
Abstract
Objective
Many population-based breast screening programmes temporarily suspended routine screening following the COVID-19 pandemic onset. This study aimed to describe screening mammography utilisation and the pattern of screen-detected breast cancer diagnoses following COVID-19-related screening disruptions in Ireland.
Methods
Using anonymous aggregate data from women invited for routine screening, three time periods were examined: (1) January–December 2019, (2) January–December 2020, and (3) January–December 2021. Descriptive statistics were conducted and comparisons between groups were performed using chi-square tests.
Results
In 2020, screening mammography capacity fell by 67.1% compared to 2019; recovering to 75% of mammograms performed in 2019, during 2021. Compared to 2019, for screen-detected invasive breast cancers, a reduction in Grade 1 (14.2% vs. 17.2%) and Grade 2 tumours (53.4% vs. 58.0%) and an increase in Grade 3 tumours (32.4% vs. 24.8%) was observed in 2020 (p = 0.03); whereas an increase in Grade 2 tumours (63.3% vs. 58.0%) and a reduction in Grade 3 tumours (19.6% vs. 24.8%) was found in 2021 (p = 0.02). No changes in oestrogen receptor-positive or nodal-positive diagnoses were observed; however the proportion of oestrogen/progesterone receptor-positive breast cancers significantly increased in 2020 (76.2%; p < 0.01) and 2021 (78.7%; p < 0.001) compared to 2019 (67.8%).
Conclusion
These findings demonstrate signs of a grade change for screen-detected invasive breast cancers early in the pandemic, with recovery evident in 2021, and without an increase in nodal positivity. Future studies are needed to determine the COVID-19 impact on long-term breast cancer outcomes including mortality.
Introduction
The COVID-19 pandemic has had many indirect health impacts globally including the temporary suspension of many organised breast screening programmes (BSPs) for various time periods. 1 Breast cancer screening aims to reduce breast cancer mortality 2 and, depending on the organised BSP, asymptomatic women are typically invited for biennial mammography screening. In response to the public health and government healthcare strategies adopted by individual countries and jurisdictions in March 2020, suspension of routine breast screening occurred and the length of disruption varied internationally ranging from one month to six months, depending on the public health advice in each country. 3
While the long-term impact of the pandemic on breast cancer incidence and mortality has yet to be fully realised, early modelling studies 3 were conducted to determine the impact of the pandemic on programme activity and outcomes across countries including Australia, 4 Canada, 5 Italy, 6 the Netherlands, 7 and the United Kingdom, 8 with some studies suggesting that pauses to organised BSPs may lead to excess mortality. 3 A modelling analysis from Scotland, using the stage-shift model, showed predicted excess mortality of 6.3% and 22.3% following three- and six-month screening disruptions. 3 Modelling studies from the United States showed similar findings. 9 A recent meta-analysis of retrospective cohort studies by Ng and Hamilton that examined the impact of the pandemic on breast cancer screening outcomes found that screening mammography declined in 2020 compared to 2019 by 41% (RR: 0.59, 95% CI: [0.46–0.75]) in studies using data from national registries and by 53% (RR: 0.47, 95% CI: [0.38–0.58]) in studies using non-registry-based data. 10 Additionally, they reported a decrease in the number of early-stage breast cancer diagnoses compared to late-stage breast cancer diagnoses over the same time period. 10
Following the onset of the COVID-19 pandemic, the national population-based BSP in Ireland paused routine breast screening between March and October 2020, and in January 2021 for a further two months. This was in response to public health advice that necessitated the temporary suspension of non-COVID-19-related healthcare services due to the high COVID-19 infection rates nationally and the subsequent increased demand for acute hospital services and bed capacity. 11 In particular, during these COVID-19 waves, there was increased demand for intensive care bed capacity. 12 In Ireland, at the BSP level, the standard care pathway begins at the point of screening mammography and continues up to the point when surgery is completed for women diagnosed with screen-detected breast cancer. Therefore, as elective or non-urgent surgeries within the hospitals were unable to go ahead due to public health advice, the national BSP was unable to continue with routine services during these time periods as access to operating theatres for women diagnosed with screen-detected breast cancer was limited. 11 Given that Ireland, like other countries, experienced subsequent COVID-19 waves, 13 this study aimed to examine the impact of the COVID-19-induced breast screening suspensions on patterns of breast screening and screen-detected breast cancer diagnoses during 2020 and 2021 compared to 2019. Further, this study aimed to build upon existing literature and contribute to our understanding of the impact of breast screening suspensions on screen-detected breast cancer diagnoses and tumour characteristics.
