
Abstract
Background
Late-stage cancer incidence has been proposed as an early surrogate for mortality in randomized controlled trials (RCTs) of cancer screening; however, its validity has not been systematically evaluated across screening RCTs of different cancers.
Methods
We conducted a meta-regression analysis of cancer screening RCTs that reported both late-stage cancer incidence and cancer mortality. Based on a systematic literature review, we included 33 RCTs of screening programs targeting seven cancer types, including lung (n = 12), colorectal (n = 8), breast (n = 5), and prostate (n = 4), among others. We regressed the relative reduction of cancer mortality on the relative reduction of late-stage cancer incidence, inversely weighted for each RCT by the variance of estimated mortality reduction.
Results
Across cancer types, the relative reduction of late-stage cancer incidence was linearly associated with the relative reduction of cancer mortality. Specifically, we observed this association for lung (R2 = 0.79 and 0.996 in three recent large trials), breast (R2 = 0.94), prostate (R2 = 0.98), and colorectal cancer (R2 = 0.75 for stage III/IV cancers and 0.93 for stage IV cancers). Trials with a 20% or greater reduction in late-stage cancers were more likely to achieve a significant reduction in cancer mortality. Our results also showed that no reduction of late-stage cancer incidence was associated with no or minimal reduction in cancer mortality.
Conclusions
Meta-regression of historical screening RCTs showed a strong linear association between reductions in late-stage cancer incidence and cancer mortality.
Keywords
Introduction
Randomized controlled trials (RCTs) demonstrating a reduction in cancer-specific mortality have been the conventional gold standard for establishing the benefit of cancer screening tests. Such trials, however, require large study populations followed for many years—often decades—to accrue mortality events for sufficient power. Over such long time periods, many changes relevant to trial results can occur. For example, there may be advances in genomics-based technologies and machine-learning algorithms now being deployed for cancer early detection; the incidence of certain cancer types may decrease 1 ; and improvements in cancer care and therapies will improve patient survival and potentially dilute the screening effect on cancer mortality in an RCT. Thus, by the time of study completion, the original screening technologies assessed in long-term RCTs may be obsolete 2 ; or the planned RCT design parameters, such as power and effect size, may become outdated. Moreover, no screening RCTs are likely ever to be sufficiently powered to detect a mortality reduction for individual uncommon cancer types, which together comprise one quarter of the total cancer burden. 3 Consequently, relying on cancer mortality may impede evaluation and implementation of effective screening tests, with potentially substantial public health costs. More expeditious methods for evaluation of benefits and harms of new cancer screening tests are needed.
There are several proposed early indicators of a future reduction in cancer mortality. These include prognostic characteristics known at or near the time of diagnosis with respect to tumor extent or spread, as these are not confounded by cancer treatment.4,5 Specifically, endpoints based on stage at diagnosis—including a reduction in late-stage cancer incidence (sometimes referred to as “stage shift”), which is not affected by overdiagnosis of indolent early-stage cancers—have been considered in lieu of cancer-specific mortality in RCTs for single-cancer early detection tests5–12 and more recently proposed for multi-cancer early detection (MCED) tests.13–15 Relatedly, as a conceptual framework, stage-shift models are well-established and commonly used to project the mortality benefit of early detection tests based entirely on the shifted stage distribution.16–18
Formal procedures have been proposed to evaluate the potential of a proposed intermediate as a surrogate for a given true clinical endpoint. The seminal Prentice criterion requires that the test of the intervention effect on the surrogate would also be a valid test of its effect on the true endpoint in an RCT 19 ; this would be satisfied if the effect of the intervention on the true endpoint were completely mediated by the surrogate. Less stringent criteria have been proposed, for example, the proportion of intervention effect explained by the surrogate in a regression framework, typically requiring individual-level data from trials. A meta-regression approach has been proposed to assess trial-level correlation of intervention effects on the surrogate and intervention effects on the true endpoint across multiple RCTs. 20 Recently, Feng et al. estimated the association between the effect of trial arm on cancer stage and the corresponding effect on the first reported cancer-specific mortality endpoint in a meta-analysis of cancer screening trials. 21 They reported mixed results, with relatively weak associations for several cancer types.
In the present work, we systematically identified rigorously conducted cancer screening RCTs across seven cancer types and assessed the trial-level association between the reduction of late-stage cancer incidence and the reduction of cancer mortality. When there were multiple reports from the same trial, we focused on the reports of cancer mortality with longer follow-up. While Feng et al. defined late-stage cancers as stage III/IV cancers for most cancer types, we also allowed different dichotomization of cancer stages by cancer type, for example, stage IV as late-stage for prostate cancer. The goal was to evaluate whether the reduction of late-stage cancer incidence has been robustly correlated with cancer mortality benefit in past cancer screening RCTs, across the spectrum of single cancer types that have been targeted.
Methods
Literature search methods
The objective of our systematic literature review was to identify cancer screening RCTs that reported quantitative results for late-stage cancer incidence and cancer-specific mortality in both the intervention arm and the comparator arm. The literature search methods are described in detail in the Supplemental Materials.
Briefly, we developed our literature search criteria to supplement existing recent systematic literature reviews of cancer screening conducted by the US Preventive Services Task Force (USPSTF),22,23 with additional searching of the PubMed database for RCTs of screening for cancer types with population-based screening tests not evaluated by USPSTF, published as of 22 August 2023. We also searched for RCTs of screening for cancer types addressed by USPSTF but published after each most recent USPSTF Evidence Synthesis. In addition, we examined reference lists of included RCTs and relevant review articles to identify potentially relevant RCTs. The literature search strategy and all studies identified, along with reasons for exclusion of those not included after full-text review, are provided in Supplemental Tables 1–4. We excluded studies that were not randomized, did not report quantitative results for both outcomes of interest, did not describe power and sample size planning for detecting an effect on cancer-specific mortality, or did not report cancer incidence by tumor-node-metastasis stage. Thus, for example, we excluded studies that reported results only by tumor size or lymph node status. We also excluded studies described by the USPSTF as having inadequate randomization. 23 A flow chart illustrating the literature search and selection process is provided in Supplemental Figure 1.
Table 1 lists the RCTs included in this analysis, grouped by targeted cancer type. For each RCT, the number of cancer-specific deaths is shown as an indicator of the power of the study. Table 1 also shows whether an included study was previously used in a USPSTF Evidence Synthesis.
Eligible randomized clinical trials of cancer screening for meta-regression analysis.
