 202312003). All procedures performed in studies involving human participants were in accordance with the ethical standards.
Consent to participate
The primary investigator also obtained written approval for all participants. The data from respondents were treated with confidentiality at all times. The research team treated respondents with respect, particularly by valuing their opinions, honoring their right to end an interview if they felt uncomfortable, and using careful questioning techniques, particularly when addressing deeply personal or sensitive topics. The purpose and methodology of the study were explained to the participants to seek their informed consent before participation in the study.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Guangzhou Municipal Health Commission’s Research Project on the Construction of Palliative Care System in Guangzhou (J2427X002).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sources are not publicly available due to privacy and ethical restrictions. However, it can be accessed upon request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.