Methods
Study design
A repeated cross-sectional study design was used. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies. 14
Study population
BreastCheck is the national population-based BSP in Ireland that invites eligible asymptomatic women aged 50–69 years for free biennial mammography screening, via letter, at age 50 years and subsequently at the time of their 24-month screening interval. 15 In March 2020, following the declaration by the World Health Organization of the COVID-19 pandemic and upon national governmental public health restrictions, BreastCheck routine screening for asymptomatic women was paused. The service was suspended initially from March to October 2020 and from January to February 2021. During these time periods, screening units maintained the provision of the standard care pathway including follow-up assessments, further work-up, and surgery as required for women recalled following abnormal or positive screening mammograms that took place prior to the pandemic and pausing of the screening programme. 16 Furthermore, when the screening programme was suspended, BreastCheck staff including radiographers and consultant radiologists were temporarily redeployed to support hospital-based symptomatic breast services through the provision of imaging services and assessment clinics for women referred for assessment to symptomatic services by their general practitioners. 16 The provision of these services at screening units ceased once screening resumed after each suspension, and women presenting with breast symptoms attended hospital-based symptomatic breast clinics for their assessment and review as was standard prior to the pandemic.
Upon resumption of screening after each suspension, screening capacity continued to be limited to enable adherence to COVID-19 restrictions including physical distancing. Several operational measures were taken by the programme upon resumption to maximise screening appointments and to minimise the number of people passing through the screening units, to reduce the risk of COVID-19 exposure to staff and screening participants. Prior to the pandemic, both initial and subsequent women were invited for their scheduled screening appointment via letter.15,17,18 ‘Initial women’ comprised of women invited to attend for their first screening mammogram and those who were previously invited but did not attend (also known as previous non-attenders, PNAs). ‘Subsequent women’ comprised of women invited to attend for their second or subsequent screening mammogram. On restarting screening after each COVID-19-related suspension, eligible subsequent women who previously attended their screening appointment continued to receive a scheduled appointment via letter and were able to reschedule their appointment if they wished, while PNAs were sent an invitation letter without a fixed appointment that invited them to contact the programme to schedule an appointment at their convenience. Invitations were prioritised based on time since last appointment, therefore subsequent women with the longest time since their last appointment were invited back first upon restarting screening. 16 In the early phases of the programme resuming routine breast screening, initial invitations for women entering the programme started at women aged 51 years and above. These invitation strategies aimed to minimise the number of missed appointments 19 and reduce the length of time between screens for BreastCheck participants, while at the same time ensuring a steady throughput of new participants to the programme. Examples of other COVID-19 infection control measures included the use of telephone consultations for women who were receiving benign results. Prior to the pandemic, these women would have received these results at an in-person consultation.
Data ascertainment
This study used anonymised aggregate data from the National Screening Service. Women who participate in BreastCheck provide signed informed consent at each screening appointment for their demographic data, screening mammograms, and outcome data to be used for audit and quality assurance purposes in accordance with the General Data Protection Regulation. Ethical approval was not required as this study was a screening service evaluation. Three study periods, January–December 2019, 2020, and 2021, were examined as shown in Figure 1.
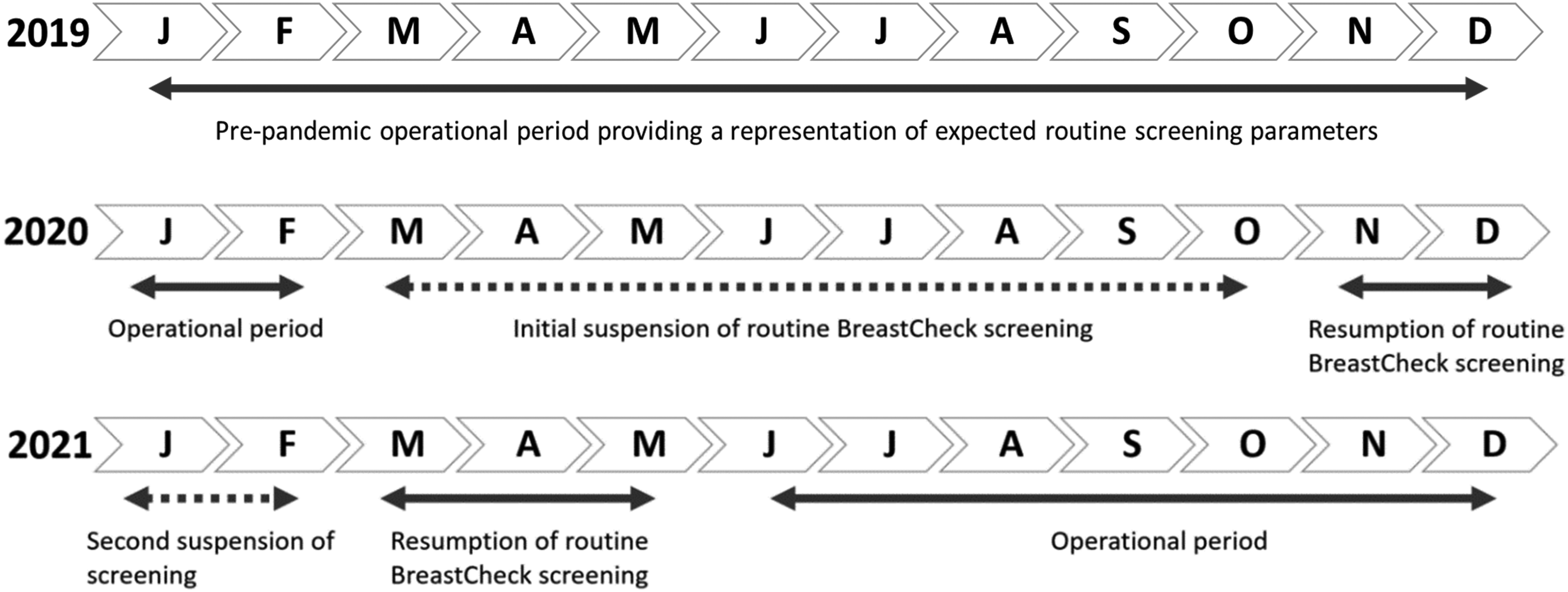
Detailed description of the three study periods examined. A solid line arrow indicates operational periods and dashed line arrows indicate periods where routine BreastCheck screening was suspended (developed for and adapted from the screening programme Statistical Report 20 ).