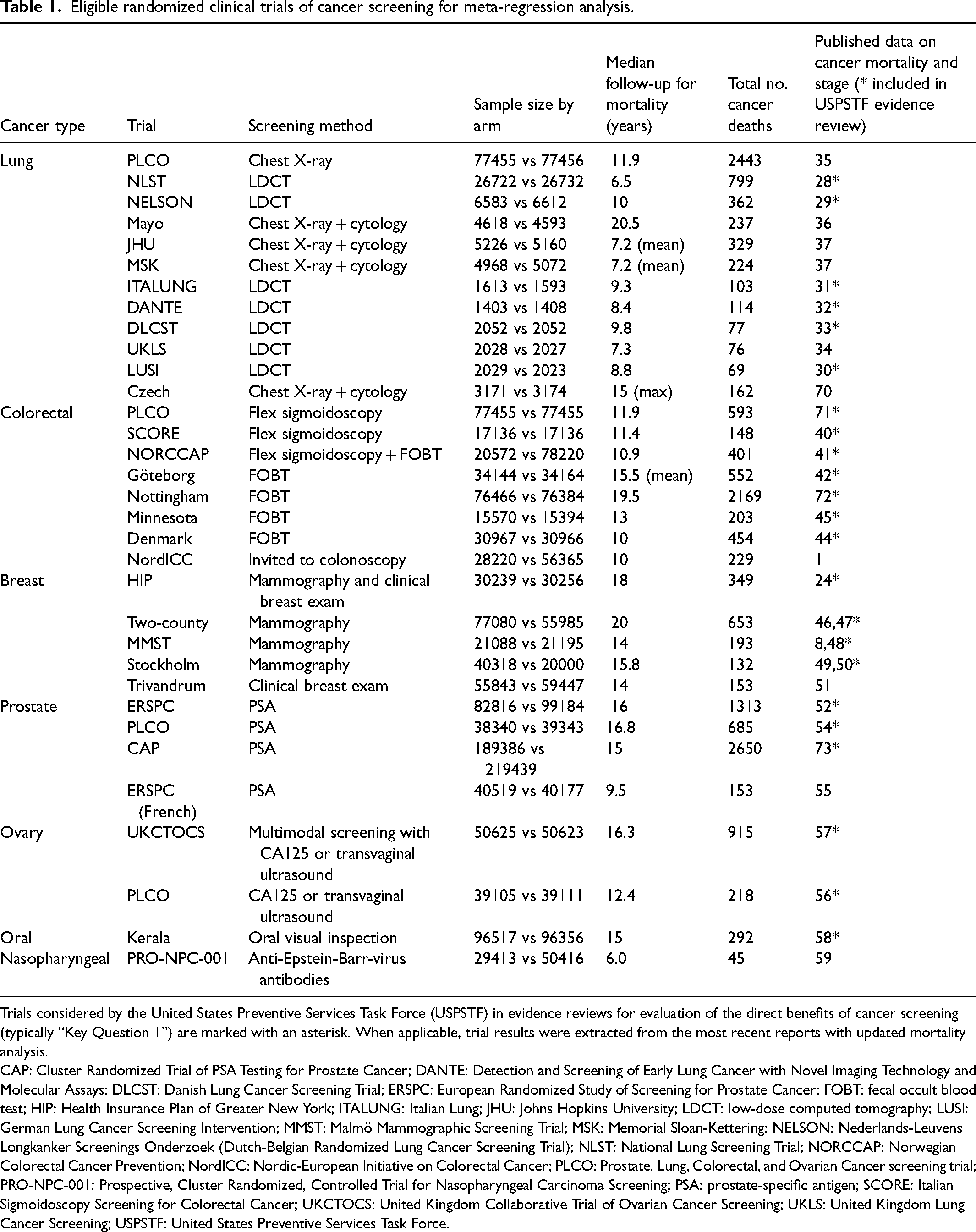
Trials considered by the United States Preventive Services Task Force (USPSTF) in evidence reviews for evaluation of the direct benefits of cancer screening (typically “Key Question 1”) are marked with an asterisk. When applicable, trial results were extracted from the most recent reports with updated mortality analysis.
CAP: Cluster Randomized Trial of PSA Testing for Prostate Cancer; DANTE: Detection and Screening of Early Lung Cancer with Novel Imaging Technology and Molecular Assays; DLCST: Danish Lung Cancer Screening Trial; ERSPC: European Randomized Study of Screening for Prostate Cancer; FOBT: fecal occult blood test; HIP: Health Insurance Plan of Greater New York; ITALUNG: Italian Lung; JHU: Johns Hopkins University; LDCT: low-dose computed tomography; LUSI: German Lung Cancer Screening Intervention; MMST: Malmö Mammographic Screening Trial; MSK: Memorial Sloan-Kettering; NELSON: Nederlands-Leuvens Longkanker Screenings Onderzoek (Dutch-Belgian Randomized Lung Cancer Screening Trial); NLST: National Lung Screening Trial; NORCCAP: Norwegian Colorectal Cancer Prevention; NordICC: Nordic-European Initiative on Colorectal Cancer; PLCO: Prostate, Lung, Colorectal, and Ovarian Cancer screening trial; PRO-NPC-001: Prospective, Cluster Randomized, Controlled Trial for Nasopharyngeal Carcinoma Screening; PSA: prostate-specific antigen; SCORE: Italian Sigmoidoscopy Screening for Colorectal Cancer; UKCTOCS: United Kingdom Collaborative Trial of Ovarian Cancer Screening; UKLS: United Kingdom Lung Cancer Screening; USPSTF: United States Preventive Services Task Force.
Data extraction and statistical methods
For all RCTs included in this meta-regression analysis, we extracted the published relative risks (RRs) for cancer-specific mortality, along with 95% confidence intervals (CIs). Most RCTs did not report an RR for late-stage cancer incidence.
