
Abstract
Background
Low-dose computed tomography screening reduces lung cancer-specific mortality in high-risk individuals. Lung cancer risk factors overlap with comorbid diseases, highlighting the significance of frailty and comorbidities for lung cancer screening (LCS). Here, we describe the prevalence of frailty and comorbidity in those invited for LCS and evaluate their associations with response to telephone risk assessment invitation and subsequent uptake of LCS.
Methods
Analysis was based on the intervention arm of the Yorkshire Lung Screening Trial, where ever-smoked individuals aged 55–80 were invited to telephone risk assessment followed by community-based LCS if at higher risk. The electronic frailty index (eFI) was used to compute individual frailty scores (categorised as fit, mild, moderate and severe) and derive comorbidity data.
Results
Of 27,761 individuals invited, 24.1% (n = 6702), 8.5% (n = 2353) and 1.7% (n = 459) had mild, moderate and severe frailty, respectively. Over half responded to the invitation to telephone risk assessment (n = 14,523, 52.5%) with frailty associated with a higher response rate compared to fit individuals: adjusted odds ratio (ORadj) 1.34, 95% confidence interval (CI) 1.26–1.42 for mild frailty; ORadj 1.28, 95%CI 1.16–1.40 for moderate frailty; and ORadj 1.32, 95%CI 1.08–1.61 for severe frailty. Similar patterns were seen with comorbidity counts. After assessment, moderate (ORadj 0.75, 95%CI 0.59–0.96) and severe (ORadj 0.67, 95%CI 0.43–1.04) frailty were associated with reduced screening uptake.
Conclusion
The presence of frailty was associated with increased response to LCS invitation. Given the strong association between frailty and reduced life expectancy, these results suggest that people with potentially more life years to be gained from LCS may be less inclined to take part. Further research is needed to explore the interactions between frailty and LCS decision-making to inform future invitation strategies.
Introduction
Lung cancer is the leading cause of cancer-specific mortality in the UK 1 and globally, 2 with low survival rates reflecting the fact that most patients presenting symptomatically have late-stage disease at diagnosis, which is less responsive to treatment. Early diagnosis of lung cancer significantly improves survival rates, hence the importance of screening for early detection, especially in high-risk groups. The National Lung Screening Trial (NLST) in the US and the Nederlands–Leuvens Longkanker Screenings Onderzoek (NELSON) in Europe have shown that lung cancer screening (LCS) with low-dose computed tomography (LDCT) reduces lung cancer mortality by 20% and 24% respectively.3,4 In the UK, following the recommendation from the National Screening Committee, the UK government announced in June 2023 the rollout of targeted LCS for individuals between the ages of 55 and 74 who were recognised as having a higher risk of developing lung cancer, largely based on smoking history. 5
However, in individuals with significant frailty or comorbidities, competing causes of death may limit the life years gained by LCS, and this may be more apparent in real-world studies compared to that observed in the original randomised trials due to the healthy volunteer effect. Data on smoking history and frailty are potentially available from General Practice (GP) electronic patient records. Frailty is defined as the loss of biological reserves across several organ systems and vulnerability to physiological decompensation following a stressor event. 6 There is relatively little published research assessing frailty in the context of LCS. 7 Most LCS guidelines highlight the need to assess candidates’ fitness and ability to tolerate screening and subsequent curative treatment. 7 Yet, the ability of LCS programs to identify and exclude candidates who might not benefit from screening is still a challenging area that needs further research, as recognised by the American Thoracic Society. 8 Given the relationship of frailty and comorbidity with adverse outcomes in patients with lung cancer,8–10 it is critical to establish the prevalence of frailty and comorbidity among potential screenees and examine their association with LCS invitation response, uptake and outcomes from screening.
The objective of this study was to describe the prevalence of frailty and comorbidities in a subcohort of the population invited for LCS as part of the Yorkshire Lung Screening Trial (YLST), as well as examine the associations of frailty and comorbidity with response to invitation for telephone lung cancer risk assessment and uptake of LDCT screening amongst those people found to be eligible (framed as part of a lung health check (LHC)).
Methods
We conducted a retrospective case-control analysis using data extracted from the intervention arm of the ongoing YLST, where frailty was the primary exposure of interest and case-control status was defined by response/non-response to an invitation to telephone-based lung cancer risk assessment to determine eligibility for LDCT screening. In addition, screening uptake was defined based on the attendance at a mobile CT scanning unit for those people found to be eligible for screening based on any one of three criteria (the USPSTF2013 criteria, a PLCOM2012 risk of ≥1.51% over six years, or an LLPv2 risk of ≥5% over five years). Details of the YLST design and participation in the baseline screening round have been published previously.11,12 Briefly, the YLST is a randomised controlled trial evaluating invitations to community-based LHCs (involving LDCT screening) for people aged 55–80 years with a GP record indicating a smoking history. The trial is being conducted in Leeds, UK and includes a usual care (no invitation) comparison group.
For this study, 66 participating practices that used The Phoenix Partnership (TPP) SystmOne 13 electronic patient records were approached for permission to extract additional participant information. Participant data were extracted under a Section 251 amendment approved by the Health Research Authority Confidentiality Advisory Group (further details below). Frailty was investigated using the electronic Frailty Index eFI, 14 which can be applied to electronic GP records through an algorithm that uses READ/Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) codes. The eFI consists of 36 equally weighted deficits with no time constraints to individual deficits except for polypharmacy. Frailty was investigated by categorising the frailty scores into a 4-level variable (fit, mild, moderate, severe) according to pre-defined cut-offs (0–0.12 was defined as fit; >0.12–0.24 as mild frailty; >0.24–0.36 as moderate frailty and >0.36 as severe frailty). 14 YLST included a coded diagnosis of severe frailty in the electronic GP record as an exclusion criterion. GP electronic health records are configured to automatically calculate the eFI, 15 but frailty codes are only added to the patient record following clinical review and confirmation. Thus, people with sufficient deficits to be categorised as having severe frailty, but in whom this had not been clinically verified, were invited for screening and are included in the analysis presented here.