Statistical analysis
To examine screening mammography utilisation, the aggregated monthly number of screening mammograms was determined. Mammograms performed as part of follow-up recall assessments were not included in this analysis. To examine patterns of screen-detected breast cancer diagnoses and radiological performance indicators, the aggregated number of screen-detected breast cancers diagnosed within the programme and their tumour characteristics over the specified time periods were determined. This analysis included all women with a screen-detected breast cancer diagnosis defined as ductal carcinoma in situ (DCIS) or an invasive breast cancer diagnosed among asymptomatic women aged 50–69 years who participated in the programme. Furthermore, women aged 69 years who missed their final mammogram due to the screening suspensions in 2020 or 2021 were offered their final mammogram upon resumption of screening, therefore any woman that availed of this limited service and was aged 70 or over at diagnosis are also included in this analyis. 21 Descriptive statistics were used to describe patterns of mammography uptake, radiological performance indicators, and tumour characteristics of screen-detected breast cancers for the study periods. Screening attendance is defined as ‘the number of women recorded as having a complete screening visit within a specified date range’. 17 Radiological performance indicators examined included: (1) recall rate defined as ‘the number of women recalled to assessment as a percentage of the women screened (to date)’, (2) cancer detection rate defined as ‘the number of women with a malignant result(s) per thousand women screened’, and (3) positive predictive value (PPV) defined as ‘the number of women diagnosed with breast cancer as a proportion of the number of women ‘recalled to assessment’ following their screening mammogram’. 17 Tumour characteristics examined included: (1) DCIS grade categorised as low, intermediate, high, or not assessable, (2) invasive grade categorised as Grade 1, Grade 2, Grade 3, or Grade not assessable, (3) nodal status categorised as positive, negative, or missing, (4) human epidermal growth factor receptor 2 (HER2) status categorised as positive, negative, or missing, (5) oestrogen receptor (ER) status categorised as positive, negative, or missing, and (6) oestrogen/progesterone receptor (ER/PR) status categorised as positive (i.e., tumours that are both ER-positive and PR-positive), negative (i.e., tumours that are ER-positive and PR-negative or ER-negative and PR-positive), or missing. Chi-square tests were used to compare categorical data across groups, including study periods. Results are presented for the screened population overall and stratified by attendance status (initial and subsequent attendance). Statistical tests were two-sided and p < 0.05 was considered statistically significant. Data where n < 7 are not presented and do not contribute to total values or percentages. Similarly, if the grade was not assessable for DCIS or invasive breast cancer, these data also do not contribute to total values or percentages. Stata 17.0 software was used to conduct the statistical analysis. 22
Results
During 2019, the total absolute number of screening mammograms performed was 170,959 (Figure 2A). In 2020, mammograms performed fell by 67.1% to 56,270, following the suspension of routine mammography screening between March and October. In 2021, the number of screening mammograms increased to 127,290, recovering to approximately 75% of the 2019 volume, despite the suspension of routine screening between January and February. Among women screened in 2019, 14.6% (n = 24,907) were initial attenders and 85.4% (n = 146,052) were subsequent attenders. The absolute number of screening mammograms performed for initial attenders was lower during both recovery periods in 2020 and 2021, due to restarting strategies outlined previously in the methods; however, the monthly volume was in line with pre-pandemic levels by July 2021 (Figure 2B). For subsequent attenders, the number of screening mammograms per month were similar in December 2020 and April–December 2021 as those reported for the same months in 2019, with some variation in the numbers of screening mammograms performed per month noted in June–August 2021 compared to these months in 2019 (Figure 2C).