To calculate an RR measure of the effect of screening on cancer stage in these historical trials, we dichotomized cancer stages as “early-stage” or “late-stage” using a cancer-type-specific approach. The dichotomization rule for each cancer type was determined by whether a reduction in incidence of the defined late-stage cancers would likely predict a reduction in cancer-specific mortality in the general population. Several factors were considered in determining these rules. First, and most importantly, are the cancer stages identified as late-stage associated with markedly different cancer-specific mortality when compared with early-stage, such that downstaging from late to early stage would entail a substantial reduction in cancer-specific mortality? Second, is the defined late-stage cancer sufficiently frequent that, if used as an early surrogate of cancer mortality, it will result in a more powerful test than testing the reduction of cancer mortality? Third, do cancer stages grouped together as either late or early have similar mortality rates, thereby minimizing within-group variability in cancer mortality? These three considerations pertain to the plausibility of whether a screening effect on cancer-specific mortality can be largely mediated via an effect on defined late-stage incidence. Using population-based cancer registry data in the US (Supplemental Table 5) and England (Supplemental Table 6) to guide these considerations, we defined late-stage cancers as stages III/IV for lung and ovarian cancers. For colorectal cancer (CRC), we assessed late-stage as stage III/IV or stage IV (or Dukes’ stage D), in part due to a moderate mortality rate for stage III (or Dukes’ stage C). For breast cancer, population-based cancer registry data indicates that only a minority of deaths occur from stages III and IV disease at diagnosis, whereas 80–90% of deaths occur from stages II, III, and IV combined (Supplemental Tables 5 and 6). Furthermore, the mortality of stage II breast cancers was much higher in the 1980s, for example, 60–70% in the Health Insurance Plan of Greater New York (HIP) trial. 24 We therefore defined late-stage breast cancer as stage II or later. This is also consistent with previous analyses of breast cancer.8,25 For prostate cancer, we noted that stages I–III have a low mortality rate; almost 70% of prostate cancer deaths occur in stage IV. We therefore use metastatic disease (stage IV) as the primary definition of late-stage for prostate cancer.
Based on published counts of incident late-stage cancers diagnosed during trial follow-up, we computed RRs for late-stage cancer incidence comparing the intervention and control arms, and estimated the standard error using Poisson regression. Forest plots of the two RRs were drawn using the ggplot2 package in the R statistical programming language.26,27
We used a meta-regression approach to assess the trial-level surrogacy of late-stage cancer incidence for cancer-specific mortality. We used a simple stage-shift model for predicting cancer mortality to show that the relative reduction of cancer mortality is linearly dependent on the relative reduction of late-stage cancer incidence (Supplemental Methods). For each cancer type with multiple RCTs (lung, CRC, breast, and prostate), we linearly regressed the relative reduction of cancer mortality on the relative reduction of late-stage cancer incidence, weighted by the reciprocal of the variance of estimated relative mortality reduction. Three statistics were computed to evaluate surrogacy, including R2, which summarizes how much variability of the estimated mortality reduction is explained by the reduction of late-stage cancer incidence. The slope of the meta-regression line represents the degree of mortality reduction per unit reduction of late-stage incidence. The intercept of the meta-regression line provides auxiliary evidence, assessing whether a null effect on late-stage cancer incidence would be associated with a null effect on cancer mortality. Ideally, a large R2 that is close to 1, a slope that is significantly greater than zero, and a close-to-zero intercept constitute evidence of a good surrogate.
Our primary analysis included RCTs of lung (n = 12), CRC (n = 8), breast (n = 5), and prostate (n = 4) cancers. In an exploratory analysis, although we would not expect a common line of dependence for all cancers, we pooled 33 RCTs of all seven cancer types (including RCTs of ovarian (n = 2), oral (n = 1), and nasopharyngeal (n = 1) cancers) to perform a meta-regression. The R2 was computed by first using the cancer-specific slopes and intercepts to compute the predicted mortality reduction, and then calculating the weighted average R2 across cancers.
Results
Lung cancer screening trials
Figure 1 shows the relationship between the screening effects on stages III/IV cancer incidence and the effects on cancer mortality among 12 lung cancer screening RCTs. The majority of trials, including the National Lung Screening Trial (NLST), 28 Nederlands-Leuvens Longkanker Screenings Onderzoek (Dutch-Belgian Randomized Lung Cancer Screening Trial; NELSON), 29 and several smaller studies,30–34 tested low-dose computed tomography (LDCT) as the screening modality. The Prostate, Lung, Colorectal, and Ovarian (PLCO) cancer screening trial was powered to test the effect of chest radiography on lung cancer mortality, 35 and the Mayo Clinic, 36 Johns Hopkins University, 37 Memorial Sloan-Kettering, 37 and Czech 38 trials in the early 1970s tested radiologic and cytologic screening. Only NLST and NELSON yielded a statistically significant reduction of lung cancer mortality, while several small European trials did not reach statistical significance despite reporting a large reduction of mortality. At the trial level, there was clear positive correlation between the RRs for cancer mortality and for stages III/IV incidence: R2 = 0.996 based on the three recent large trials adequately powered for lung cancer mortality (NLST, NELSON, and PLCO; Figure 1(C)), R2 = 0.79 based on all 12 trials (Figure 1(B)). Both meta-regression models yielded a statistically significant linear slope, which was greater based on the three large trials (slope = 1.06) than all 12 trials (slope = 0.72). Both models resulted in a near-zero intercept, suggesting that mortality reduction would be nearly zero if there were no reduction in stages III/IV incidence. In an exploratory analysis, using stage IV lung cancers as late-stage cancers yielded a high R2 but a smaller slope (Supplemental Figure 2).