In addition, 12 physical health comorbidities were selected for analysis including cancer, stroke, chronic obstructive pulmonary disease (COPD), heart failure, peripheral vascular disease (PVD), inflammatory arthritis, liver problems, mono/hemiparesis, peptic ulcer disease (PUD), chronic kidney disease (CKD), diabetes and ischaemic heart disease (IHD). These comorbidities were selected based on their inclusion in the Charlson Comorbidity Index (CCI) 16 and were analysed separately from the eFI. Polypharmacy is one of the eFI deficits, defined originally based on the presence of ≥5 prescribed medications, using chapters 1–15 of the British National Formulary. Unfortunately, it was not possible to extract comprehensive medication data to calculate the polypharmacy deficit for all included participants. Therefore, for each frailty category, the presence/absence of polypharmacy for participants was inferred using the observed frailty-specific prevalence of polypharmacy in the eFI development cohort used by the eFI authors. 14 We conducted several sensitivity analyses that examined the effect of using different polypharmacy prevalences on calculating eFI scores. An Excel file containing all eFI SNOMED CT codes was provided by the eFI development team and uploaded to TPP SystmOne by the NHS West Yorkshire Integrated Care Board (ICB) Office of Data Analytics team. Data for all participants were extracted between August 2022 and February 2023, and all analyses were conducted using SNOMED CT codes entered into the GP record up to the date of randomisation. Ethnicity and smoking status were derived by the YLST statisticians using general practice codes for all invitees, as reported previously. 12 YLST invited participants aged up to 80 at the time of data extraction from primary care records, whereas the current NHS England Targeted Lung Health Check programme only includes participants up to 74 years. Frailty descriptors and comorbidity counts are therefore shown for participants aged <75 and ≥75 years.
The univariable relationships between response to invitation (telephone assessment), attendance and baseline factors, including frailty and comorbidities, were investigated using logistic regression. Multivariable logistic regression was used to investigate the relationship between response to telephone eligibility assessment and the exposure of interest, adjusting for factors previously identified as significantly associated with response (including age, Index of Multiple Deprivation (IMD) quintile, smoking status, sex and ethnicity). 12 These analyses were conducted for exposures of interest, including eFI and physical health comorbidities. The analyses were repeated for attendance status in those eligible and invited to the LHC. Odds ratios (ORs) are presented with 95% confidence intervals (CIs), and statistical tests were two-sided. Analyses were conducted using Stata version 17.0 (StataCorp, CollegeStation, TX, USA).
The Health Research Authority approved the YLST following a review by the Research Advisory Group (18/NW/0012) and the Confidentiality Advisory Group (18/CAG/0038). The approval covers using eFI to explore the link between frailty/comorbidity and response to the invitation for an eligibility check and LHC screening attendance.
Results
Among all individuals randomised to the intervention arm of the YLST (n = 44,943), we accessed 27,761 participants’ records (61.8%) from 54 general practices in Leeds; 12 practices did not respond to requests for data access, and an additional 18 practices used a different software system (EMIS) from which we were unable to access data. A comparison of demographic and clinical characteristics according to whether people responded to a written invitation for telephone risk assessment is shown in Table 1. Baseline demographics in the frailty/comorbidity subcohort (shown in Table 1) were comparable to those reported in the YLST intervention arm, 12 indicating that the data presented here are representative of the YLST intervention cohort. Overall, the mean age of people invited for a risk assessment was 66, 14.4% were ≥75 years, 52.2% were male, and 29.3% resided in areas associated with the most deprived IMD quintile. Based on primary care record codes, 30.3% of the cohort were currently smoking, and 68.5% had previously smoked but now quit. The prevalence of individual deficits that make up the eFI is presented in supplementary data (Table S1). In line with the findings observed during the development of the eFI, 14 we found an inverse correlation between the eFI and IMD – i.e. people from more deprived populations were more frail (Supplementary data, Figure S1). The eFI identified 24.1% of participants as having mild frailty, 8.5% with moderate frailty and 1.7% with severe frailty. Of the selected 12 comorbidities, 46.4% of participants had zero comorbidities, 26.2% had one comorbidity, 14.1% had two comorbidities, 7.5% had three comorbidities and 5.8% had four or more comorbidities. Invitees aged ≥75 years had higher levels of frailty and comorbidity (Figure 1).