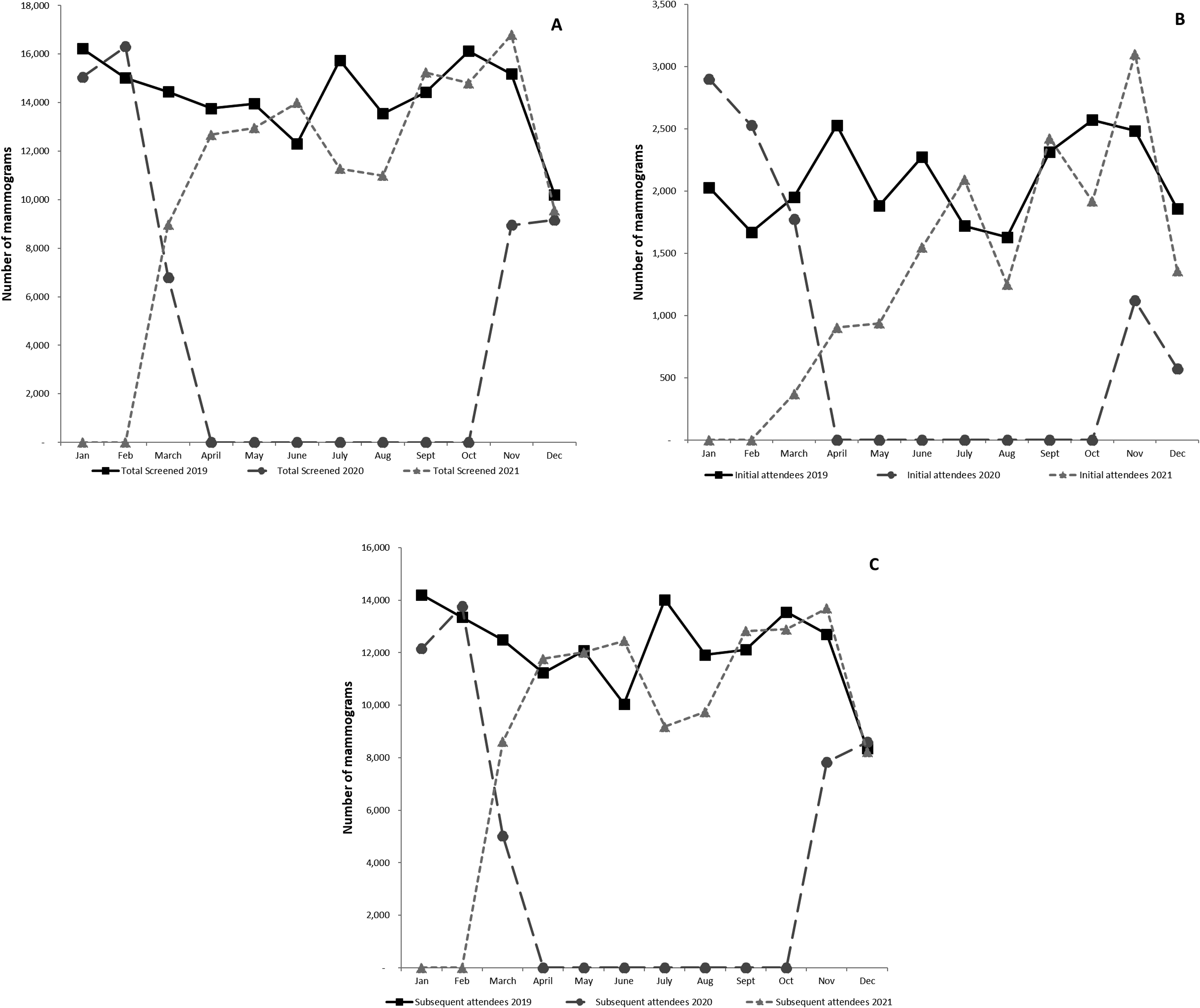
The absolute number of screening mammograms per month performed during 2019, 2020, and 2021 for (A) all, (B) initial, and (C) subsequent attendees of the population-based breast screening programme in Ireland. Routine mammography screening was suspended between March and October 2020 and in January–February 2021.
Patterns of attendance were examined for women invited during the study periods January–December 2019, 2020, and 2021 (Table 1). While the absolute numbers of women who were invited and attended were lower in 2020 and 2021, higher proportions of women attended routine breast screening in 2020 (74.4%) and 2021 (74.8%) compared to 2019 (71.6%). In 2021, a lower proportion of eligible women received invitations to enter the screening programme for their initial screening appointment, while a higher proportion of eligible women were invited to return for their second or subsequent screening appointment compared to 2019 and 2020. The uptake rate varied for initial invitees with higher uptake rates observed in 2020 (41.8%) and 2021 (38.2%), compared to 2019 (35.8%). Similar uptake rates were observed for subsequent invitees across the three study periods. Similar patterns were observed among women who were invited but did not attend for their first screening appointment and those who did not attend for their second or subsequent screening appointments across the three study periods.
Invitations and uptake rates among women invited in 2019, 2020, and 2021 to participate in the population-based breast screening programme in Ireland.