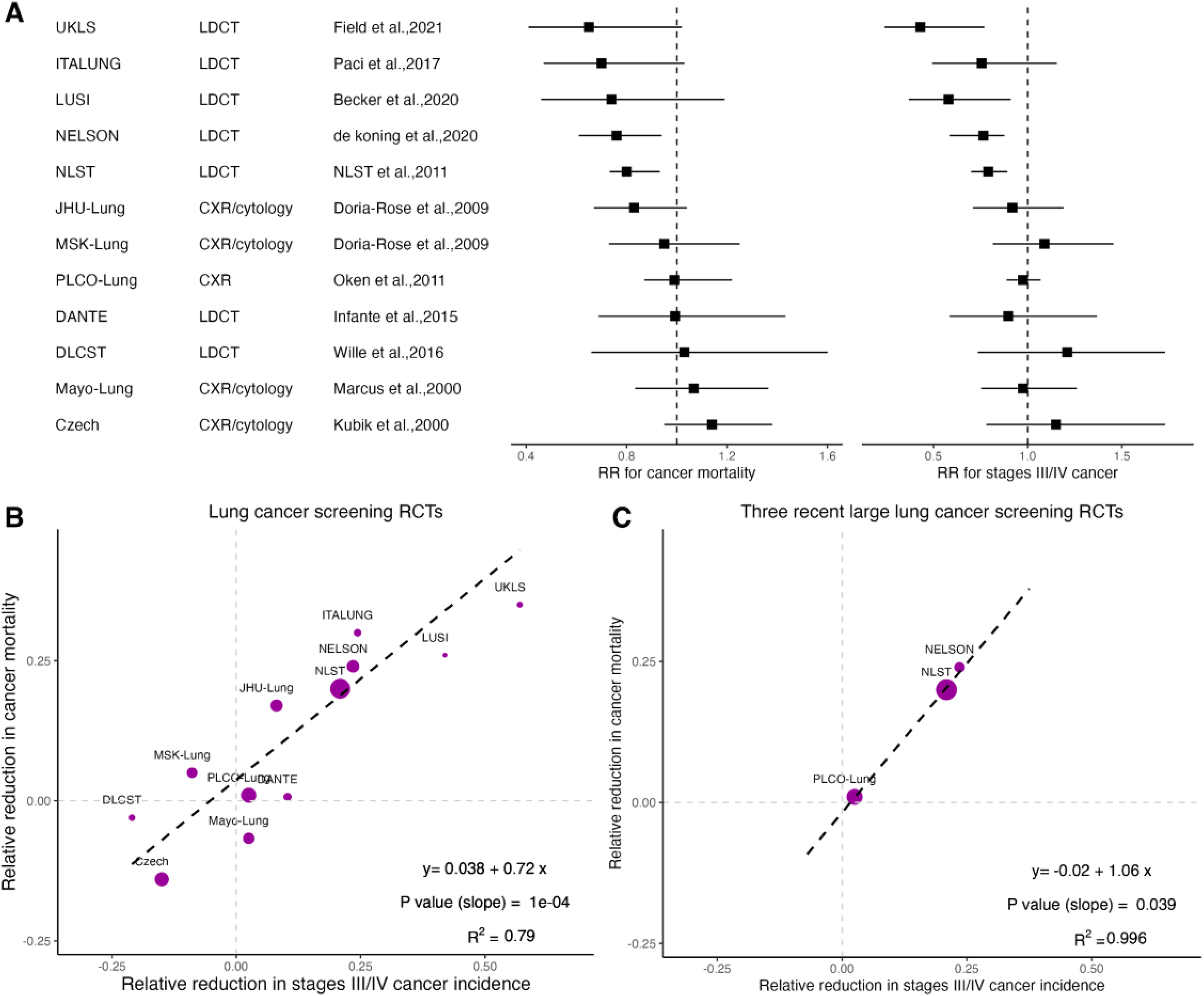
Published randomized clinical trials for lung cancer screening with cancer mortality and stage distribution available for meta-regression. (A) The relative risk (RR) for cancer mortality and RR for stages III/IV incidence are shown. (B) The weighted meta-regression line is shown for all 12 trials. (C) The weighted meta-regression line is shown for the three large trials. In B and C, the sizes of the dots are proportional to the precision of the corresponding estimated RR for cancer mortality.
Colorectal cancer screening trials
The screening effects on late-stage CRC incidence and mortality in eight RCTs are shown in Figure 2. These trials used various screening modalities (flexible sigmoidoscopy for PLCO, 39 Italian Sigmoidoscopy Screening for Colorectal Cancer (SCORE), 40 and Norwegian Colorectal Cancer Prevention (NORCCAP); 41 fecal occult blood test (FOBT) for Göteborg, 42 Nottingham, 43 Denmark, 44 and Minnesota; 45 and colonoscopy for Nordic-European Initiative on Colorectal Cancer (NordICC) 1 ) and cancer staging systems (Dukes’, American Joint Committee on Cancer (AJCC), and Union for International Cancer Control (UICC)). Seven out of eight RCTs demonstrated a statistically significant reduction in CRC mortality. In an analysis limited to metastatic CRC (stage IV or Dukes’ D) incidence among six RCTs with published data on this endpoint (Figure 2(C)), strong correlation was observed, with R2 = 0.93, slope = 0.57 (p = 0.002), and intercept = 0.08. The meta-regression line of screening effects on cancer mortality and stages III/IV or Dukes’ C/D incidence among all eight trials yielded a less pronounced association (R2 = 0.75, p = 0.01, Figure 2(B)). The combination of endoscopy and FOBT trials may be inappropriate, because whereas FOBT works primarily by detecting CRC at an earlier stage, endoscopic screening works by reducing the incidence of CRC at all stages. When separating FOBT trials and sigmoidoscopy/colonoscopy trials (Supplemental Figure 3), FOBT trials showed a significant linear relationship (R2 = 0.91, p = 0.05), but sigmoidoscopy/colonoscopy trials did not.