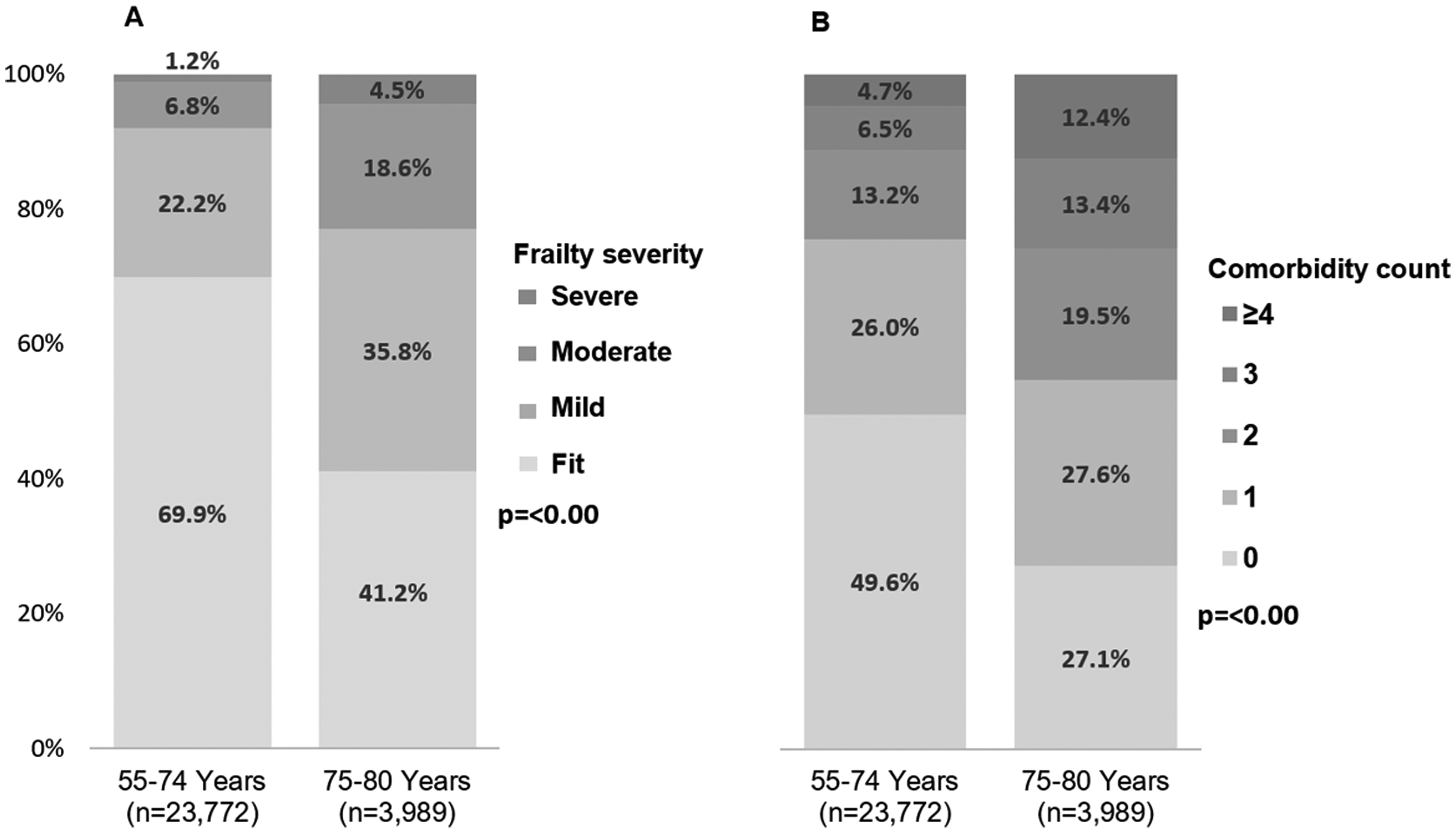
Distribution of frailty severity (A) and comorbidity count (B) by age group based on the current LCS UK recommendation cut-off age of 74 years in those invited to telephone risk assessment.
Baseline factors by the response to the invitation to telephone eligibility assessment.
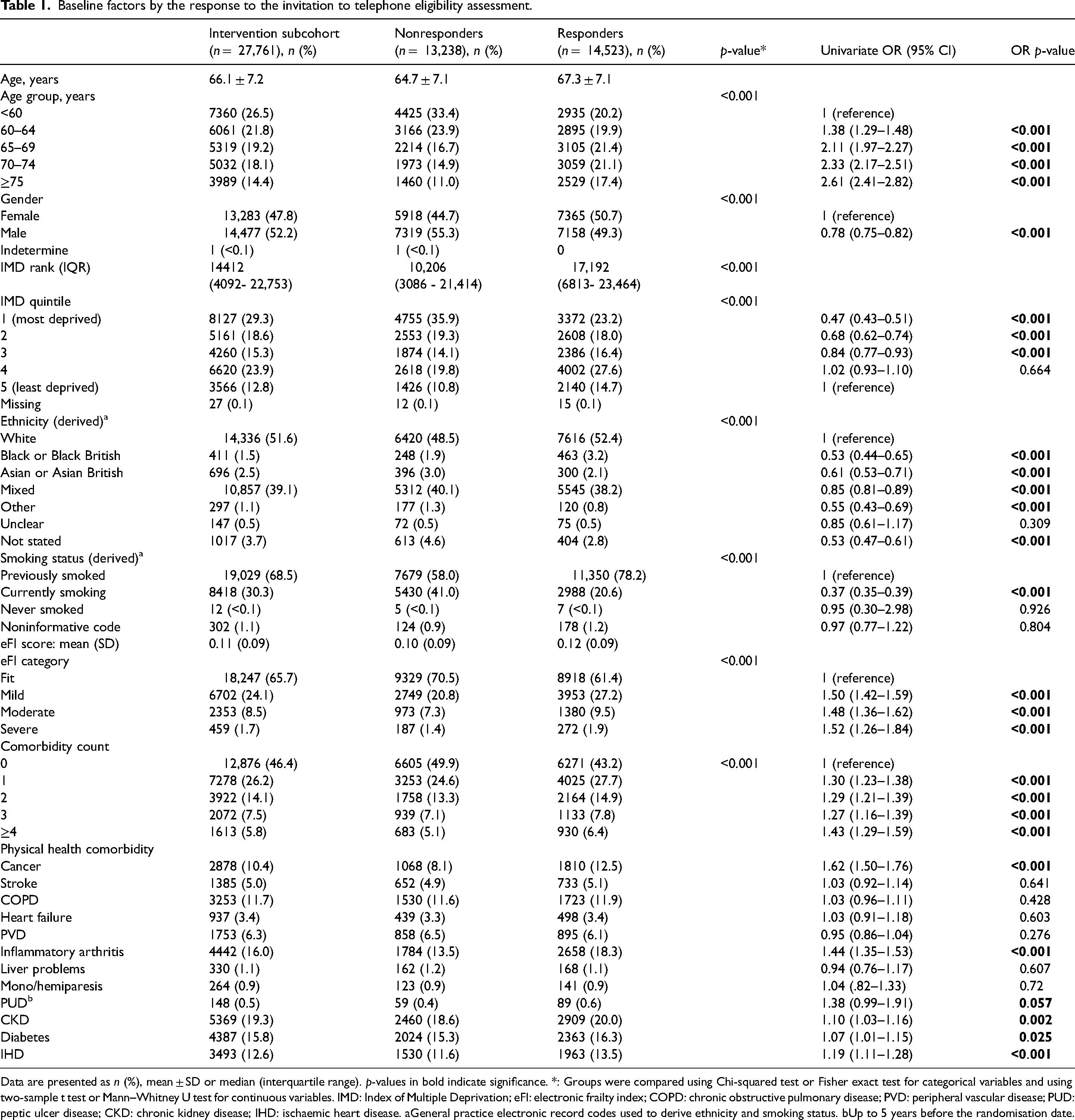
Data are presented as n (%), mean ± SD or median (interquartile range). p-values in bold indicate significance. *: Groups were compared using Chi-squared test or Fisher exact test for categorical variables and using two-sample t test or Mann–Whitney U test for continuous variables. IMD: Index of Multiple Deprivation; eFI: electronic frailty index; COPD: chronic obstructive pulmonary disease; PVD: peripheral vascular disease; PUD: peptic ulcer disease; CKD: chronic kidney disease; IHD: ischaemic heart disease. aGeneral practice electronic record codes used to derive ethnicity and smoking status. bUp to 5 years before the randomisation date.
Response to the invitation for telephone lung cancer risk assessment
Over half of the invitees (n = 14523, 52.5%) responded to the invitation for lung cancer risk assessment by making telephone contact. As reported previously, 12 age, sex, deprivation, ethnicity and smoking status were significantly different between responders and nonresponders (Table 1). A higher proportion of those responding were classified as having moderate (9.5%) or severe (1.9%) frailty compared to those