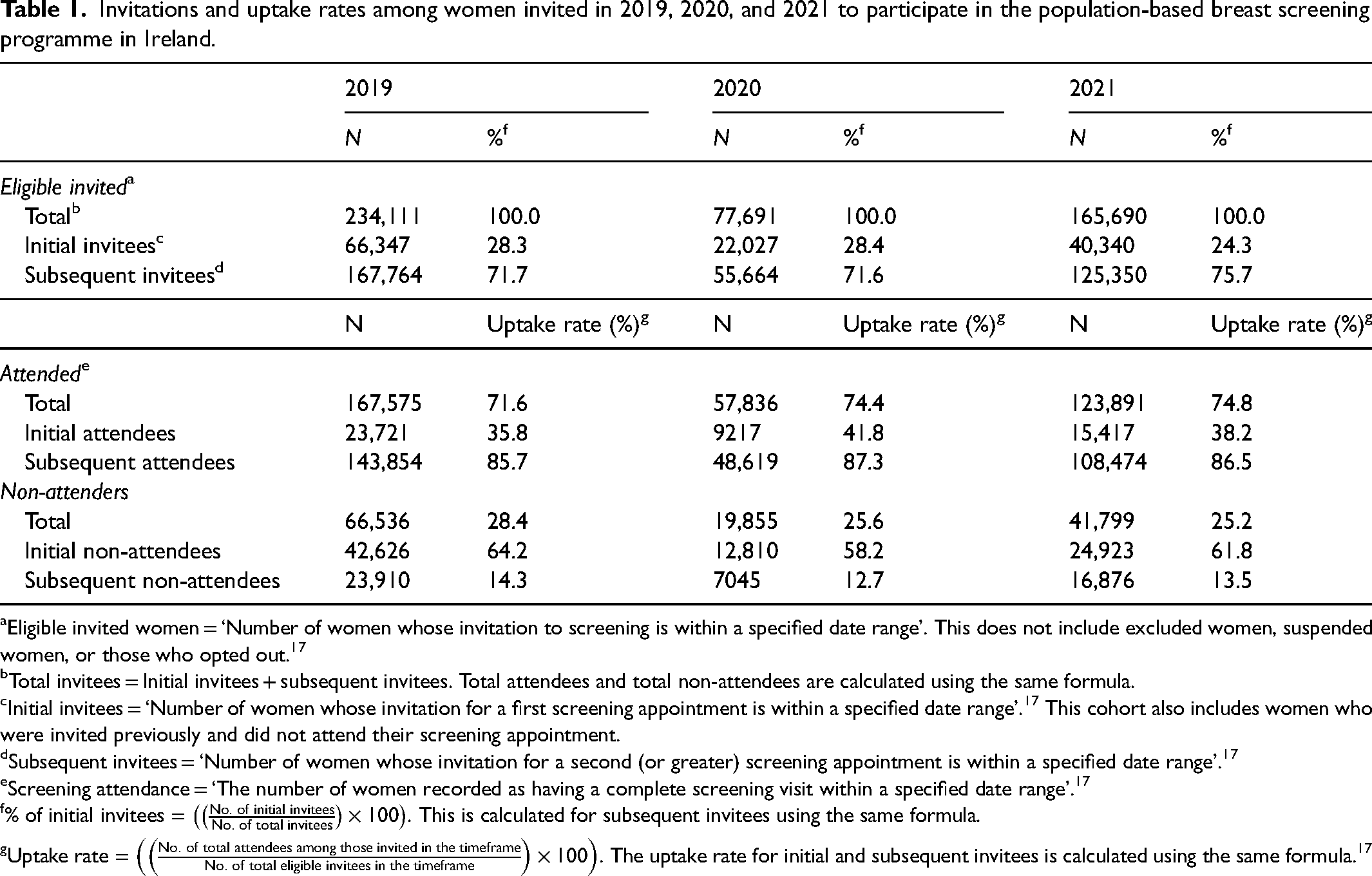
Eligible invited women = ‘Number of women whose invitation to screening is within a specified date range’. This does not include excluded women, suspended women, or those who opted out. 17
Total invitees = Initial invitees + subsequent invitees. Total attendees and total non-attendees are calculated using the same formula.
Initial invitees = ‘Number of women whose invitation for a first screening appointment is within a specified date range’. 17 This cohort also includes women who were invited previously and did not attend their screening appointment.
Subsequent invitees = ‘Number of women whose invitation for a second (or greater) screening appointment is within a specified date range’. 17
Screening attendance = ‘The number of women recorded as having a complete screening visit within a specified date range’. 17
% of initial invitees =
Uptake rate =
Among women who were screened, the percentage of women recalled for assessment in 2019 was 4.1%. While the absolute numbers of women recalled were lower during 2020 and 2021 compared to 2019, the percentage of women recalled was similar for 2020 (4.7%) and 2021 (4.9%) (Table 2).
Radiological performance indicators and tumour characteristics of screen-detected breast cancers diagnosed among women screened in 2019, 2020, and 2021.