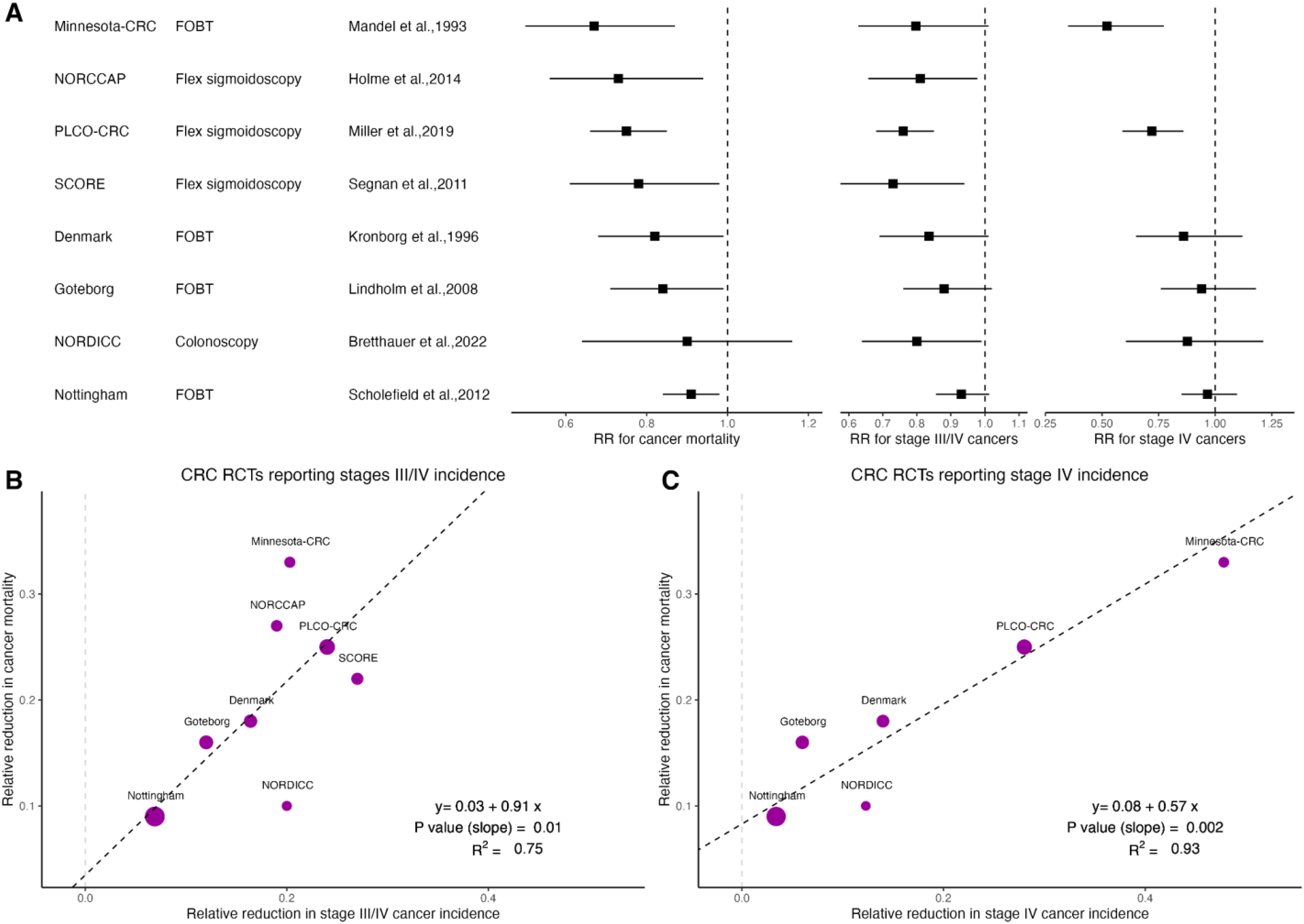
Published randomized clinical trials for colorectal cancer (CRC) screening with cancer mortality and stage distribution available for meta-regression. (A) The relative risk (RR) for cancer mortality, RR for stages III/IV, and stage IV incidence are shown. (B) The weighted meta-regression line is shown for the eight trials reporting stage III/IV incidence. (C) The weighted meta-regression line is shown for the six trials reporting stage IV incidence. In B and C, the sizes of the dots are proportional to the precision of the corresponding estimated RR for cancer mortality.
Breast cancer screening trials
Figure 3 shows results from the five breast cancer screening RCTs included in our analysis. Four of the five RCTs tested for a mortality benefit of mammography (HIP, 24 Two-County,46,47 Malmö Mammographic Screening Trial (MMST),8,48 Stockholm49,50) and were previously analyzed in two meta-regression publications;8,9 all four of these trials demonstrated a reduction of breast cancer mortality. A recent cluster RCT in Trivandrum, India, evaluated the effectiveness of clinical breast examination (CBE), and did not demonstrate any mortality benefit. 51 The meta-regression model of the five RCTs resulted in a strong linear relationship between the screening effects on stages II/III/IV incidence and breast cancer mortality (R2 = 0.94, slope = 0.84, p = 0.01, intercept = 0.05). Removing the CBE trial as an outlier increased R2 to 0.97 and the linear slope to 1.04. In Supplemental Figure 3, using stage IV or stage III/IV as late-stage cancers yielded R2 values of 0.92 and 0.55, respectively.
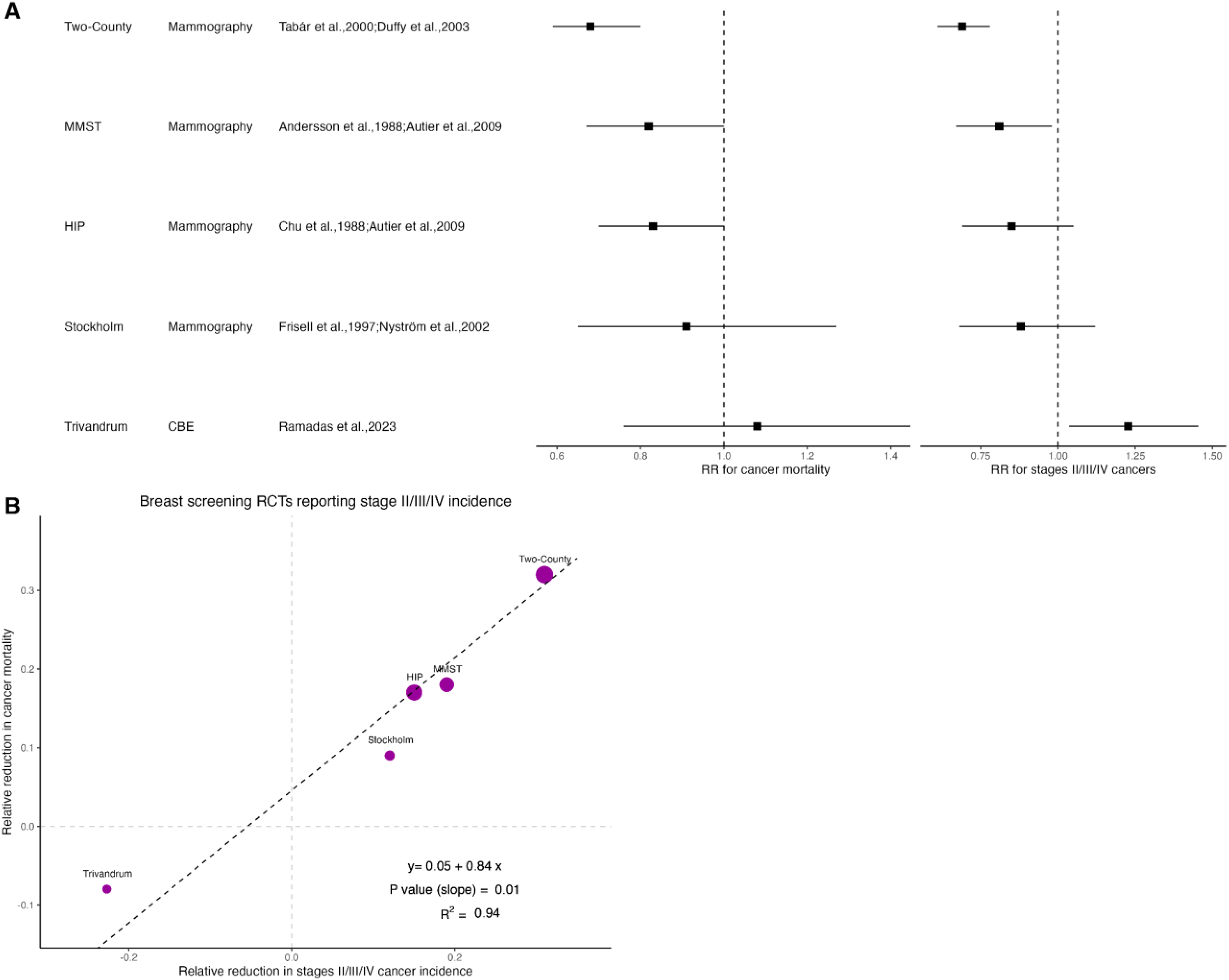
Published randomized clinical trials for breast cancer screening with clinical stage distribution available for meta-regression. (A) The relative risk (RR) for cancer mortality and RR for stages II/III/IV incidence are shown in forest plots. (B) The weighted meta-regression line is shown for five breast cancer trials, where the sizes of the dots are proportional to the precision of the corresponding estimated RR for cancer mortality.