who did not respond (7.3% and 1.4%, respectively) using eFI. There was a higher proportion of responders with three or more comorbidities (14.2%) than nonresponders (12.2%). Unadjusted and adjusted analysis of the effect of frailty and comorbidities on the response to the invitation is shown in Tables 1 and 2. Overall, individuals with mild, moderate and severe frailty were more likely to respond to invitation compared to fit individuals based on the eFI: adjusted OR (ORadj) 1.34, 95% CI 1.26–1.42; ORadj 1.28, 95% CI 1.16–1.40; ORadj 1.32, 95% CI 1.08–1.61, respectively). The sensitivity analysis of different polypharmacy prevalences showed similar results.
Relationship of frailty and comorbidities with response in multivariable analyses.
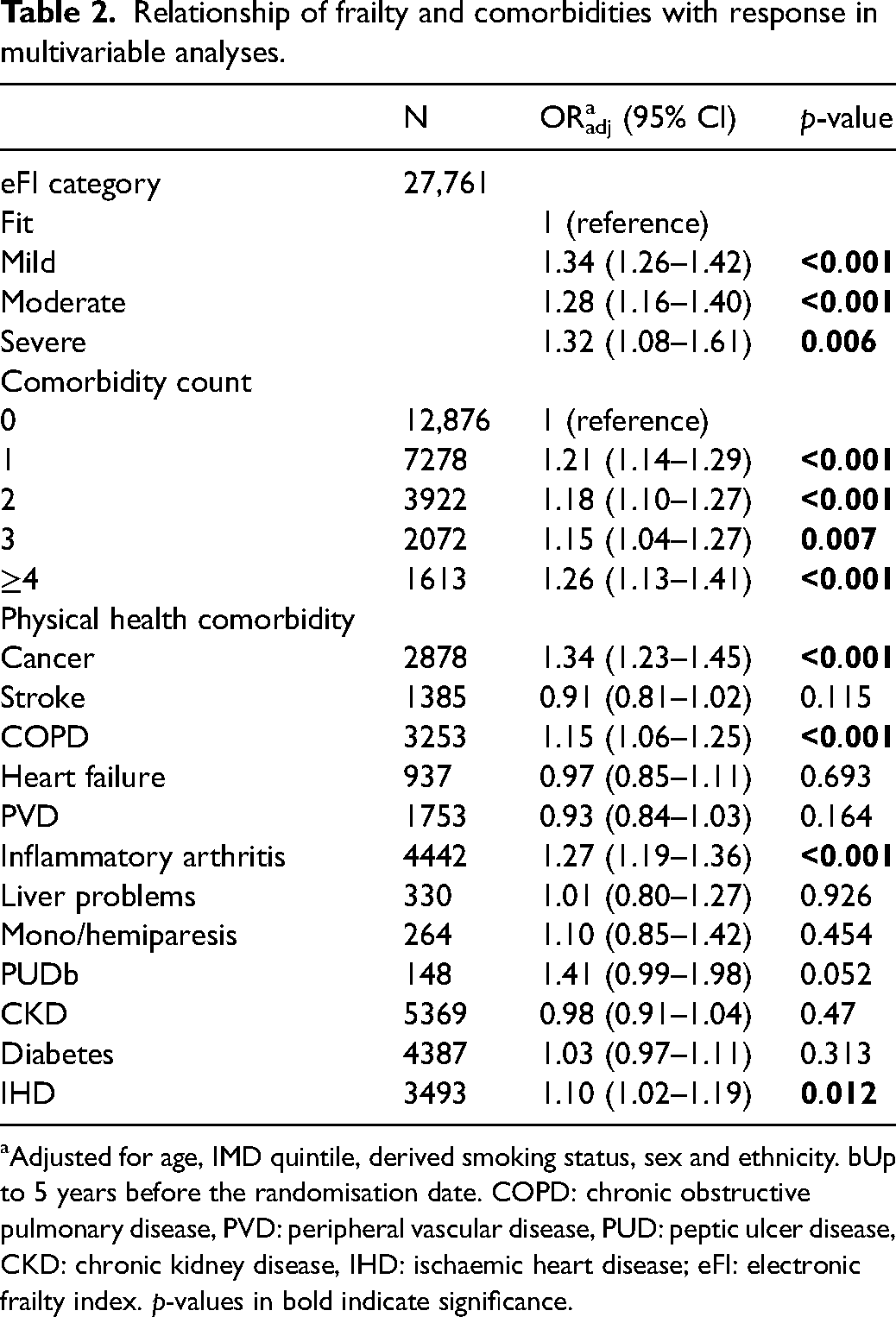
aAdjusted for age, IMD quintile, derived smoking status, sex and ethnicity. bUp to 5 years before the randomisation date. COPD: chronic obstructive pulmonary disease, PVD: peripheral vascular disease, PUD: peptic ulcer disease, CKD: chronic kidney disease, IHD: ischaemic heart disease; eFI: electronic frailty index. p-values in bold indicate significance.
People with 1, 2, 3 and 4 or more comorbidities were more likely to respond to the invitation compared to people without any comorbidities based on the comorbidity count of the 12 selected comorbidities (Table 2). Individuals with primary care records of comorbidities including cancer (ORadj 1.34, 95% CI 1.23–1.45), COPD (ORadj 1.15, 95% CI 1.06–1.25), inflammatory arthritis (ORadj 1.27, 95% CI 1.19–1.36) and IHD (ORadj 1.10, 95% CI 1.02–1.19) were more likely to respond to invitation compared with those without these conditions.
Uptake of LDCT screening in eligible responders
Of the 14,523 responders, 5041 met one of the three risk criteria and were invited for LDCT screening, representing 64.2% of all eligible invitees in the YLST intervention cohort. Of the 5041 invited, 4383 (86.9%) attended their appointment. As reported previously, 12 age, sex, deprivation and smoking status were all significantly different between those who attended their LHC appointment and those who did not. Following univariate analysis, both moderate and severe frailty were associated with lower attendance for LDCT screening, but there was no impact of mild frailty nor of comorbidity counts (Table 3). Adjusted analyses of the effect of frailty and comorbidities on the uptake of the LHC are presented in Table 4. The presence of moderate frailty was negatively associated with attendance for LDCT (ORadj 0.75, 95% CI 0.59–0.96, p = 0.024), and there was a trend to lower attendance with severe frailty (ORadj 0.67, 95% CI 0.43–1.04, p = 0.072) albeit the number of severely frail participants was much smaller than the other groups (n = 146, 2.9% of total eligible cohort). The sensitivity analysis estimating different polypharmacy prevalences showed similar results.
Baseline factors by attendance to lung health check appointment.