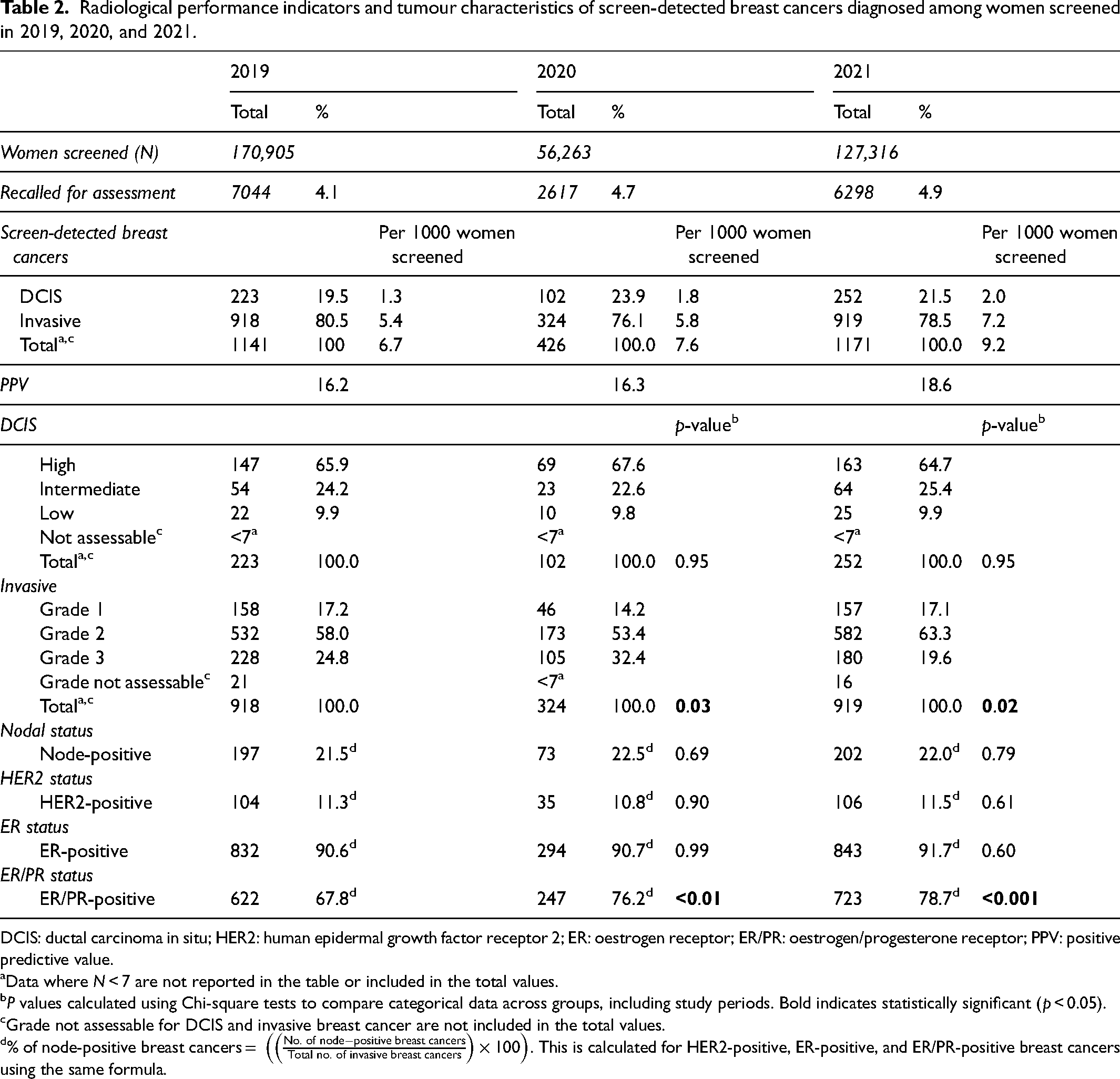
DCIS: ductal carcinoma in situ; HER2: human epidermal growth factor receptor 2; ER: oestrogen receptor; ER/PR: oestrogen/progesterone receptor; PPV: positive predictive value.
Data where N < 7 are not reported in the table or included in the total values.
P values calculated using Chi-square tests to compare categorical data across groups, including study periods. Bold indicates statistically significant (p < 0.05).
Grade not assessable for DCIS and invasive breast cancer are not included in the total values.
% of node-positive breast cancers =
Among the breast cancers detected in 2019, 80.5% (n = 918) were invasive and 19.5% (n = 223) were DCIS. In 2020, 76.1% were invasive (n = 324) and 23.9% were DCIS (n = 102). Similar patterns were observed in 2021 (Table 2). The cancer detection rate for all screen-detected breast cancers was higher in 2021 (9.2 per 1000 women screened) compared to 2019 (6.7 per 1000 women screened) and 2020 (7.6 per 1000 women screened). The PPV was 16.2% in 2019, 16.3% in 2020, and 18.6% in 2021.
In 2019, 65.9% of DCIS detected were high grade (n = 147), 24.2% were intermediate grade (n = 54) and the remaining 9.9% were low grade (n = 22) (Table 2). Though the absolute number diagnosed was smaller in 2020, similar patterns of distribution were observed for 2020 and 2021.