Prostate cancer screening trials
Three prostate cancer screening trials (European Randomized Study of Screening for Prostate Cancer (ERSPC), 52 Cluster Randomized Trial of PSA Testing for Prostate Cancer (CAP), 53 and PLCO), 54 all of which evaluated the screening effect of prostate-specific antigen (PSA) testing on cancer mortality, are included in Figure 4. The French section of ERSPC 55 was initially reported separately from the primary results of ERSPC, which encompassed seven other European countries, and was therefore included as a fourth trial in a secondary analysis. Only the main ERSPC trial and the CAP trial (15 years follow-up) showed a statistically significant reduction of cancer mortality. Despite slight study differences in the definition of late-stage cancers, the meta-regression model of the three large main RCTs and the French ERSPC study yielded a strong linear trend (R2 = 0.98, slope = 0.45, p = 0.01, intercept = 0.003). Using high-risk prostate cancers including metastatic diseases only slightly reduced the association (R2 = 0.94, slope = 0.8, p = 0.03, intercept = –0.02, Supplemental Figure 5).
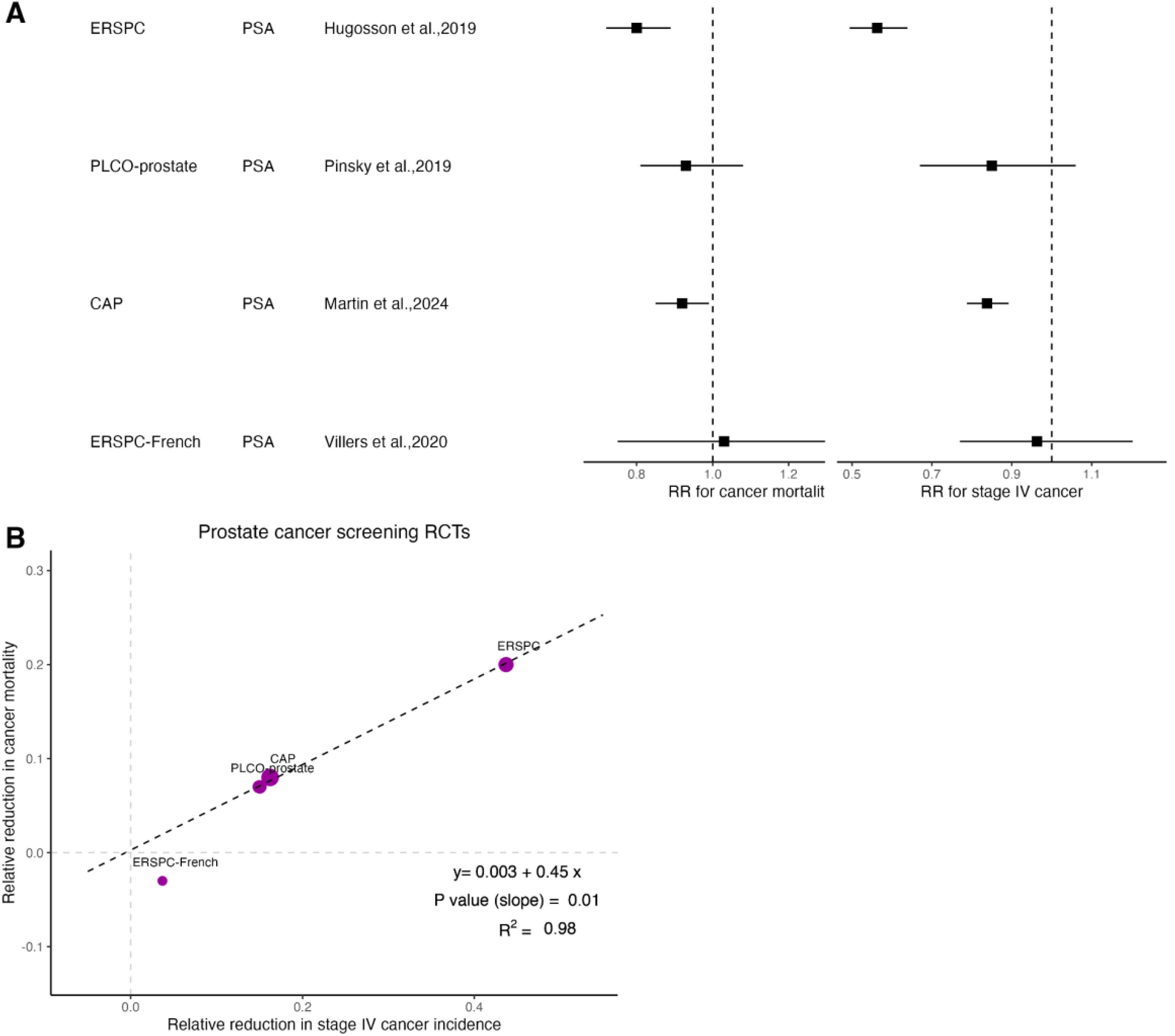
Published randomized clinical trials for prostate cancer screening with clinical stage distribution available for meta-regression. (A) The relative risk (RR) for cancer mortality and RR for stage IV incidence are shown in forest plots. (B) The weighted meta-regression line is shown for the four trials. The sizes of the dots are proportional to the precision of the corresponding estimated RR for cancer mortality.