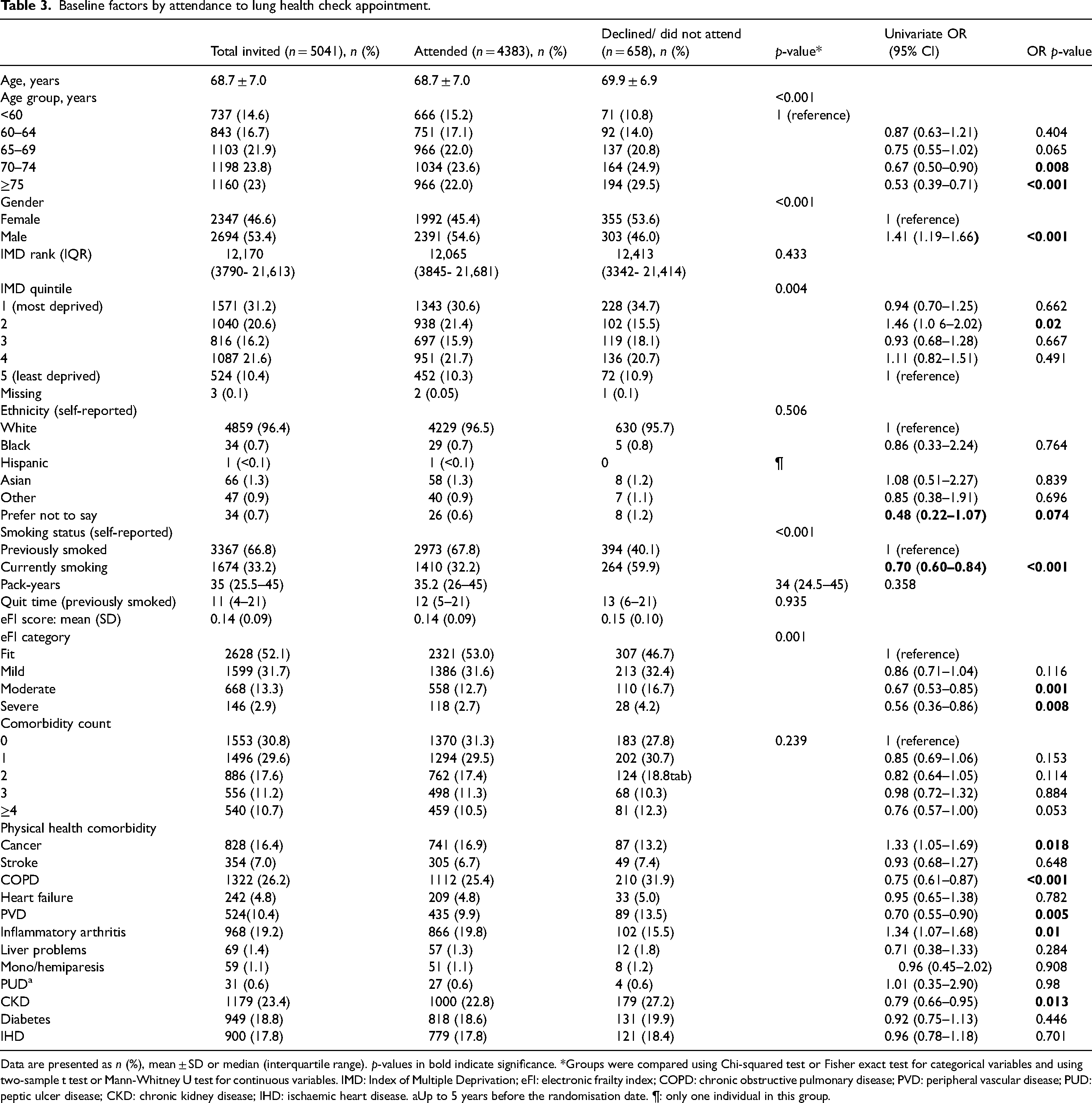
Data are presented as n (%), mean ± SD or median (interquartile range). p-values in bold indicate significance. *Groups were compared using Chi-squared test or Fisher exact test for categorical variables and using two-sample t test or Mann-Whitney U test for continuous variables. IMD: Index of Multiple Deprivation; eFI: electronic frailty index; COPD: chronic obstructive pulmonary disease; PVD: peripheral vascular disease; PUD: peptic ulcer disease; CKD: chronic kidney disease; IHD: ischaemic heart disease. aUp to 5 years before the randomisation date. ¶: only one individual in this group.
Relationship of frailty and comorbidities with lung health check appointment uptake in multivariable analyses.
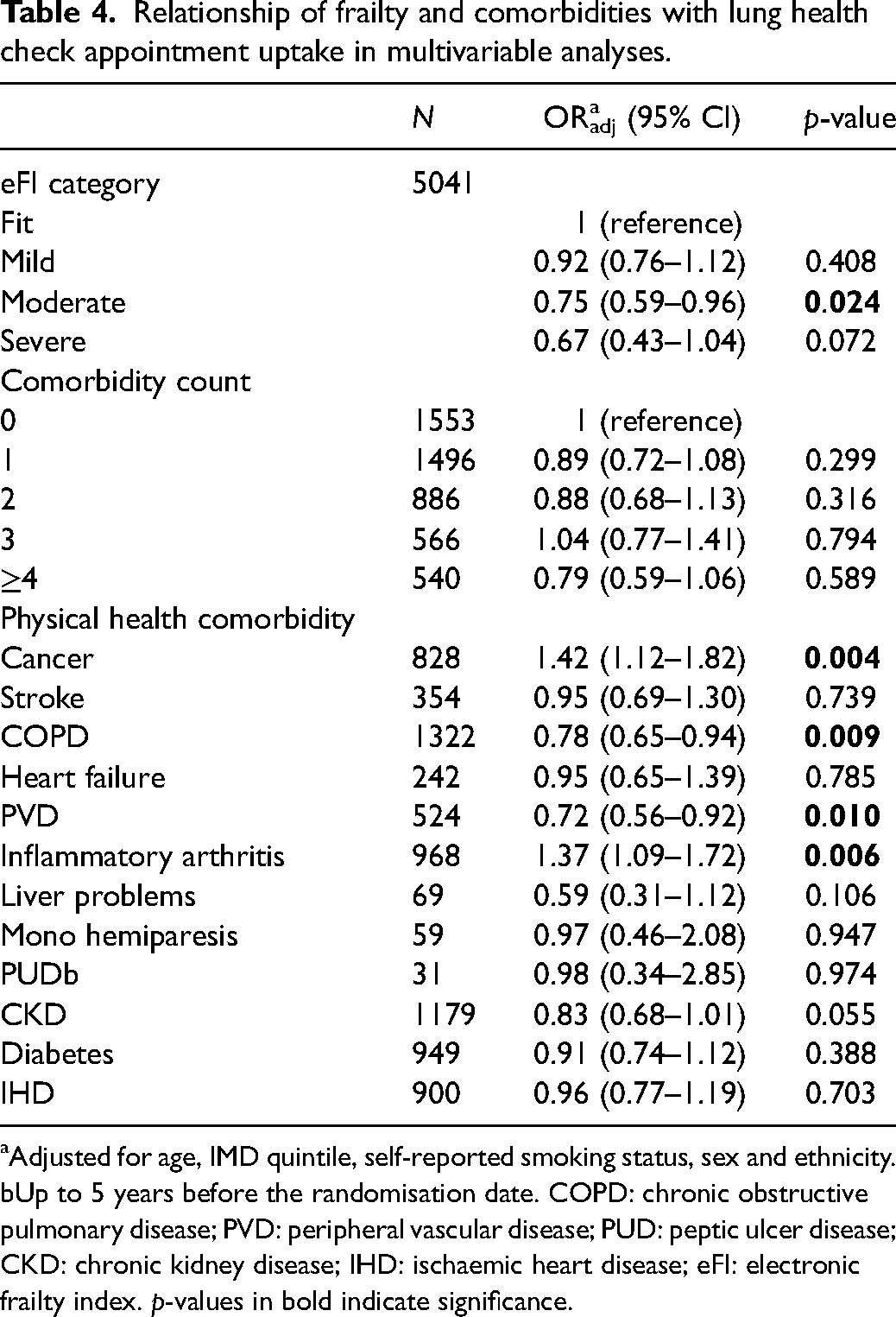
aAdjusted for age, IMD quintile, self-reported smoking status, sex and ethnicity. bUp to 5 years before the randomisation date. COPD: chronic obstructive pulmonary disease; PVD: peripheral vascular disease; PUD: peptic ulcer disease; CKD: chronic kidney disease; IHD: ischaemic heart disease; eFI: electronic frailty index. p-values in bold indicate significance.
All five levels of comorbidity count were not significantly associated with LDCT uptake (Table 4). However, individuals with cancer and inflammatory arthritis were more likely to attend the LHC appointment than those without these comorbidities (cancer ORadj 1.42, 95% CI 1.12–1.82; inflammatory arthritis ORadj 1.37, 95% CI 1.09–1.72). Conversely, individuals with COPD, PVD and CKD were less likely to attend the LHC appointment than those without these conditions (COPD ORadj 0.78, 95% CI 0.65–0.94; PVD ORadj 0.72 95%, CI 0.56–0.92; CKD ORadj 0.79, 95% CI 0.66–0.95).
Discussion
The current study measured the prevalence of frailty and selected comorbidities and their effects on response to the invitation for telephone lung cancer risk assessment and LDCT screening appointment uptake within the YLST. Our results indicate that mild, moderate and severe frailty, as defined by eFI, were prevalent in 24.1%, 8.5% and 1.7% of the invited population, respectively. We found an increase in response to telephone triage invitations based on the eFI frailty category whereby, compared to fit people, the odds of responding were 34%, 28%, and 32% increased in those with mild, moderate and severe frailty, respectively, after adjustment. These similar response rates suggest a threshold effect, where higher levels of frailty did not lead to a further increase in the odds of responding. Several factors might explain this effect in those with any level of frailty, including perceived vulnerability, previous interactions with healthcare