Of the invasive breast cancers diagnosed in 2020, compared to 2019, lower proportions of Grade 1 (14.2%, n = 46 vs. 17.2%, n = 158) and Grade 2 (53.4%, n = 173 vs. 58.0%, n = 532) and a higher proportion of Grade 3 (32.4%, n = 105 vs. 24.8%, n = 228) invasive breast cancers were detected (p = 0.03) (Table 2). Compared to 2019, a similar proportion of Grade 1 (17.1%, n = 157 vs. 17.2%, n = 158), a higher proportion of Grade 2 (63.3%, n = 582 vs. 58.0%, n = 532), and a lower proportion of Grade 3 (19.6%, n = 180 vs. 24.8%, n = 228; p = 0.02) invasive breast cancers were observed in 2021.
No difference in patterns of node-positive cancers or HER2-positive cancers were observed across the study periods. Similarly, no difference in the proportion of invasive breast cancers that were ER-positive was found, with 90.6% (n = 832) diagnosed in 2019, 90.7% (n = 294) in 2020, and 91.7% (n = 843) in 2021 (Table 2). Compared to 2019 (67.8%, n = 622), higher proportions of ER/PR-positive breast cancers were diagnosed in 2020 (76.2%, n = 247; p < 0.01) and 2021 (78.7%, n = 723; p < 0.001).
Discussion
Similar to other international programmes, the national BSP in Ireland was paused following the onset of the COVID-19 pandemic. 3 This study showed that following COVID-19-related screening suspensions, screening mammography volume had recovered to pre-pandemic levels during 2021. Women attended routine breast screening appointments in 2020 and 2021 at levels higher than those observed in 2019. As anticipated, a pause in screening resulted in a reduced number of screen-detected breast cancers. Of the screen-detected breast cancers diagnosed, no differences in the distribution of DCIS and invasive breast cancer were found in 2020 or 2021 compared to 2019. While findings from this study demonstrated differences in the grading distribution and an increase in ER/PR positivity among screen-detected invasive cancers diagnosed following the pandemic onset, no change in nodal positivity or HER2 status was observed.
Our findings demonstrate the reduction and recovery of screening mammography volume reflecting the suspension and resumption of screening in Ireland in 2020 and 2021 following the pandemic onset. These findings are consistent with those from a recent systematic review that found screening mammography volume reduced to ≥49% during the pandemic in more than 50% of included studies. 23 For studies with time periods beyond the initial peak of the pandemic (March–May 2020), Li et al. observed the gradual recovery of screening mammography volume. 23 This temporal pattern was also identified by Teglia et al. for breast cancer screening settings across North America, South America, and Europe. 24 The impact of the pandemic on mammography volume differed internationally due to variations in public health guidance 25 with BSPs suspending screening for differing lengths of time 3 and adopting different approaches to restarting.
We found the uptake rate for initial invitees varied slightly across the three study periods, increasing to 41.8% and 38.2% in 2020 and 2021 respectively, compared to 35.8% in 2019. This variation can be attributed to changes to invitation policies adopted by the programme to address and overcome the backlog created by the COVID-19 pandemic and maximise resource use within the screening programme. Women with the longest time since their last appointment were prioritised upon the resumption of screening in November 2020. In 2021, the programme began to invite increased numbers of eligible initial invitees and PNAs for routine breast screening. Prior to the pandemic, PNAs were offered a fixed scheduled appointment. However, to maximise screening attendance upon the resumption of screening, PNAs were sent an invitation letter and invited to contact the programme to schedule an appointment. An intervention trial previously conducted by Fleming et al. 19 that piloted this invitation strategy for PNAs on the BreastCheck programme demonstrated that while uptake was lower for this open invitation strategy compared to offering a scheduled appointment, this strategy reduced the number of missed appointments and the length of time between screens for screening participants. In Spain, the population-based BSP modified their invitation strategy to a telephone-based strategy to schedule appointments and found that women who received an invitation for their first or subsequent screening mammogram were less likely to participate in the COVID-19 period (March 2020 - March 2021) compared to the pre-COVID-19 period (four two year periods beginning in March 2012 and ending in March 2019). 26 While in the United Kingdom, a similar open invitation approach was adopted by the NHS BSP where women were invited to select their appointment time upon the restarting of screening. 27 Within a modelling study, Duffy et al. 27 examined this recovery approach while also estimating the impact of changes to round length on the number of cancers detected. Their analysis found that prioritising improved uptake of screening appointments, supporting the use of scheduled appointments where possible, may provide more benefit to cancer detection within the NHS screening population in the United Kingdom. 27