Combined analysis across all cancer screening trials
Figure 5 shows the scatter plot of all 33 eligible RCTs across cancer types (including two RCTs for ovarian cancer,56,57 one RCT for oral cancer, 58 and one RCT for nasopharyngeal cancer 59 ), and the diagonal line crossing the origin. The majority of trials had a reduction of late-stage cancers and a similar reduction of cancer mortality (the first quadrant). Consistent with the cancer-specific analyses, we observed a strong association between the reduction of late-stage cancer incidence and the reduction of cancer-specific mortality. After adjusting for different slopes and intercepts among different cancer types, the overall R2 was 0.75. Rather than showing the regression line, which is difficult to interpret as it is a combination of different regression lines for different cancers, we show the diagonal line as ideal agreement, which would be observed if the effect of the screening intervention on incidence of advanced stage were exactly equal to its predicted effect on cancer-specific mortality. Although inevitably there is variation, the results clustered close to this line of ideal agreement.

A scatter plot with all 33 cancer screening RCTs. The dotted line is the diagonal line crossing the origin.
As shown in Supplemental Table 7, the concordance of statistical significance for the two endpoints in these trials was high. The majority of trials (26 out of 33) reported agreement in statistical significance, that is, statistically significant results for both endpoints or insignificant results for both.
Discussion
Despite substantial heterogeneity in geographic locations, screening populations, screening modalities, and cancer staging systems, among other factors affecting single-site cancer screening RCTs, we observed consistent, strong linear trends across multiple targeted cancer types between reductions in late-stage cancer incidence and reductions in cancer-specific mortality. While the number of large RCTs included for each cancer type was small, the degree of variability in mortality reduction explained by stage shift appeared to be at least moderately high: R2 was close to or greater than 0.9 among RCTs for lung, breast, and prostate cancers, and R2 = 0.93 for CRC trials when assessing stage IV. When pooling all 33 RCTs from seven different cancer types, meta-regression resulted in a strong linear increasing relationship between the two sets of screening effects, and a high overall R2 (0.75) after adjusting for cancer-specific slopes and intercepts.
Strengths of our analysis include the systematic identification and inclusion of all informative RCTs for single-cancer screening across multiple cancer types, and the weighted meta-regression approach yielding multiple statistical criteria to evaluate potential surrogacy; namely, R2, slope, and intercept. Our eligibility criteria allowed us to include 33 trials across seven different targeted cancer types. We built upon the rigorous inclusion criteria used by the USPSTF for including trials in evidence reviews, and included additional trials that met these criteria but had not been published in time for USPSTF consideration. Another strength of this analysis is that the primary analysis included only RCTs that were described as adequately powered to detect an effect on cancer-specific mortality. As illustrated in Figures 1 to 4, the larger dots, which represent RCTs with more mortality events, were more linearly aligned within the meta-regression line, whereas the smaller trials, such as the European LDCT trials, were more likely to be outliers. This phenomenon is particularly notable for the lung cancer and CRC trials, in that excluding the smaller trials resulted in a nearly perfect meta-regression line (Figures 1(B) and 2(B)).
The slope of the meta-regression line is a cancer-specific parameter, informing the degree of mortality reduction that could be attained per unit reduction of late-stage incidence. As shown by our simple stage-shift model, the slope is affected by the proportion of late-stage cancers and the relative mortality increment from early stage to late stage (Supplemental Materials). Therefore, the slope is expected to differ across cancer types. Further, if differing trials report differing definitions of late stage, the slope may also differ. The steepest slope in our analysis was 1.06 based on three large lung cancer screening trials, consistent with the pivotal lung cancer trial result from the NLST (20% reduction in stages III/IV cancers and 20% reduction in lung cancer mortality). 28 This finding is perhaps not surprising, given the high mortality of stages III and IV lung cancer. The slope was 0.84 in the breast cancer trials, which is qualitatively close to what was reported in previous meta-regression analyses.8,25 As noted before, 25 combining stages II/III/IV together as late-stage breast cancer did not account for stage migration within stages II-IV, for example, from stage IV to stage II, which also conferred a mortality benefit. Smaller slopes were observed for prostate cancer (slope = 0.45), based on analyses in which stage IV cancer was considered late-stage. Metastatic disease comprises a small proportion of prostate cancer yet carries the majority of the mortality burden for this malignancy; this may explain the moderate meta-regression slope.
Our results were more positive than those of Feng et al. 21 This is largely because the primary analysis of Feng and colleagues was based on the earliest reported mortality results; however, in their secondary analysis, using the most recent mortality figures from the trials with longer follow-up times, their results were more aligned with ours. To accurately estimate the mortality benefit of screening, long-term follow-up is necessary. 60 Thus, it is important to determine the predictive power of stage effects for long-term mortality. For example, in the European Randomised Study of Screening for Prostate Cancer at 13 years’ follow-up, there were 1.2 deaths prevented per thousand men randomized to screening. At 16 years, the number increased by 50% to 1.8.52,61
In contrast to Feng et al., we also allowed the definition of advanced stage to vary by cancer type. While reduction in stages III/IV cancers was generally associated with reduction in cancer mortality, the best measure of advanced stage for predicting mortality is likely to vary between cancers due to different biological mechanisms and consequences of early detection, depending on a number of observations, as elaborated in the Methods. These considerations can be evaluated from cancer registry data, thereby determining an appropriate definition of advanced stage for a cancer site. Figure 3 shows that the reduction in incidence of breast cancers of stage II or later is predictive of the reduction in cancer mortality, and gives an estimate of relative incidence that is considerably more precise than the estimate of relative mortality (forest plot). Supplemental Figure 4 indicates that the reduction in stage IV incidence may be predictive of the reduction in mortality, though the association is not significant. However, relatively few breast cancers are diagnosed at stage IV, so it is implausible that the effect on cancer mortality should be largely mediated via the effect on incidence of stage IV disease.
An additional difference between our analysis and that of Feng et al. is that theirs included two observational (non-randomized) FOBT studies:62,63 one “poor-quality” mammography trial 64 that USPSTF excluded from review due to “inadequate randomization” 65 and one trial of CBE published in 2021 66 that USPSTF did not consider in its 2023 draft evidence review for breast cancer screening. 67 Inclusion of these studies may have contributed to the discrepancy in findings between our analysis and that of Feng et al.
We had data from only two trials of ovarian cancer screening. In the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS), 57 there was a significant reduction in incidence of stage IV disease in one of the screened arms (RR = 0.75, 95% CI 0.57–0.97, p = 0.03), but no significant reduction in ovarian cancer mortality (RR = 0.96, 95% CI 0.83–1.10). This result may suggest that the reduction in the incidence of stage IV ovarian cancer is not a good predictor of the effect on cancer mortality, since only 23% of ovarian cancer deaths were from cancer that was stage IV at diagnosis. Given that 90% of cancer deaths were from stages III and IV disease combined, a better surrogate may be stages III–IV incidence (RR = 0.90, 95% CI 0.79–1.02). 68 Our results are consistent with this conjecture, showing a slope of dependence much closer to agreement for stages III and IV combined (Supplemental Figure 6). However, the effect of stage IV disease was not adjusted for multiple testing and there is considerable overlap of the CIs for the effects on stage IV cancer and on cancer mortality. It is therefore possible that the effect of screening even on stage IV disease is predictive of the effect on cancer-specific mortality in ovarian cancer.