services and increased health monitoring, which may make individuals with frailty more responsive to health-related invitations than fit individuals. Additionally, social support from caregivers or family members and the likelihood of not being in full-time employment could play a role in facilitating the initial telephone-based engagement for those with frailty. Conversely, fitter people with less interaction with healthcare may perceive themselves as lower risk and may ignore the invitation as a result. 17 Similar effects were seen with overall comorbidity counts (i.e. higher odds of response to invitation in people with comorbidities versus no comorbidities). The presence of cancer, COPD, inflammatory arthritis, and ischaemic heart disease were also associated with an increased response to telephone triage invitations. Regarding LDCT uptake, there was an indication of a non-significant dose-response relationship between frailty severity and attendance, with odds of attendance decreasing by 8%, 25%, and 33% for individuals with mild, moderate, and severe frailty, respectively, compared to those who were fit. There were no differences in uptake by comorbidity count. The presence of cancer and inflammatory arthritis were associated with increased odds of uptake, whereas a diagnosis of COPD reduced the odds of uptake.
To our knowledge, this is the first study that measures the prevalence of frailty severity and its impact on LCS invitation and uptake using an established frailty assessment tool, the eFI. 14 Previous LCS trials and studies relied on other metrics for determining the fitness and overall health of candidates, including self-reported health status, 3 the ability to climb stairs,3,18 the ability to lie flat19,20 and life expectancy.18,21,22 While these metrics might be practical and the only feasible options in many settings, they only capture part of the spectrum of frailty compared to a comprehensive frailty measure such as the eFI. In the UK, the eFI is currently integrated into primary care systems for all GPs in England 15 and Scotland, 23 making it a readily available option for assessing the severity of frailty when delivering LCS at the national level. In the context of LCS, incorporating well-established frailty models for frailty assessment remains a significantly underexplored avenue. Notably, a limited body of research has addressed the subject of frailty within the breast 24 and colon 25 cancer screening contexts. This underutilisation of frailty assessment in cancer screening might be due to the emerging nature of frailty as a concept and the challenges of assessing frailty through established frailty models in many settings.