In agreement with studies internationally,10,23,28–31 a reduction in the number of screen-detected breast cancers was observed in 2020. In this analysis, no significant differences were observed in the proportions of DCIS and invasive breast cancers diagnosed in 2020 or 2021, compared to 2019. However, among women screened in 2021, the DCIS detection rate (2.0 per 1000 women screened) and invasive cancer detection rate (7.2 per 1000 women screened) were higher compared to 2019. While similar grading distribution patterns for DCIS were observed across the three study periods, differences in the grading distribution of invasive breast cancers were observed. A study within a northern province of Italy comparing breast cancer characteristics between 2019 and 2020, capturing a breast screening suspension in March–May 2020, reported no grade change for invasive breast cancers. 32 Our study found no difference in the proportion of cancers that were node-positive following the suspension of screening in 2020 and 2021 which is in contrast to an early study by Toss et al. 33 examining the impact of a 2-month screening suspension on breast cancer characteristics between May and July 2020 compared to the same time period in 2019. They observed a significant increase in the number of node-positive breast cancers (approximately 11%) in their institution. 33 However, updated findings for the same institution from May to July 2021 showed the number of node-positive cancers decreased compared to the same time period in 2020. 34 Unlike our findings, which showed no change in ER status but an increase in ER/PR-positive cancers, Tonneson et al. reported no significant change in the proportions of ER-positive, PR-positive, or hormone receptor-positive breast cancers. Their study captured an early pandemic time period (March–August 2020) and was set in a single U.S. institution, which may not be fully comparable with that of a population-based BSP. 35 While stage data were not examined in this study, recent data from the screening programme in the Netherlands show that the relative stage distribution in 2021 and early 2022 for DCIS, Stage I and Stage II breast cancers was similar to the distribution seen in 2017–2019; the distribution for Stage III and Stage IV breast cancers was more varied for the same time periods.28,31 Findings from a systematic review by Li et al. also reported lower proportions of early-stage breast cancer and, subsequently, higher proportions of more advanced-stage breast cancer diagnosed during the pandemic period, March and September 2020. 23 These differences in findings may relate to several factors, including variations in the timeline of the pandemic impact period assessed, the study setting, the burden of COVID-19 within the population examined, country-specific restrictions, length of screening suspensions, and recovery strategies used.
In an effort to determine the potential long-term impact of the pandemic and inform service requirement discussions, using a modelling approach, Duffy et al. 36 estimated the number of delayed breast cancers diagnosed and resultant breast cancer deaths in the United Kingdom, accounting for COVID-19-related backlogs in screening and screening recovery periods. Their modelling analysis reported a projected increase of 148–687 breast cancer deaths over 10 years due to the suspension of screening. 36 A recent study by Poelhekken et al. modelled the impact of 3-, 6-, and 12-month screening interruptions on the BSP in the Netherlands. Their study found a three-month screening disruption did not impact tumour size for screen-detected breast cancers. The modelling results also predicted a 20% increase in the interval cancer rate between the last screening phase before the disruption and the first screening phase upon the resumption of screening. 37
Strengths of this study include the expanded study period from 2019 to 2021 allowing for the investigation of the cumulative impact of multiple waves of the pandemic. This study included the population-based BSP in Ireland and is representative of the COVID-19 impact at the population level in contrast to other studies that focused on a single institution or a hospital-based setting. However, the limitations of this study must be acknowledged. Firstly, this analysis did not account for other factors outside the setting of the pandemic that may have influenced screening and cancer detection patterns. Our study focused on data from the screening programme only and did not include breast cancers detected outside of the population-based BSP. Further analyses of national cancer registry data will be needed to validate and explore the present study findings.
Continued efforts are ongoing to mitigate the impacts of the pandemic and ensure the screening backlog is eliminated. In line with current screening capacity, the programme continues to invite women for routine breast screening, with an aim to return to pre-COVID-19 policies such as offering fixed appointments for all women.
In conclusion, this study provides an initial insight into the impact of the COVID-19 pandemic on the national population-based BSP in Ireland. It will take some time before the long-term impact of the pandemic on cancer-related healthcare and services is fully realised. Future research over extended time periods will be needed to decipher the impact on breast cancer prognostic characteristics, including mortality.
Footnotes
Authors’ Notes
Fidelma Flanagan and Maeve Mullooly are joint senior authors.
Author contributions
Jessica O’Driscoll: formal analysis, investigation, writing – original draft, writing – review and editing, visualisation, and project administration; Therese Mooney: investigation, validation, data curation, writing – review and editing, and visualisation; Paul Kearney: data curation, investigation, validation, and writing – review and editing; Yvonne Williams: data curation and writing – review and editing; Suzanne Lynch: writing – review and editing; Alissa Connors: writing – review and editing; Aideen Larke: writing – review and editing; Sorcha McNally: writing – review and editing; Ann O’Doherty: writing – review and editing; Laura Murphy: writing – review and editing; Kathleen Bennett: conceptualisation, methodology, validation, formal analysis, writing – review and editing, and supervision; Patricia Fitzpatrick: conceptualisation, investigation, methodology, and writing – review and editing; Maeve Mullooly: conceptualisation, investigation, methodology, writing – original draft, writing – review and editing, supervision, and project adminisatration; Fidelma Flanagan: conceptualisation, investigation, methodology, writing – review and editing, and supervision.
Data availability
The anonymised aggregate data were provided by the National Screening Service. For queries regarding this data, please contact the National Screening Service at info@screeningservice.ie.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MM/JOD are supported by funding from the Health Research Board.