Our analysis has several limitations. First, cancer screening trials represent a massive undertaking in cost and time; consequently, there are limited numbers of large RCTs for any particular cancer type, especially after further restriction to those with published results for clinical stage distribution. Therefore, the data points for our meta-regression analysis were sparse, for example, n = 3–4 for several analyses, weakening the robustness and generalizability of our results. Second, the heterogeneity of the design, screening modalities, population characteristics, and implementation of RCTs was substantial for some cancer types, which may obscure an underlying causal relationship. For example, CRC screening RCTs have been successful in proving the mortality benefit of flexible sigmoidoscopy and FOBT. These RCTs span in time from the mid-1970s to 2022, a long period during which treatment options have advanced. Furthermore, three cancer staging systems were used in these RCTs (UICC, Dukes’, and AJCC), which further complicated the meta-regression. We found that for FOBT trials, where the mechanism under study is mainly early detection of cancer, there is a stronger linear association and the effect on stage was closer to the effect on cancer mortality than for endoscopic trials (Supplemental Figure 3), where the mechanism is largely prevention of cancers of all stages.
Another limitation of our analysis is that reported trial-level summary data generally did not provide early read-out of the cancer stage distribution after the screening period, so it is not possible to estimate how much time advancement (lead time) a reduction in late-stage cancer incidence could provide as an early indicator for reduction in cancer mortality. Most trials reported data for the two endpoints after the same follow-up window, which was typically planned for observing the primary endpoint of mortality. Therefore, the reported data enabled us to analyze only the correlation of the two endpoints, yielding good trial-level evidence that no reduction in late-stage cancer incidence is strongly correlated with no mortality benefit at the same point in time. Individual-level trial data would be needed to assess the timing of late-stage cancer incidence as a potential early indicator of mortality reduction.
When summary data for cancer mortality and advanced disease across different breast cancer trials were used to estimate the proportional treatment effect explained, advanced stage incidence yielded a Freedman estimate of 67%. 25 Adopting this analytical strategy, we estimated the Freedman statistic for prostate, lung (LDCT), and CRCs as 100%, 62%, and 14%, respectively. The last pertains to all CRCs. For FOBT trials alone, the Freedman statistic for the logarithm of numbers of stage III and IV cancers was 77%, whereas for endoscopy trials it was 0%. We urge caution in interpreting these results as they are based on ecological (trial-level) rather than individual data.
Along these lines, if individual-level data from cancer screening RCTs were available, then further analyses could have been conducted to comprehensively evaluate late-stage cancer incidence as a potential surrogate for cancer-specific mortality. For example, one could evaluate the degree to which late-stage cancer incidence mediated the treatment effect on cancer mortality in NLST or PLCO, which are among a few trials that have made individual-level data publicly available to researchers by request. Caution would be needed to control for post-randomization selection bias when adjusting for cancer stages in a mediation regression model. Furthermore, screen-detected cancers may be inherently different from incident cancers arising in the control arm, such that it would be important to evaluate the degree to which cancer stage mediates the screening effect on cancer mortality.
The published literature to date includes RCTs of only single-cancer screening tests for a limited number of cancer types, so the results of this analysis are not necessarily generalizable to MCED tests. Nevertheless, our findings provide compelling theoretical and practical grounds to believe that the strong concordance between reduction in late-stage incidence and reduction in mortality holds across a spectrum of cancer types. An important observation of our analysis is that both the definition of late-stage cancers and the slope of trial-level association depend on cancer type. It remains a valuable future research topic, when data are available, to evaluate the generalizability of these results to an MCED trial, and potentially to define the most powerful composite measure of late-stage cancer incidence that combines multiple cancer types targeted by an MCED test. Another important area of research is the development of computational models calibrated to stage-specific incidence that could be used to predict the corresponding mortality reduction in a trial. Such models can enable “rigorous and transparent projections that may increase efficiencies and even eliminate the need for some trials.” 69 Nevertheless, from a conceptual standpoint, our analysis can be viewed as a preliminary but foundational work toward establishing broad surrogacy of reduction in late-stage cancer incidence for cancer-specific mortality: if a strong trial-level association has been found to hold across several individual cancer types, reduction of late-stage cancer incidence could be a reliable indicator of cancer-specific mortality across cancer types.
Conclusion
Across multiple cancer types, meta-regression of historical cancer screening RCTs showed a strong association between reduction in late-stage cancer incidence and reduction in cancer mortality. A reduction of late-stage cancer incidence may serve as an effective early indicator for mortality benefit in future cancer screening RCTs.
Supplemental Material
sj-docx-1-msc-10.1177_09691413241256744 - Supplemental material for Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types
Supplemental material, sj-docx-1-msc-10.1177_09691413241256744 for Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types by James Y Dai, E Georg Luebeck, Ellen T Chang and Christina A Clarke, Earl A Hubbell, Nan Zhang, Stephen W Duffy in Journal of Medical Screening
Supplemental Material
sj-xlsx-2-msc-10.1177_09691413241256744 - Supplemental material for Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types
Supplemental material, sj-xlsx-2-msc-10.1177_09691413241256744 for Strong association between reduction of late-stage cancers and reduction of cancer-specific mortality in meta-regression of randomized screening trials across multiple cancer types by James Y Dai, E Georg Luebeck, Ellen T Chang and Christina A Clarke, Earl A Hubbell, Nan Zhang, Stephen W Duffy in Journal of Medical Screening
Footnotes
Acknowledgements
The authors thank Randall Janairo (GRAIL, LLC) for help with manuscript development. Project management assistance was provided by Prescott Medical Communications Group (Chicago, IL). Editorial assistance was provided by Erin Spohr (ENGAGE Labs, LLC, Oak Ridge, NJ). All support and study funding were provided by GRAIL, LLC.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JYD, ETC, CAC, EAH, and NZ are employees of GRAIL, LLC, and report other support from GRAIL, LLC, during the conduct of the study. In addition, EAH has multiple patents in the field of cancer detection pending to GRAIL, LLC. EGL reports receiving consulting fees from GRAIL, LLC.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the GRAIL, LLC,
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.