Several studies have reported frailty in patients with lung cancer. One UK study reported that 31% of patients presenting with symptomatic lung cancer had some degree of frailty, as measured by the eFI, 26 and a recent meta-analysis reported the prevalence of frailty in patients with lung cancer to be around 45% (95% CI 28–61). 27 The results presented here show that 47.9% of those offered an LDCT screening appointment had some degree of frailty and are therefore consistent with these estimates.
The prevalence of individual physical comorbidities in our cohort is in line with what has been observed in LCS settings 7 and is comparable to what has been reported among the eFI development cohort. 14 In our cohort, individuals with several comorbidities (e.g. cancer, COPD, inflammatory arthritis and IHD) were more likely to be contacted for telephone risk assessment following postal invitation, and the presence of cancer and inflammatory arthritis was additionally associated with an increased likelihood of attending the screening appointment for those eligible following a risk assessment. Previous malignancy might encourage attendance due to greater awareness of the importance of early detection. Findings regarding COPD were somewhat conflicting, with the presence of COPD increasing the likelihood of undergoing telephone risk assessment but reducing the likelihood of attending screening for those fulfilling eligibility criteria. Evidence from the US has shown increased LCS participation overall among candidates with self-reported COPD. 28 The benefit of LCS relates to the life years gained by participants in whom a lung cancer death is prevented through early diagnosis and treatment. Given that increasing frailty is strongly linked to reduced life expectancy, the fact that fit people are less likely to respond to an initial invitation to participate in screening is concerning. Qualitative research is required to better understand the impact of frailty and fitness on decision-making around screening participation. In addition, determining the impact of frailty and comorbidity on LCS outcomes is of great interest and will be the subject of a future paper.
Strengths and limitations
The current study gives a unique insight into the target population for LCS and has several strengths, including a large sample size, being representative of the whole YLST screening arm, the novel investigation of an established, widely appliable frailty tool in the context of UK LCS and the ability to investigate non-response to the screening invitation. A possible limitation is the inability to collect polypharmacy data from all participants due to logistical challenges. To overcome this, we conducted a series of sensitivity analyses, which indicated that our results were robust. An additional consideration is that the age range for the population invited to participate in YLST was from 55 to 80 years at the time of data extraction, whereas other screening programmes, such as the Targeted Lung Health Check programme in England, only screen up to 74 years. The prevalence of frailty has been shown to be higher in those invitees over 75 years, and this will influence the generalisability of our findings to screening programmes accordingly. Finally, responses to LCS invites within a trial context may differ from LCS offered outside research settings. YLST was designed as an implementation study for LCS, and as such, the initial written invitation and telephone call did not mention any research. While the research study was fully discussed with participants at the time they attended the mobile unit for screening (prior to obtaining written consent), the timing of response and uptake predated the discussion about research.
Conclusion
The key finding from this study is that frailty is associated with a higher likelihood of people undergoing telephone risk assessment for lung cancer following postal invitation as part of a community-based LCS programme. Conversely, amongst those eligible for screening and offered an appointment for LDCT, there was some evidence of reduced uptake associated with frailty. By focusing efforts on encouraging initial engagement from the fit population who potentially have more life years to be gained, LCS programmes may be able to maximise the clinical efficacy of the intervention.
Supplemental Material
sj-docx-1-msc-10.1177_09691413251315087 - Supplemental material for Impact of frailty and comorbidity on initial response to lung cancer screening invitation and low-dose CT screening uptake: Findings from the Yorkshire Lung Screening Trial
Supplemental material, sj-docx-1-msc-10.1177_09691413251315087 for Impact of frailty and comorbidity on initial response to lung cancer screening invitation and low-dose CT screening uptake: Findings from the Yorkshire Lung Screening Trial by Anas Almatrafi, Rhian Gabe, Rebecca J Beeken, Richard D Neal, Andrew Clegg, Kate E Best, Samuel Relton, Martel Brown, Hui Zhen Tam, Neil Hancock, Philip A.J. Crosbie and Matthew E.J. Callister in Journal of Medical Screening
Footnotes
Acknowledgements
We acknowledge the contribution of the whole Yorkshire Lung Screening Trial clinical team in delivering this study.
Data sharing arrangements
Researchers wishing to use the data will need to complete a request for data sharing form describing a methodologically sound proposal. The form will need to include the objectives, what data are requested, timelines for use, intellectual property and publication rights, data release definition in the contract and participant informed consent, etc. A data-sharing agreement from the sponsor may be required.
Declaration of conflicting interests
P.A.J. Crosbie reports stock options from Everest Detection, and lecture honoraria from Bayer, outside the submitted work. R.J. Beeken reports fellowship and grant funding from Yorkshire Cancer Research and grant funding from Roy Castle Lung Cancer Foundation, outside the submitted work. A. Clegg has received consultancy fees from the Geras Centre for Aging Research, received meeting/travel support from the Australian and New Zealand Society of Geriatric Medicine, and is a chair of the global Ageing Research Trialists collaborative.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yorkshire Cancer Research (grant number L403).
Support statement
This work was funded by Yorkshire Cancer Research (award reference L403). A. Almatrafi is supported by a PhD scholarship from Umm Al-Qura University in Saudi Arabia. P.A.J. Crosbie is supported by the Manchester National Institute for Health Research Manchester Biomedical Research Centre (IS-BRC-1215-20007).
Patient and public involvement statement
A PPIE group was set up specifically for the Yorkshire Lung Screening Trial, comprising three people affected by cancer. Group members contributed to the protocol, advised on trial design issues, and reviewed all participant-facing materials. In addition, the Leeds Lung Cancer and Mesothelioma Support group reviewed all trial design issues and contributed to the participant-facing materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.